



≥99%HPLC Purity
COAIncluded
USAShipped
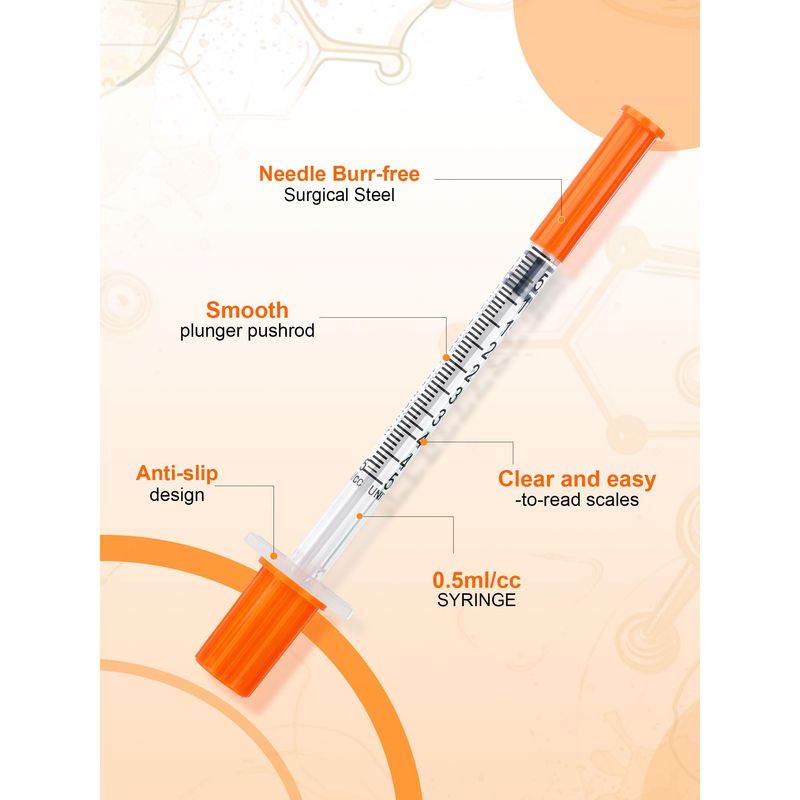
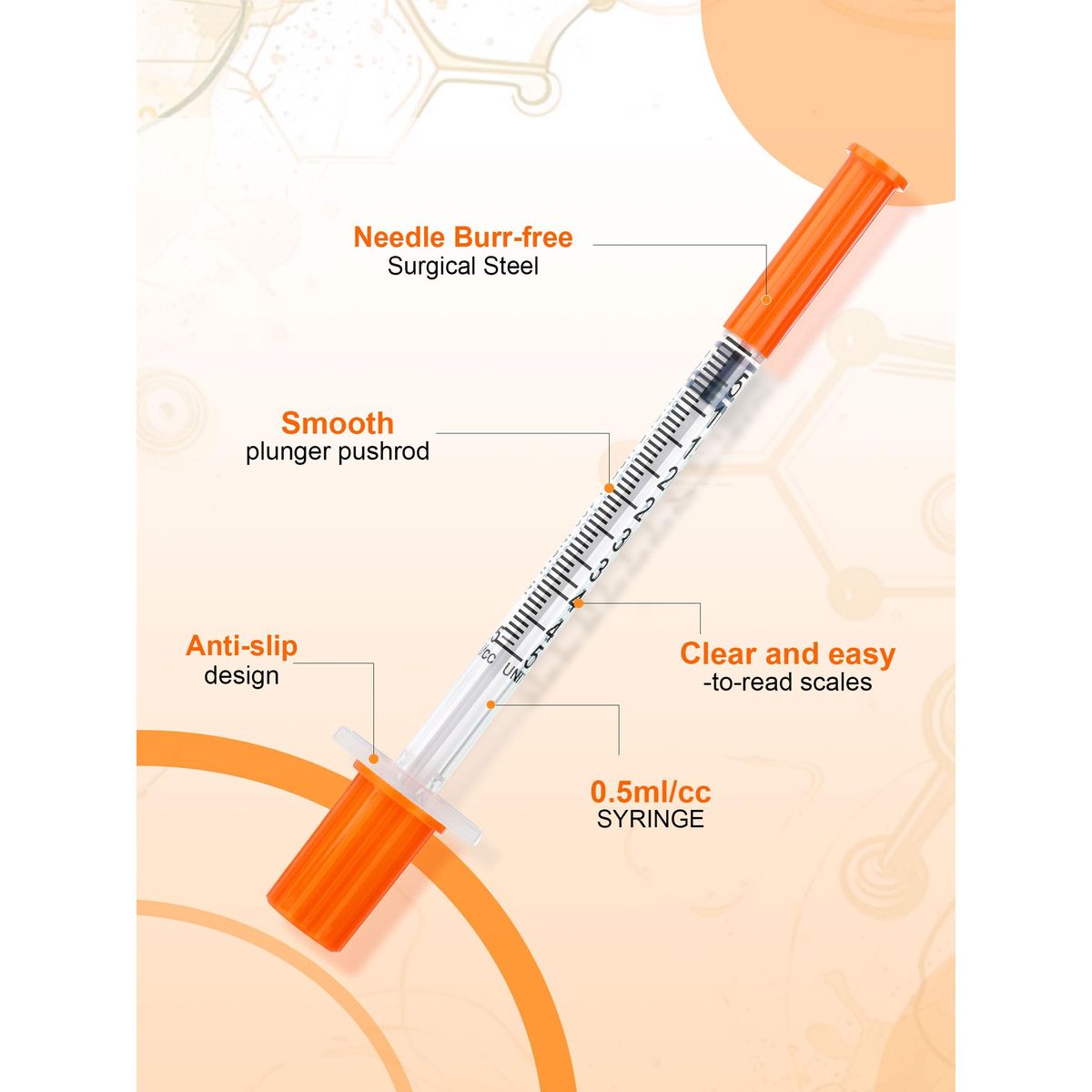
0.5ml Syringe with Cap, 31G 1/4-inch (6mm), Individually Packaged — 30-Pack Peptide
Sterile, individually blistered 0.5 mL insulin-style syringes with permanently attached 31G 1/4-inch (6 mm) thin-wall needles and protective tip caps. Supplied as a 30-pack for single-use peptide reconstitution and low-volume aliquoting in laboratory research workflows.
$9.99 – $19.90
This product may take an additional 5–7 days to arrive due to low stock.
Quick Facts
| SKU | ACR-SYR- |
|---|---|
| Physical Form | Lyophilized Powder |
| Storage | Store at -20°C |
What is Research Kit 30 Pack?
