Introduction: Where BPC-157 Comes From Is Where It Works Best
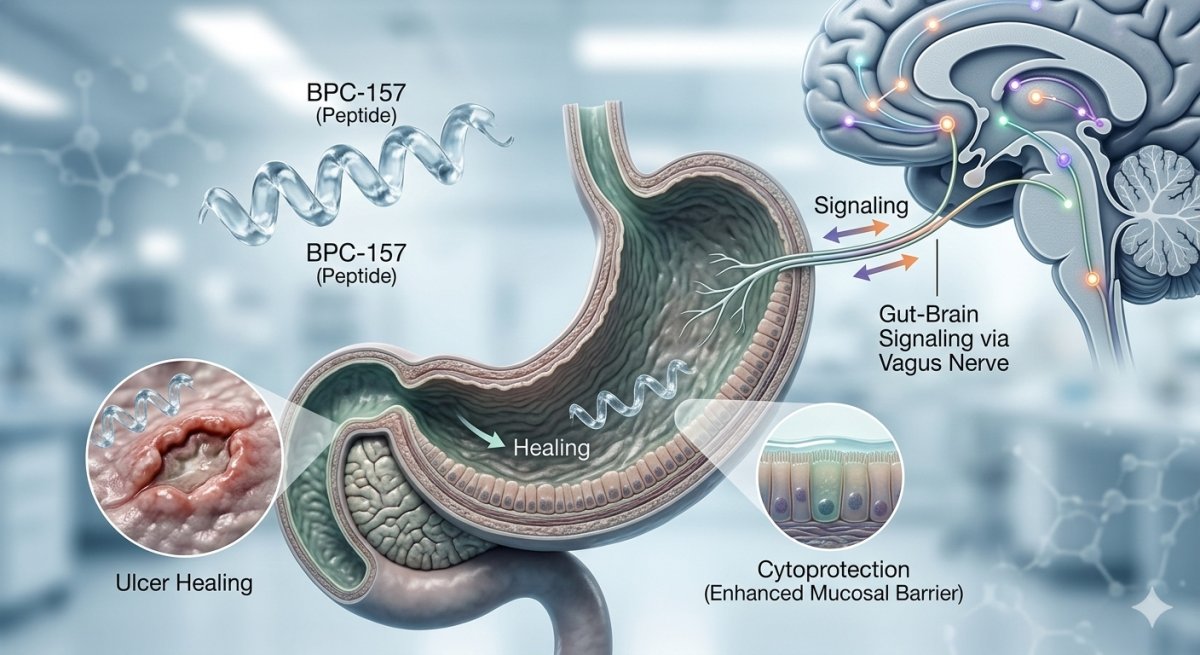
The gastrointestinal tract is not merely one of many systems where BPC-157 has been studied — it is the peptide's native domain, the biological context from which it was originally isolated, and the research area supported by the deepest and most differentiated body of evidence. BPC-157 was discovered as a fragment of a protective protein in human gastric juice, and its extraordinary stability in the acidic gastric environment is a direct reflection of this origin.[1]
Understanding BPC-157's gastrointestinal effects provides essential context for interpreting its broader pharmacology. The cytoprotection concept — the theoretical framework that unifies BPC-157's diverse tissue effects — was first articulated in the stomach, and the peptide's clinical trial history began with gastrointestinal indications. This article examines BPC-157's GI research in detail. For general background on the peptide, see our pillar article on what BPC-157 is. For the molecular pathways underlying these effects, see our mechanism of action article.
The Cytoprotection Concept
Robert's Original Framework
The concept of gastric cytoprotection was first described by André Robert in 1979, demonstrating that prostaglandins could protect gastric mucosal cells from damage by various noxious agents at doses too low to inhibit acid secretion. This observation established that the stomach possesses active cellular defense mechanisms beyond the mechanical mucus-bicarbonate barrier. The concept was subsequently extended to "adaptive cytoprotection" — the observation that mild irritants could induce a protective response against subsequent stronger challenges.[2]
BPC-157 as Cytoprotection Mediator
Sikiric and colleagues have positioned BPC-157 as a novel endogenous mediator of Robert's cytoprotection concept. The rationale is compelling: BPC-157 is native to human gastric juice, stable in the gastric environment, and demonstrates cytoprotective effects that exceed those of standard anti-ulcer agents including cimetidine, ranitidine, omeprazole, and atropine in several experimental assays.[2] The cytoprotection framework was progressively expanded from stomach cell protection to endothelium protection, and ultimately to the control of blood vessel function — three interconnected levels that BPC-157 addresses simultaneously.