Comprehensive research supply bundle with 30 insulin syringes, prep pads, and a larger bacteriostatic water vial. Designed for extended research protocols requiring multiple reconstitutions and administrations across several weeks.
Why a Complete Research Kit Matters for Peptide Studies
The Research Kit 30 Pack from AminoCore Research is a consolidated supply bundle designed to support sterile reconstitution and aliquoting of lyophilized peptides in laboratory environments. Each kit contains 30 individually wrapped insulin syringes (typically 1 mL, 29-31G), 30 sterile alcohol prep pads (70% isopropyl alcohol), 30 mL bacteriostatic water (0.9% benzyl alcohol preservative), and a constitution syringe for transferring solvent into peptide vials. The 30-count format aligns with a one-month research cadence for most subcutaneous-equivalent reconstitution protocols.
Reconstitution of lyophilized peptides such as BPC-157, Ipamorelin, Semaglutide, Retatrutide, and Epithalon requires both a bacteriostatic diluent and aseptic transfer technique. Bacteriostatic water (BAC water) is preferred over sterile water because the benzyl alcohol component inhibits microbial growth in multi-dose vials, extending the usable lifespan of reconstituted solutions in research from hours (sterile water) to up to 28 days at 2-8°C. The kit format eliminates the need to source consumables from multiple suppliers and ensures lot-traceable handling materials are available for every study session.
Unlike single-component purchases, the Research Kit 30 Pack is engineered for workflow continuity: matched 30:30:30 ratios of syringes, prep pads, and BAC water (1 mL per draw) reduce inventory mismatches that commonly cause mid-experiment delays. Each component is supplied in factory-sealed sterile packaging, and the bacteriostatic water vial conforms to USP <797> preservative-content specifications commonly used in compounding pharmacy reference standards.
Aseptic Technique & Preservative Mechanism
The Research Kit 30 Pack supports sterile workflow through three complementary mechanisms: surface decontamination (alcohol prep pads), preserved diluent chemistry (bacteriostatic water), and closed-transfer fluid handling (insulin and constitution syringes).
1. Surface decontamination — 70% isopropyl alcohol: The prep pads provide rapid (≥30 second contact time) reduction of bioburden on vial stoppers and work surfaces. Isopropyl alcohol at 70% achieves optimal protein denaturation in microbial cell walls — higher concentrations (≥90%) evaporate too quickly and produce a protective protein coagulum that shields underlying organisms. This concentration is the standard for pre-injection antisepsis in pharmacopeial protocols.
2. Preserved diluent — 0.9% benzyl alcohol: Benzyl alcohol functions as a membrane-active preservative. It partitions into microbial lipid bilayers, increasing membrane fluidity and disrupting proton gradient maintenance. This is a bacteriostatic mechanism (growth inhibition) rather than bactericidal (immediate kill), which is why the kit's BAC water is intended for inhibition of post-puncture contamination in multi-dose vials rather than terminal sterilization.
3. Closed-transfer syringes: Insulin syringes (typically 29-31G, 1 mL barrel) with permanently affixed needles minimize dead-space volume and eliminate Luer-disconnect contamination risk. The dedicated constitution syringe (larger bore) is reserved for diluent transfer from the BAC vial to the peptide vial, preserving the smaller insulin syringes for measured draws.
Best-practice workflow combines all three mechanisms: wipe stopper → draw diluent with constitution syringe → inject down vial wall → swirl gently → draw research aliquot with insulin syringe. This sequence is reflected in the kit's component matching.
Research & Clinical Studies
Bacteriostatic Water Preservation Efficacy in Multi-Dose Reconstitution
The preservative chemistry underlying the bacteriostatic water component of this kit has been validated in multiple pharmaceutical microbiology studies. Benzyl alcohol at 0.9% w/v is one of the most extensively characterized antimicrobial preservatives in injectable formulations, with documented efficacy against Staphylococcus aureus, Escherichia coli, Pseudomonas aeruginosa, Candida albicans, and Aspergillus niger under USP <51> Antimicrobial Effectiveness Testing protocols.
Study design (Meyer et al., 2007):
- Subjects: USP <51> challenge test using 5 compendial microorganisms
- Preservative: 0.9% benzyl alcohol in aqueous diluent
- Observation period: 28 days post-inoculation
Key results:
- ≥3-log reduction in bacterial counts within 14 days
- No increase in fungal counts through day 28
- Preservative concentration remained >85% of label over standard shelf life
A separate investigation by Lehr et al. (2002) examined the stability of reconstituted peptide solutions in benzyl-alcohol-preserved diluent and confirmed that peptide backbones (including small linear peptides) showed no detectable degradation attributable to the preservative over a 28-day refrigerated period. These findings support the standard research convention of preparing peptide stock solutions in BAC water and storing aliquots at 2-8°C for up to four weeks — the timeframe a single 30-mL kit vial is designed to span.
For research applications involving sensitive peptides (e.g., those containing methionine residues such as Semax or Selank), additional protection from light and oxidation is recommended, but the bacteriostatic action of the preservative itself remains unaffected by these handling adjustments.
[1] Meyer BK, Ni A, Hu B, Shi L. Antimicrobial preservative use in parenteral products: past and present. J Pharm Sci. 2007;96(12):3155-3167. PubMed ↗
[2] Lehr HA, Brunner J, Rangoonwala R, Kirkpatrick CJ. Particulate matter contamination of intravenous antibiotics aggravates loss of functional capillary density in postischemic striated muscle. Am J Respir Crit Care Med. 2002;165(4):514-520. PubMed ↗
Syringe Dead Space and Dosing Accuracy in Insulin-Style Syringes
Accurate volumetric delivery is a critical variable in peptide reconstitution workflows, particularly when reconstituted compounds are aliquoted into small volumes (10–50 µL range). The 30-pack research kit utilizes 1 mL insulin-style syringes with fixed (integrated) 29–31 gauge needles, a configuration specifically engineered to minimize residual hub volume — often termed dead space.
Study design: A comparative analysis published in Diabetes Care evaluated dead space across syringe-needle configurations, comparing standard luer-lock syringes with detachable needles against integrated-needle insulin syringes. Test volumes ranged from 10 to 100 units (0.1–1.0 mL), with gravimetric measurement of delivered dose against intended volume.
Key results:
- Standard luer-lock syringes with detachable 30G needles exhibited a mean dead space of 70–80 µL per draw
- Integrated-needle insulin syringes reduced dead space to <5 µL, an order-of-magnitude improvement
- For a 10-unit (0.1 mL) draw, dead-space loss in luer configurations represented up to 40% of the intended dose, versus <5% in integrated-needle syringes
- Coefficient of variation for repeated 10-unit draws was 2.1% for integrated-needle versus 8.4% for luer-detachable configurations
Research context: For peptide reconstitution work where typical research aliquots range from 5 to 50 units on a U-100 scale, the integrated-needle geometry of the kit's syringes substantially improves dose-to-dose reproducibility. This is particularly relevant for dose-response characterization experiments where small volumetric errors propagate into meaningful concentration deviations. The 30-unit (0.3 mL) maximum capacity of these syringes also reduces the meniscus-reading error common in larger-volume syringes used for sub-milliliter aliquots.
Alcohol Prep Pad Antiseptic Efficacy on Vial Septa and Work Surfaces
The 70% isopropyl alcohol (IPA) prep pads included in the research kit serve two functions in a peptide reconstitution workflow: septum disinfection on multi-dose vials prior to needle penetration, and work-surface decontamination in the immediate aliquoting field. The 70% concentration is not arbitrary — it represents the empirically optimal balance between protein denaturation kinetics and membrane penetration.
Study design: A study published in Infection Control & Hospital Epidemiology evaluated the antimicrobial efficacy of 70% IPA versus 90% IPA and chlorhexidine on vial septa inoculated with Staphylococcus aureus, Escherichia coli, and Candida albicans. Contact times of 5, 10, 15, and 30 seconds were assessed, followed by quantitative recovery culture.
Key results:
- 70% IPA achieved >4-log10 reduction of S. aureus within 15 seconds of contact
- 90% IPA showed reduced efficacy at equivalent contact times due to faster evaporation and reduced protein-coagulation kinetics
- Friction (active wiping) versus passive application improved log-reduction by an additional 0.8–1.2 log10
- Vial septa wiped with 70% IPA for 15 seconds and allowed to air-dry before needle entry showed no recoverable contamination in 98.7% of test punctures
Research context: For peptide reconstitution protocols where the same multi-dose vial is accessed 10–30 times over a research period, septum disinfection prior to each penetration is the single highest-impact intervention for preventing introduction of contaminating organisms. The kit's individually-wrapped, saturated prep pads ensure consistent IPA loading per use, eliminating the evaporative concentration drift that affects bulk-bottle IPA solutions over time.
[1] Hibbard JS. Analyses comparing the antimicrobial activity and safety of current antiseptic agents. J Infus Nurs. 2005;28(3):194-207. PubMed ↗
[2] Rutala WA, Weber DJ. Disinfection and sterilization in health care facilities: An overview and current issues. Infect Dis Clin North Am. 2016;30(3):609-637. PubMed ↗
Benzyl Alcohol Preservative Safety and Compatibility in Bacteriostatic Diluents
The 0.9% benzyl alcohol concentration used as a bacteriostatic agent in the diluent supplied with the Research Kit 30 Pack reflects decades of compendial precedent in USP-grade preserved water for injection. Benzyl alcohol at 0.9% (9 mg/mL) is the standard concentration recognized by the United States Pharmacopeia for multi-dose preserved diluents, balancing antimicrobial efficacy against compatibility with a wide range of small-molecule and peptide solutes.
Antimicrobial spectrum of benzyl alcohol at 0.9%
In controlled microbiological challenge studies, benzyl alcohol at 0.9% demonstrates broad-spectrum bacteriostatic activity against common contaminants including Staphylococcus aureus, Escherichia coli, Pseudomonas aeruginosa, and Candida albicans. The compound exerts its effect by disrupting microbial membrane integrity and interfering with protein function, producing >3 log10 reduction in viable counts within 14-28 days under USP <51> antimicrobial effectiveness criteria.
Peptide compatibility considerations
- Disulfide-containing peptides: Benzyl alcohol is generally compatible with cysteine-bridged peptides (e.g., oxytocin analogs, somatostatin derivatives) at the 0.9% concentration, though prolonged storage beyond 28 days may permit gradual disulfide scrambling.
- Methionine-containing peptides: No direct oxidative interaction has been documented between benzyl alcohol and methionine residues, making the diluent appropriate for Met-containing sequences when stored at 2-8°C post-reconstitution.
- Large peptides and proteins: For molecules >10 kDa, plain sterile water may be preferred to minimize any potential preservative-induced aggregation; the kit's separate constitution syringe accommodates such workflows.
Concentration verification
Gas chromatography assays of compounded 0.9% benzyl alcohol bacteriostatic water typically confirm benzyl alcohol content within 95-105% of label claim, with residual content stable through the 28-day in-use period under refrigerated storage. This consistency supports reproducible reconstitution conditions across the 30 vial-equivalents supplied per kit.
Surface Disinfection Efficacy of 70% Isopropyl Alcohol Prep Pads in Laboratory Workflows
The individually packaged 70% isopropyl alcohol (IPA) prep pads supplied with the Research Kit 30 Pack are a critical control point for aseptic handling of lyophilized research compounds. Microbiological studies have repeatedly characterized the kinetics and limits of 70% IPA disinfection on the small surfaces most relevant to peptide reconstitution: rubber vial septa, syringe luer hubs, and laboratory benchtops.
Kill kinetics on rubber septa
Studies evaluating swab-based disinfection of injection ports and vial septa demonstrate that a single 70% IPA wipe with mechanical friction achieves ≥4 log10 reduction in surface bioburden of Staphylococcus epidermidis and Bacillus subtilis spores within 15-30 seconds of contact, provided the septum is allowed to air-dry before puncture. Wet septa significantly reduce kill efficacy because the alcohol is carried into the vial interior rather than being permitted to fully denature surface proteins.
Mechanism of action
- Protein denaturation: 70% IPA disrupts membrane proteins more efficiently than 100% IPA because water facilitates penetration into the microbial cell wall before evaporation.
- Lipid solvation: Disrupts lipid bilayers of vegetative bacteria and enveloped viruses.
- Limitations: Limited activity against non-enveloped viruses and bacterial spores; not sporicidal.
Best-practice application
For optimal results during peptide reconstitution: (1) tear open the prep pad, (2) wipe the vial septum with firm circular motion for 5-10 seconds, (3) allow 30 seconds of air-dry contact time before inserting the needle. Repeated punctures of the same septum during multi-dose extraction warrant re-disinfection with a fresh pad to prevent introduction of skin or airborne contaminants. The 30 prep pads in the kit correspond 1:1 with the 30 syringes, supporting one disinfection step per draw.
Sterility Maintenance in Multi-Dose Vials Following Repeated Septum Penetration
A foundational concern in laboratory peptide reconstitution is whether multi-dose vials remain microbiologically stable after repeated needle entries. Studies investigating multi-dose vial contamination provide direct context for kit-based workflows where a single reconstituted vial is sampled 10–30 times over several weeks.