From this gastric foundation, BPC-157 research extended to the concept of "organoprotection" — the hypothesis that the same cytoprotective mechanisms operating in the stomach could be generalized to other organs. This conceptual progression from cytoprotection to organoprotection provides the theoretical bridge between BPC-157's GI effects and its documented activity in musculoskeletal, vascular, and neurological systems.[2]
Gastric and Duodenal Ulcer Healing
Ethanol-Induced Gastric Lesions
Acute ethanol administration is a standard method for inducing gastric mucosal injury in experimental models. Ethanol causes direct epithelial cell damage, disrupts the mucosal barrier, impairs microcirculation, and triggers an inflammatory cascade. BPC-157 demonstrates potent protective effects against ethanol-induced lesions, both when administered prophylactically (before ethanol challenge) and therapeutically (after lesion establishment). The protective effect has been observed with both parenteral and oral administration routes, consistent with the peptide's systemic bioavailability and gastric stability.[3]
Cysteamine-Induced Duodenal Ulcers
Cysteamine administration produces duodenal ulcers through a mechanism long thought to be exclusively acid-dependent. In an innovative experimental design, Sikiric and colleagues demonstrated that BPC-157's cytoprotective effect persisted even in totally gastrectomized rats — animals lacking a stomach and therefore lacking gastric acid — challenging the assumption that cysteamine toxicity is solely acid-mediated. BPC-157 at doses of 10 μg/kg or 10 ng/kg administered intraperitoneally significantly reduced duodenal lesion severity in this acid-free model, supporting a direct cytoprotective mechanism independent of acid suppression.[4]
Chronic Ulcer Models
Beyond acute lesion models, BPC-157 has demonstrated efficacy in chronic ulcer healing, including acetic acid-induced chronic gastric ulcers. Both intragastric and intramuscular administration improved chronic ulcer healing outcomes. The peptide's effect on chronic ulceration is particularly relevant because chronic ulcers present a more clinically representative healing challenge, involving sustained inflammation, fibrosis, and impaired angiogenesis that acute models do not fully capture.[1]
NSAID-Induced Gastrointestinal Injury
Non-steroidal anti-inflammatory drugs (NSAIDs) cause gastrointestinal damage through both topical irritation and systemic inhibition of prostaglandin synthesis. NSAID gastropathy is a major clinical problem, and the development of protective agents that do not compromise NSAID efficacy is an active area of pharmacological research. BPC-157 has shown notable effects in NSAID-injury models.[5]
Indomethacin-Induced Lesions
Indomethacin, a potent non-selective COX inhibitor, produces gastric erosions that model the clinical gastropathy associated with chronic NSAID use. BPC-157 prevents the formation of indomethacin-induced gastric lesions and promotes healing of established lesions. Importantly, the peptide appears to achieve this protection without interfering with NSAID-mediated anti-inflammatory effects, suggesting a mechanism distinct from prostaglandin replacement.[5]
Broader NSAID Toxicity Counteraction
BPC-157's protective effects extend beyond the gastric mucosa to other organ systems affected by NSAID toxicity. In models of NSAID-induced hepatotoxicity, encephalopathy, and systemic inflammatory injury, BPC-157 attenuated multi-organ damage while maintaining or restoring GI tract integrity. This broad counteraction of NSAID adverse effects further supports the cytoprotection-to-organoprotection conceptual framework and distinguishes BPC-157 from conventional gastroprotective agents whose effects are limited to the gastric mucosa.[5]
Inflammatory Bowel Disease Models
Preclinical Evidence
BPC-157 has been studied in multiple IBD-relevant models, including trinitrobenzene sulfonic acid (TNBS)-induced colitis, acetic acid-induced colitis, and dextran sodium sulfate (DSS)-induced colitis. The peptide reduces inflammatory cell infiltration, preserves mucosal architecture, and promotes healing of colonic lesions across these models. Its effects include reduced inflammatory cytokine expression, preserved intestinal barrier function, and improved macroscopic and histological disease scores.[6]
Ischemia-Reperfusion Colitis
A particularly informative model involves ischemia-reperfusion injury to the colon, induced by temporary ligation of the left colic artery and vein. BPC-157 exerted rapid cytoprotective endothelium rescue, restoring blood flow by activating collateral vessel pathways and bypassing the obstructed vessels. The peptide normalized nitric oxide levels and reduced malondialdehyde (a marker of oxidative stress) in colonic tissue, and these effects were maintained even over the NO-system background when pharmacologically manipulated with L-NAME or L-arginine.[7]
The ischemia-reperfusion colitis model is significant because it demonstrates BPC-157's vascular recruitment capacity in the GI tract — the same mechanism that underlies its protective effects in other vascular beds. The colon is particularly susceptible to insufficient vascular perfusion, and BPC-157's ability to rapidly bypass obstructions through arcade vessel activation may represent a critical component of its GI cytoprotective mechanism.