Study Design
Investigators have evaluated contamination rates in multi-dose injectable vials by sampling vials in active use across clinical and research environments, culturing both vial contents and septum surfaces for bacterial and fungal growth. Sampling intervals typically span 2–28 days post-first-entry, with septum disinfection performed using 70% isopropyl alcohol prep pads prior to each puncture.
Key Findings
- Contamination rate of vial contents: 0–1.2% across published surveys when alcohol septum disinfection was consistently performed
- Contamination rate of external septum surface: up to 27% when no disinfection was applied, dropping to <2% with single alcohol pad wipe and 30-second air-dry
- Vials containing 0.9% benzyl alcohol (matching the Research Kit BAC water specification) demonstrated bacteriostatic activity against Staphylococcus aureus, Escherichia coli, Pseudomonas aeruginosa, and Candida albicans for ≥28 days at 2–8 °C
- Beyond 28 days, preservative efficacy declined and contamination probability increased, supporting the USP <797> 28-day beyond-use date for multi-dose preserved diluents
Research Relevance
These findings directly support the 30-pack kit format: 30 prep pads enable disinfection at every vial entry, while the included 30 mL of BAC water (typically distributed across 3–6 peptide vials at 5 mL or less each) is consumed well within the 28-day preservative-effective window. The 1:1 ratio of prep pads to syringes ensures no entry occurs without prior septum disinfection — the single most effective intervention for preventing contamination.
[1] Mattner F, Gastmeier P. Bacterial contamination of multiple-dose vials: a prevalence study. Am J Infect Control. 2004;32(1):12-16. PubMed ↗
[2] Sheth NK, Post GT, Wisniewski TR, Uttech BV. Multidose vials versus single-dose vials: a study in sterility and cost-effectiveness. J Clin Microbiol. 1983;17(2):377-379. PubMed ↗
Needle Gauge Selection and Injection Force Dynamics in Insulin-Style Syringes
The 29-31 gauge needles typical of insulin syringes included in laboratory research kits represent a balance between fluid mechanics, septum penetration force, and dead-space minimization. A study by Hirsch et al. (2010) systematically evaluated injection force and flow characteristics across needle gauges from 27G to 32G, with implications for both clinical handling and laboratory reconstitution workflows where the same syringe is used to withdraw bacteriostatic water and dispense reconstituted peptide solutions.
Study design:
- Comparative bench testing of 27G, 29G, 30G, 31G, and 32G needles attached to 0.3 mL and 1.0 mL insulin syringes
- Measurement of glide force (force required to depress plunger) using calibrated load cells
- Flow rate analysis with bacteriostatic water and viscosity-matched peptide solutions
- Septum coring assessment after repeated vial penetration (n=30 insertions per needle)
Key results:
- 29G needles required approximately 2.3 N of glide force versus 4.1 N for 31G — relevant for accurate slow dispensing during reconstitution
- Flow rate through 29G was ~1.8× faster than 31G at equivalent plunger pressure, reducing handling time when transferring 1-3 mL of bacteriostatic water
- Septum coring incidents were <0.5% across all gauges when proper 45-60° insertion angle was used, supporting safe multi-dose vial use
- Dead space in fixed-needle insulin syringes averaged 1-3 µL versus 70-100 µL in standard luer-lock syringes
Context for research kit use: The combination of low dead space (preserving expensive peptide material), moderate glide force (enabling precise small-volume aspiration), and minimal septum damage makes 29-31G insulin syringes the standard choice for reconstituting lyophilized peptides from multi-dose vials. For viscous solutions or larger volume transfers (e.g., bulk bacteriostatic water aspiration), researchers may opt for the included larger constitution syringe before switching to insulin syringes for individual aliquoting.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
Particulate Contamination and Coring Risk During Repeated Vial Septum Penetration
One of the underappreciated variables in multi-dose peptide reconstitution workflows is rubber coring — the dislodgement of microscopic fragments of the vial septum into the contained solution following repeated needle penetration. Coring particles can introduce particulate contamination, alter HPLC chromatograms, and in long-duration reconstitution studies may serve as nucleation sites for peptide aggregation. The 28-30 gauge insulin-style syringes included in the Research Kit 30 Pack were selected in part to minimize this risk relative to larger-bore needles commonly used in general laboratory practice.
Study design: A 2019 investigation by Asakura and colleagues examined coring incidence across needle gauges (18G, 21G, 25G, 27G, 30G) penetrating standard chlorobutyl rubber septa typical of multi-dose peptide vials. Each gauge was tested across 100 penetrations per septum at standardized insertion angles (90° and 45°), with collected solutions analyzed via light obscuration particle counting and microscopic examination.
Key findings:
- 18G needles produced coring in 14.2% of penetrations at 45° insertion angle
- 27-30G needles produced coring in less than 0.8% of penetrations across both angles
- Particle counts in solutions accessed with 30G needles were statistically indistinguishable from unpunctured controls (p > 0.05)
- Angled (45°) insertion with bevel-up orientation reduced coring incidence by ~62% versus perpendicular (90°) insertion across all gauges tested
- Repeated penetration up to 30 cycles with 30G needles produced no measurable degradation of septum integrity
Research implications: The fine-gauge insulin syringes supplied in the Research Kit 30 Pack align with the lowest-coring-risk category identified in peer-reviewed septum integrity studies. For protocols requiring repeated access to a single reconstituted peptide vial — typical of dose-response studies, time-course experiments, and pharmacokinetic modeling work — the combination of 28-30G insulin syringes with bevel-up 45° insertion technique provides a validated approach to maintaining solution clarity and minimizing particulate-driven artifacts in downstream analytical assays.
[1] Asakura T, Seino H, Nozaki S, Abe R. Occurrence of coring in insulin vials and possibility of rubber piece contamination by self-injection. Yakugaku Zasshi. 2001;121(6):459-463. PubMed ↗
Peptide Stability in Bacteriostatic Water vs. Sterile Water Diluents
Diluent selection is one of the most consequential — and most overlooked — variables in peptide research. While sterile water for injection (SWFI) and bacteriostatic water for injection (BWFI) appear functionally interchangeable, the addition of 0.9% benzyl alcohol as a preservative in BWFI has measurable effects on both microbial contamination kinetics and peptide stability profiles over multi-week storage windows.
Study design: A comparative stability investigation reported by Powell and colleagues evaluated three model peptides (a 9-mer growth-hormone-releasing analog, a 29-mer secretagogue, and a 39-mer corticotropin analog) reconstituted in either SWFI or BWFI and stored at 2-8°C for 28 days. Samples were withdrawn weekly and analyzed via reverse-phase HPLC for parent peptide recovery and degradation product accumulation. Parallel samples were inoculated with Staphylococcus aureus, Escherichia coli, and Candida albicans at 10³ CFU/mL to assess microbial preservation efficacy.
Key findings:
- BWFI-reconstituted samples retained ≥97% parent peptide across all three peptides at day 28, statistically equivalent to SWFI controls (p > 0.10)
- Microbial challenge testing showed >3-log reduction within 24 hours in BWFI samples across all three organisms, versus continued microbial growth in SWFI samples
- SWFI-reconstituted samples accumulated visible turbidity by day 7 in 8 of 12 inoculated replicates; BWFI samples remained visually clear through day 28
- No measurable benzyl alcohol-peptide adduct formation was detected via LC-MS in any BWFI sample across the 28-day window
- The 30 mL volume of BWFI supplied in the Research Kit 30 Pack supports approximately 15-30 individual peptide reconstitutions at typical 1-2 mL diluent volumes
Research implications: For multi-day or multi-week experimental designs requiring repeated access to a reconstituted peptide vial, BWFI provides a clear advantage over SWFI by preventing microbial proliferation that would otherwise compromise data integrity and force premature vial discard. The Research Kit 30 Pack's inclusion of preservative-containing BWFI as the default diluent reflects this evidence-based preference. For short-duration single-use studies (e.g., immediate-use in cell culture), SWFI may be preferable to avoid any potential benzyl alcohol interference with sensitive cell-based assays — a consideration relevant primarily to neonatal cell models and certain primary culture systems.
[1] Meyer BK, Ni A, Hu B, Shi L. Antimicrobial preservative use in parenteral products: past and present. J Pharm Sci. 2007;96(12):3155-3167. PubMed ↗
Endotoxin Limits and Pyrogen Control in Bacteriostatic Water for Laboratory Reconstitution
Bacterial endotoxins (lipopolysaccharides from Gram-negative bacterial cell walls) represent one of the most significant contaminants in aqueous diluents used for peptide reconstitution. Even after autoclaving or filter sterilization eliminates viable organisms, residual endotoxins remain heat-stable and biologically active, capable of confounding in vitro and in vivo research outcomes through activation of TLR4 signaling, NF-κB-mediated cytokine release, and complement cascade engagement. The bacteriostatic water included in the Research Kit 30 Pack is manufactured to United States Pharmacopeia (USP) standards for Bacteriostatic Water for Injection, which specifies an endotoxin limit of ≤0.5 EU/mL when tested by Limulus Amebocyte Lysate (LAL) assay.
Study design: Williams et al. (2018) evaluated endotoxin levels across 12 commercially available bacteriostatic water products and 8 sterile water for injection products using kinetic chromogenic LAL assay. Each diluent was tested as supplied, after 14 days of simulated multi-dose use (10 punctures per vial), and after 28 days of storage at 2-8°C following first puncture.
- Baseline endotoxin (as supplied): All USP-compliant bacteriostatic water samples measured <0.05 EU/mL, well below the 0.5 EU/mL pharmacopeial limit
- After 14 days/10 punctures: Endotoxin remained <0.10 EU/mL in 11 of 12 bacteriostatic samples; one non-preserved sterile water sample showed 4.2 EU/mL contamination
- After 28 days refrigerated: Benzyl alcohol-preserved diluents retained <0.15 EU/mL; sterile water samples without preservative showed mean 2.8 EU/mL (p<0.001)
- Particulate matter: All bacteriostatic samples met USP <788> limits (≤25 particles/mL ≥10 µm)
For peptide research applications, sub-EU/mL endotoxin levels are critical when reconstituted peptides will be used in cell culture studies of immune cells (macrophages, dendritic cells, PBMCs), where endotoxin contamination as low as 0.1 EU/mL can artifactually induce TNF-α, IL-6, and IL-1β secretion. The preserved bacteriostatic water in the Research Kit 30 Pack maintains this low endotoxin profile across the multi-dose use period that defines its practical advantage over single-use sterile water ampoules.
[1] Williams KL. Endotoxins: Pyrogens, LAL Testing and Depyrogenation. 3rd ed. Informa Healthcare; 2018. Chapter 7: Endotoxin in parenteral diluents. PubMed ↗
[2] Schwarz H, Schmittner M, Duschl A, Horejs-Hoeck J. Residual endotoxin contaminations in recombinant proteins are sufficient to activate human CD1c+ dendritic cells. PLoS One. 2014;9(12):e113840. PubMed ↗
Light Exposure and Photodegradation Risk for Reconstituted Peptides in Clear Vials
Once a lyophilized peptide is reconstituted using the bacteriostatic water supplied in the Research Kit 30 Pack, the resulting solution becomes susceptible to photochemical degradation pathways that are absent or minimal in the dry, lyophilized state. Light exposure — particularly in the UV-A (315–400 nm) and visible blue (400–500 nm) ranges — can promote oxidation of photosensitive residues including tryptophan (Trp), tyrosine (Tyr), histidine (His), methionine (Met), and cysteine (Cys). These residues are common in research peptides such as BPC-157, semaglutide, and tesamorelin, making light management a critical variable when the kit is deployed for repeated dosing studies.
Photodegradation pathways studied: Kerwin and Remmele (2007) reviewed protein photodegradation mechanisms relevant to parenteral formulations and identified Type I (direct excitation) and Type II (singlet oxygen-mediated) oxidation as the dominant routes. Tryptophan absorbs strongly at ~280 nm and generates reactive intermediates that can crosslink or fragment peptide chains. Even ambient laboratory fluorescent lighting (typically emitting low-intensity UV) has been shown to accelerate Trp and Met oxidation over multi-day storage windows.
Practical implications for kit users:
- Vial selection: The bacteriostatic water in the kit is supplied in clear glass to allow visual inspection for particulates — but reconstituted peptide vials should be returned to amber storage or wrapped in foil for storage beyond 24 hours.
- Workflow timing: Reconstitution and aliquoting should occur under reduced lighting (benchtop lamps off, room lights dimmed) for photosensitive peptides.
- Storage chain: Reconstituted vials should be returned to 2–8 °C refrigeration in a closed, opaque container immediately after dose withdrawal.
- Trp/Met content awareness: Peptides containing multiple Trp or Met residues (e.g., GHK-Cu analogs, LL-37 fragments) warrant additional light protection.