Clinical Trial Status
BPC-157 has been tested in Phase II clinical trials for ulcerative colitis under the designations PL-10, PLD-116, and PL 14736, conducted by the pharmaceutical company Pliva. The peptide demonstrated a safe profile in these trials, with no side effects reported. While detailed efficacy data from these trials have not been extensively published in peer-reviewed form, the trial history establishes that BPC-157 has undergone regulatory-level safety assessment in human IBD patients. More recently, BPC-157 has entered clinical trials for multiple sclerosis, expanding its clinical development beyond the GI tract.[6]
Fistula Healing
One of BPC-157's most distinctive GI effects is its ability to promote healing of gastrointestinal fistulas — abnormal connections between organs or between an organ and the body surface. In rat models, BPC-157 has promoted closure of gastrocutaneous, esophagocutaneous, duodenocutaneous, colocutaneous, vesicovaginal, and rectovaginal fistulas. This fistula-healing capacity is attributed to the peptide's combined angiogenic activity, granulation tissue formation, and epithelial cell migration — coordinating the simultaneous repair of multiple tissue types at the fistula margins.[8]
The fistula healing data are particularly significant because fistulas represent one of the most challenging complications of advanced IBD and GI surgery. Current treatments often require repeated surgical intervention, and an effective pharmacological approach to fistula closure would address an important unmet clinical need.
Intestinal Anastomosis Healing
Surgical anastomoses — the reconnection of intestinal segments after resection — are critical sites of potential healing failure, leading to leakage, sepsis, and death. BPC-157 has demonstrated improved anastomotic healing in models of colon-colon anastomosis, enhancing the strength, integrity, and histological quality of the healing site. The peptide reduces the incidence of anastomotic dehiscence and abscess formation, and promotes organized collagen deposition and revascularization at the anastomotic margins.[1]
Remarkably, BPC-157 has also been studied in the context of short bowel syndrome, where it has shown effects on intestinal adaptation following massive resection. These findings suggest potential applications in post-surgical GI recovery that extend beyond simple wound healing to include functional tissue adaptation.[6]
Intestinal Barrier Function
The intestinal epithelial barrier — a single-cell-layer boundary between the gut lumen and the systemic circulation — is critical for preventing translocation of bacteria, toxins, and undigested macromolecules into the bloodstream. Barrier dysfunction (commonly described as "increased intestinal permeability" or colloquially as "leaky gut") is implicated in IBD, irritable bowel syndrome, food sensitivities, and systemic inflammatory conditions.[8]
BPC-157 stabilizes epithelial and endothelial barrier functions in gastrointestinal injury models. The peptide supports faster restoration of intestinal mucosal integrity and reduces intestinal permeability in models of chronic inflammation. This barrier-protective effect is mechanistically linked to BPC-157's action as a stabilizer of cellular junctions — the tight junctions, adherens junctions, and desmosomes that maintain the physical continuity of the epithelial barrier.[8]
Esophageal Protection
BPC-157's protective effects extend to the esophagus, where it has been studied in models of esophagitis and sphincter dysfunction. The peptide has shown effects on lower esophageal sphincter (LES) tone in experimental contexts involving neuroleptic-induced sphincter relaxation, suggesting a potential role in maintaining the anti-reflux barrier. While this research area is less developed than the gastric and colonic domains, the esophageal findings are consistent with BPC-157's pan-GI-tract cytoprotective profile.[9]
The Gut-Brain Axis
BPC-157's interactions with the nervous system are closely linked to its GI identity through the concept of the gut-brain axis — the bidirectional communication network connecting the enteric nervous system, the central nervous system, and the gastrointestinal microenvironment. As a peptide native to the GI tract with demonstrated effects on serotonergic and dopaminergic signaling, BPC-157 occupies a unique position at the interface of gastric physiology and neuropharmacology.[10]
Peripheral Administration, Central Effects
When administered peripherally (intraperitoneally or intragastrically), BPC-157 produces measurable effects on brain neurotransmitter synthesis, as demonstrated by alpha-methyl-L-tryptophan autoradiography. The peptide appears to cross the blood-brain barrier and modulate region-specific serotonin synthesis, with acute effects in the thalamus, hypothalamus, hippocampus, and substantia nigra.[10] This peripheral-to-central signaling is consistent with gut-brain axis communication mediated by peptidergic signals.