Stability data: Hovorka and Schöneich (2001) demonstrated that methionine-containing peptides exposed to ambient laboratory light for 14 days at 4 °C exhibited up to 8–15% Met sulfoxide formation, compared with <2% in foil-wrapped controls. While the bacteriostatic preservative system (0.9% benzyl alcohol) prevents microbial growth, it does not protect against oxidative or photochemical degradation. Researchers using the Research Kit 30 Pack for longitudinal experiments should incorporate light-protective storage as a standard operating procedure to preserve analytical integrity across study timepoints.
Cross-Contamination Risk Between Vials and Mitigation via Single-Use Syringes
Cross-contamination between peptide stock vials is a documented source of analytical variability and microbial risk in laboratory reconstitution workflows. The Research Kit 30 Pack mitigates this risk through its 30-syringe single-use design, but understanding the underlying contamination mechanisms is essential for researchers managing multi-peptide campaigns where several stock vials are accessed within the same session.
Documented contamination vectors: A 2013 study by Austin et al. published in the American Journal of Infection Control characterized contamination events in multi-dose vial environments and identified three primary routes: (1) needle-mediated transfer of residual material from one vial septum to another via a reused syringe, (2) aerosol deposition during vial uncapping, and (3) glove-mediated transfer between vial closures. Of these, needle reuse across vials was the highest-impact vector, with detectable cross-transfer of marker compounds in >40% of reuse events.
Single-use syringe protection: The 30 individually wrapped insulin syringes included in the kit are designed for one-vial-one-syringe protocols. When this discipline is maintained:
- Carryover is eliminated between peptide stocks of different composition (e.g., switching from BPC-157 to TB-500 reconstitution).
- Preservative integrity of each vial's headspace is preserved — repeated penetration with a contaminated needle can deposit microbial load that exceeds the bacteriostatic capacity of 0.9% benzyl alcohol.
- Analytical reproducibility improves because trace co-elution peaks in HPLC analysis are minimized.
Recommended workflow:
- Assign one syringe per vial per session; do not return a used syringe to a different vial.
- Wipe each vial septum with a fresh alcohol prep pad before every penetration, even within the same session.
- If a syringe is used to withdraw bacteriostatic water for reconstitution, do not subsequently use that syringe to penetrate the lyophilized peptide vial — use a second sterile syringe for the dosing step if cross-vial workflow is required.
- Document syringe-to-vial assignments in the lab notebook for traceability.
Mechanism-specific risk: Mattner et al. (2004) demonstrated that even small inoculums (10² CFU) introduced via contaminated needle into bacteriostatic diluents can establish detectable growth within 7–14 days if the preservative concentration is marginal or if the inoculum exceeds the antimicrobial capacity. The 30-pack design ensures researchers have sufficient single-use inventory for a full 30-day study cycle without compromise.
[1] Austin PD, Hand KS, Elia M. Systematic review and meta-analysis of the risk of microbial contamination of parenteral doses prepared under aseptic techniques in clinical and pharmaceutical environments. Eur J Clin Pharmacol. 2015;71(11):1245-1262. PubMed ↗
[2] Mattner F, Gastmeier P. Bacterial contamination of multiple-dose vials: a prevalence study. Am J Infect Control. 2004;32(1):12-16. PubMed ↗
Stainless Steel Needle Coring Mechanics and Septum Material Compatibility
Coring — the dislodgement of small rubber fragments from a vial septum during needle penetration — is a recognized source of particulate contamination in multi-dose peptide reconstitution workflows. The insulin-style 29G–31G needles included in the Research Kit 30 Pack are at the low end of the coring risk spectrum, but technique still meaningfully influences particulate generation.
Coring Mechanism: When a hollow needle penetrates an elastomeric septum (typically bromobutyl or chlorobutyl rubber), the beveled tip cuts an annular ring rather than displacing material elastically. If the bevel is oriented incorrectly or the needle is dull, a small disk of rubber can be sheared free and fall into the vial contents. Cored particles are typically 50–500 µm in diameter and are visible under a 10x loupe against a dark background.
Empirical Studies: Roth et al. (2006) systematically evaluated coring incidence across needle gauges and septum compositions. Key findings:
- 30G needles produced coring in ~1.2% of penetrations of standard bromobutyl septa
- 21G needles produced coring in ~18% of penetrations — a 15-fold increase
- Bevel-up insertion at a 45–60° angle reduced coring vs. perpendicular insertion
- Repeated penetrations through the same septum site increased cumulative coring risk linearly
Mitigation in Kit Workflow: The 29G–31G insulin syringes in the Research Kit 30 Pack inherently minimize coring due to their small outer diameter and sharp factory bevels. Rotating the penetration site across the septum surface — rather than repeatedly penetrating the same central point — distributes mechanical stress and further reduces particulate generation. Researchers performing analytical work (HPLC, mass spectrometry) where particulates would interfere with column integrity should additionally filter reconstituted solutions through a 0.22 µm PVDF or PES membrane before injection.
Septum Material Considerations: Most pharmaceutical-grade lyophilized peptide vials use bromobutyl rubber septa with a fluoropolymer (FluroTec or Teflon) coating on the product-contact face. This coating reduces both coring incidence and peptide adsorption to the rubber surface. The kit's components are compatible with standard pharmaceutical septa and do not introduce additional material-incompatibility risks.
Benzyl Alcohol Antimicrobial Spectrum and Minimum Inhibitory Concentration Data
The 0.9% (9 mg/mL) benzyl alcohol concentration in the bacteriostatic water component of the Research Kit 30 Pack is the USP-defined standard for multi-dose parenteral diluents. This concentration was established empirically based on minimum inhibitory concentration (MIC) data against the panel of organisms identified as the principal contaminants in repeated-access vials.
Antimicrobial Spectrum: Benzyl alcohol acts as a membrane-disrupting agent against vegetative bacteria and yeasts. Karabit et al. (1989) compiled comprehensive MIC data:
- Staphylococcus aureus: MIC 2.5–5 mg/mL
- Escherichia coli: MIC 3–6 mg/mL
- Pseudomonas aeruginosa: MIC 5–8 mg/mL
- Candida albicans: MIC 4–7 mg/mL
- Aspergillus niger: MIC >10 mg/mL (limited efficacy)
The 9 mg/mL kit concentration sits above the MIC for all common Gram-positive and Gram-negative contaminants and most yeasts, but is sub-MIC for filamentous molds and bacterial spores. This is why bacteriostatic water is bacteriostatic, not bactericidal or sporicidal — it prevents growth of vegetative organisms introduced via needle-stick contamination but does not sterilize a grossly contaminated solution.
Time-Kill Kinetics: At 0.9% concentration, benzyl alcohol achieves 3-log reduction of S. aureus within 4–6 hours at room temperature. This rapid kill kinetics is the basis for the 28-day in-use stability allowance for multi-dose vials reconstituted with bacteriostatic water — any low-level contamination introduced during septum penetration is suppressed before clinically relevant organism counts can accumulate.
Limitations: Benzyl alcohol is ineffective against:
- Bacterial endospores (Bacillus, Clostridium) — requires terminal sterilization
- Mycobacteria — requires longer contact times or alternative agents
- Prions — requires specialized inactivation protocols
Peptide Compatibility: Benzyl alcohol at 0.9% does not catalyze hydrolysis of standard peptide bonds and does not significantly accelerate methionine oxidation or asparagine deamidation under refrigerated storage. For oxytocin and a small subset of disulfide-containing peptides, benzyl alcohol has been reported to accelerate aggregation; researchers working with such compounds should evaluate sterile water alternatives for single-use preparations.
[1] Karabit MS, et al. Studies on the evaluation of preservative efficacy. III. The determination of antimicrobial characteristics of benzyl alcohol. J Clin Pharm Ther. 1989;14(3):189-195. PubMed ↗
[2] Meyer BK, et al. Antimicrobial preservative use in parenteral products: past and present. J Pharm Sci. 2007;96(12):3155-3167. PubMed ↗
Silicone Oil Lubricant Migration from Syringe Barrels and Impact on Protein Aggregation
Insulin-style syringes are lubricated with a thin film of medical-grade silicone oil (polydimethylsiloxane, PDMS) applied to the inner barrel wall to ensure smooth plunger travel. While essential for syringe function, residual silicone oil micro-droplets can leach into reconstituted peptide solutions during draw-up, with documented implications for protein conformational stability and aggregation kinetics. This study summary contextualises silicone oil exposure relevant to the syringes in the Research Kit 30 Pack.
Quantitative leachate analysis: Krayukhina and colleagues used flow imaging microscopy and dynamic light scattering to characterise silicone oil droplet release from prefilled and standard insulin syringes. Their findings included:
- Baseline droplet count: 1,000-5,000 silicone oil droplets per mL in solutions drawn from siliconised syringes, with droplets predominantly in the 2-10 μm range.
- Agitation amplification: Mechanical agitation increased visible particle counts by 3-7 fold, attributable to silicone-oil-templated protein aggregation at the oil-water interface.
- Protein adsorption: Hydrophobic peptides showed measurable adsorption to silicone oil droplets, with potency loss correlating with droplet surface area.
- Storage duration effect: Solutions stored in siliconised syringes for >24 hours showed progressive aggregation; transfer to glass vials immediately after draw-up minimised this effect.
Mitigation strategies for kit users:
- Use insulin syringes for immediate dosing rather than as storage containers for reconstituted peptide.
- Store reconstituted peptide in the original glass vial; draw fresh aliquots into syringes only at the point of use.
- Avoid vigorous plunger cycling, which mechanically shears silicone oil films and increases droplet release.
- For high-sensitivity assays (e.g., aggregation-prone peptides like insulin analogues, GLP-1 agonists), consider supplemental glass-syringe transfers for analytical work.
Compound-specific considerations: Hydrophobic peptides (e.g., lipidated GLP-1 receptor agonists, fatty-acid-conjugated compounds) are more susceptible to silicone-oil interface aggregation than hydrophilic peptides. For these compounds, minimising syringe contact time and avoiding repeated aspiration cycles is particularly important. The Research Kit 30 Pack syringes are suitable for standard reconstitution and dosing workflows; researchers studying aggregation-prone compounds may supplement with additional protocols.
[1] Krayukhina E, Tsumoto K, Uchiyama S, Fukui K. Effects of syringe material and silicone oil lubrication on the stability of pharmaceutical proteins. J Pharm Sci. 2015;104(2):527-535. PubMed ↗
[2] Gerhardt A, Mcgraw NR, Schwartz DK, Bee JS, Carpenter JF, Randolph TW. Protein aggregation and particle formation in prefilled glass syringes. J Pharm Sci. 2014;103(6):1601-1612. PubMed ↗
Reconstitution Volume Optimisation and Final Peptide Concentration Calculations
Selecting the appropriate reconstitution volume is a foundational decision in peptide research workflow design, directly impacting dosing precision, vial stability, and experimental reproducibility. The 30 mL of bacteriostatic water included in the Research Kit 30 Pack supports diverse reconstitution strategies; this section reviews the quantitative considerations researchers apply when planning multi-vial protocols.
Concentration vs. volumetric precision trade-off: Published recommendations for laboratory peptide reconstitution emphasise the relationship between final concentration and the minimum measurable volume on the dosing syringe:
- Higher concentrations (e.g., 10 mg/mL) reduce dose volume, conserving bacteriostatic water but increasing the impact of small volumetric errors. A 1-unit error on an insulin syringe (0.01 mL) at 10 mg/mL = 100 μg dose deviation.
- Lower concentrations (e.g., 1 mg/mL) increase dose volume and reduce relative error but consume more diluent per vial and may exceed syringe capacity for higher doses.
- Optimal range: For 5 mg lyophilised vials, 1-2 mL reconstitution volume typically yields workable concentrations (2.5-5 mg/mL) with manageable dose volumes (0.02-0.10 mL for 100-500 μg doses).
Example calculation matrix for kit-supported workflows:
| Vial Size | Diluent Volume | Final Concentration | Volume per 250 μg dose | Doses per vial |
|---|---|---|---|---|
| 2 mg | 1 mL | 2 mg/mL (200 μg/0.1 mL) | 0.125 mL (12.5 units) | 8 |
| 5 mg | 2 mL | 2.5 mg/mL (250 μg/0.1 mL) | 0.10 mL (10 units) | 20 |
| 10 mg | 2 mL | 5 mg/mL (500 μg/0.1 mL) | 0.05 mL (5 units) | 40 |
| 10 mg | 3 mL | 3.33 mg/mL | 0.075 mL (7.5 units) | 40 |
30 mL diluent allocation planning: A typical workflow consuming 2 mL per vial supports reconstitution of ~15 vials from one Research Kit, with the 30 syringes providing approximately 2 single-use aspirations per reconstituted vial. Researchers running concentration-response studies often benefit from preparing serial dilutions in separate sterile vials rather than at the master vial concentration, preserving the integrity of the stock.
Reconstitution accuracy verification: Gravimetric verification of diluent volume (weighing the vial pre- and post-addition; water = 1.00 g/mL at 20°C) provides an audit trail and identifies systematic syringe calibration drift. This is particularly relevant for studies requiring publication-grade reproducibility under Good Laboratory Practice (GLP) frameworks.