Behavioral and Neuroprotective Effects
BPC-157's gut-brain interactions manifest as beneficial effects on behavioral disturbances associated with neurotransmitter system dysfunction, including counteraction of serotonin syndrome, depression-like behaviors in the Porsolt forced swim test, and anxiety models. The peptide also attenuates encephalopathies caused by NSAID or insulin overdose — conditions that involve both systemic GI-tract damage and central nervous system injury — suggesting that BPC-157's GI protective effects and neuroprotective effects may be mechanistically interconnected through shared NO-system and vascular pathways.[10]
Gastric Stability as a Therapeutic Advantage
BPC-157's exceptional stability in gastric juice has profound implications for its GI research applications. The peptide can be administered orally with retained biological activity — a route unavailable to virtually all other bioactive peptides. This enables research designs where the peptide is delivered directly to the site of GI pathology (stomach, duodenum, intestine) through the natural route, achieving high local concentrations at the mucosal surface while simultaneously undergoing systemic absorption for distant tissue effects.[1]
The practical significance of this dual local-and-systemic effect profile is demonstrated by studies showing that intragastric BPC-157 administration heals not only gastric ulcers but also distant tendon injuries — evidence that the orally administered peptide is both locally active in the GI tract and systemically bioavailable after absorption. For detailed handling and storage protocols that preserve this stability, see our stability and storage guide.
Comparison with Standard Anti-Ulcer Agents
BPC-157's GI effects have been compared directly with established anti-ulcer agents in multiple studies. In standardized assays, the peptide has demonstrated superior effectiveness compared with cimetidine (H2 receptor antagonist), ranitidine (H2 receptor antagonist), omeprazole (proton pump inhibitor), atropine (muscarinic antagonist), and bromocriptine (dopamine agonist). Unlike these conventional agents, which primarily act by suppressing acid secretion or blocking specific receptor pathways, BPC-157 operates through a fundamentally different mechanism: direct cytoprotection of mucosal cells combined with angiogenic support for the vascular infrastructure underlying tissue repair.[4]
This mechanistic distinction is important because it positions BPC-157 as complementary to, rather than competitive with, conventional acid-suppressive therapy. The peptide addresses tissue-level repair processes that are not targeted by proton pump inhibitors or H2 blockers.
Limitations and Future Directions
Despite the extensive preclinical GI literature, important limitations persist. The concentration of research in a single laboratory group raises questions about independent reproducibility. Detailed efficacy data from the Phase II ulcerative colitis trials have not been fully reported in peer-reviewed journals, limiting external assessment of the clinical results. Dose-response relationships remain incompletely characterized, with most studies using only the standard 10 μg/kg and 10 ng/kg doses.[11]
The field would benefit from independent replication of key GI findings, formal dose-response characterization including doses above and below the standard range, long-term safety studies specifically evaluating GI tract effects during chronic administration, and randomized controlled trials in human GI conditions with adequate sample sizes and pre-registered endpoints. For guidance on experimental design considerations, see our article on how BPC-157 is studied in laboratories.
Conclusion
BPC-157's gastrointestinal research represents the strongest and most scientifically mature domain in the peptide's preclinical portfolio. From its origin in human gastric juice to its demonstrated effects across ulcer healing, IBD models, fistula closure, barrier function, and gut-brain signaling, the peptide's GI effects form a coherent narrative grounded in the cytoprotection framework. The unique combination of gastric stability, oral bioactivity, and multi-level tissue protection (cellular, endothelial, vascular) distinguishes BPC-157 from conventional gastroprotective agents and positions it as a potentially important research tool for understanding and modulating gastrointestinal repair mechanisms.