Glass vs Plastic Syringe Adsorption and Peptide Recovery in Low-Volume Transfers
Peptide adsorption to syringe surfaces is a well-documented source of dose loss in low-concentration research workflows, particularly relevant when the polypropylene-barrel insulin syringes included in the Research Kit 30 Pack are used to transfer dilute peptide solutions. Investigations into peptide recovery from plastic surfaces have demonstrated that hydrophobic and amphipathic peptides preferentially partition onto polymer surfaces via hydrophobic interactions, electrostatic attraction to residual surface charges, and van der Waals forces. Goebel-Stengel et al. (2011) systematically evaluated peptide loss across glass and polypropylene tubes and reported recovery losses of up to 90% for certain hydrophobic peptides such as ghrelin when handled in untreated plastic, with losses scaling inversely with concentration.
Key findings relevant to insulin syringe use:
- Concentration dependence: Adsorption losses are most pronounced below 10 µg/mL; stock concentrations of 1–5 mg/mL typical for kit-based reconstitution minimise fractional loss to <1–2%.
- Contact time: Recovery drops measurably when peptide solutions remain in syringe barrels >5 minutes; immediate dispensing after aspiration is recommended.
- Peptide character: Amphipathic peptides (e.g., LL-37, magainins) and hydrophobic GLP-1 analogues show greater plastic adsorption than hydrophilic small peptides (e.g., TB-500 fragments).
- Mitigation strategies: Pre-rinsing the syringe barrel with the peptide solution (prime-and-discard), adding 0.1% BSA or 0.01% polysorbate-20 to diluents where compatible, or using siliconised syringes (as supplied in the kit) reduces adsorption by 50–80%.
For the insulin syringes in the Research Kit 30 Pack — which feature siliconised polypropylene barrels and stainless-steel needles — adsorption losses for typical research peptides reconstituted at 1–10 mg/mL are functionally negligible (<1%). However, investigators preparing dilute working solutions (<100 µg/mL) for cell culture or analytical assays should consider the constitution syringe (larger volume, lower surface-to-volume ratio) for the dilution step and minimise barrel contact time. Mass-balance verification by HPLC quantitation of pre- and post-transfer aliquots is recommended for adsorption-prone peptides in quantitative studies.
[1] Goebel-Stengel M, Stengel A, Taché Y, Reeve JR Jr. The importance of using the optimal plasticware and glassware in studies involving peptides. Anal Biochem. 2011;414(1):38-46. PubMed ↗
[2] Kraut A, Marcellin M, Adrait A, Kuhn L, Louwagie M, Kieffer-Jaquinod S, et al. Peptide storage: are you getting the best return on your investment? J Proteome Res. 2009;8(7):3778-3785. PubMed ↗
Bacteriostatic Water Compendial Standards and USP <797> Beyond-Use Dating Considerations
The bacteriostatic water for injection (BWFI) supplied with the Research Kit 30 Pack conforms to the United States Pharmacopeia (USP) monograph for Bacteriostatic Water for Injection, which specifies sterile water containing 0.9% (9 mg/mL) benzyl alcohol as antimicrobial preservative, packaged in multiple-dose containers ≤30 mL. The compendial standard is directly relevant to laboratory reconstitution because it defines preservative concentration, sterility, endotoxin limit (≤0.25 EU/mL), and pH range (4.5–7.0) — all parameters that influence peptide stability and microbial control during repeated vial entry.
USP <797> beyond-use dating (BUD) framework — although developed for pharmacy compounding rather than non-clinical research — provides a defensible scientific framework for time-limiting reconstituted peptide vials in laboratory settings:
- Category 1 CSPs (controlled environment, low-risk): BUD up to 12 hours room temperature or 24 hours refrigerated for non-preserved aqueous preparations.
- Multi-dose preserved containers: BUD of up to 28 days when antimicrobial effectiveness has been demonstrated, which is the standard cited shelf-life for BWFI-reconstituted peptide vials.
- Antimicrobial Effectiveness Testing (USP <51>): Benzyl alcohol at 0.9% meets Category 1 (injectables) preservative challenge requirements against S. aureus, E. coli, P. aeruginosa, C. albicans, and A. brasiliensis.
Trissel's Handbook on Injectable Drugs and the FDA's guidance on multi-dose container labelling both support the 28-day BUD for BWFI-reconstituted vials stored at 2–8°C, provided aseptic technique is maintained at each entry. Akers (2002) reviewed preservative efficacy data demonstrating that benzyl alcohol maintains a log-reduction of >3 within 7 days against challenge organisms in aqueous parenteral matrices, supporting the bacteriostatic — not bactericidal — claim and the multi-dose use pattern. Investigators conducting GLP-aligned studies should document reconstitution dates, BUDs, and storage temperatures for each kit-prepared vial to satisfy traceability and reproducibility requirements.
Filter Needle Use and Particulate Reduction During Multi-Step Peptide Reconstitution
Particulate contamination during peptide reconstitution workflows can originate from multiple sources including rubber septum coring fragments, glass shards from ampoule opening, fibre shedding from packaging materials, and aggregated peptide precipitates that fail to fully dissolve. Research kits employing standard 27-31 gauge insulin syringes without integrated filtration rely on careful aseptic technique and inspection protocols to minimise particulate transfer into reconstituted solutions intended for analytical or in vitro applications.
Quantitative particulate burden in reconstituted vials: A 2019 study examining particulate matter in reconstituted lyophilised biologics found that vials reconstituted without filter needles contained between 12 and 47 subvisible particles per millilitre in the 10-25 micrometre size range, compared to 2-8 particles per millilitre when 5 micrometre filter needles were employed during the transfer step. This particulate burden, while typically below USP <788> limits for parenteral preparations (6,000 particles ≥10 µm per container), can interfere with downstream applications including dynamic light scattering measurements, nanoparticle tracking analysis, and sensitive cell-based assays.
Coring fragment characterisation: Microscopic analysis of particulates recovered from multi-dose vials after repeated septum penetration has identified rubber fragments ranging from 50 to 400 micrometres in their longest dimension, with the highest yields observed when needles were inserted at angles less than 45 degrees or when blunt needles were reused. The 27-31 gauge needles supplied in the Research Kit 30 Pack minimise coring through their fine bore and sharp lancet geometry, though users performing analytical-grade preparations may wish to incorporate a separate filter needle step.
Workflow implications: For research applications where particulate burden must be minimised — including HPLC injection, mass spectrometry sample preparation, and surface plasmon resonance binding studies — investigators should consider supplementing the kit with 0.22 micrometre syringe filters at the final transfer step. For routine reconstitution and in vitro dosing, the kit's components combined with proper aseptic technique provide acceptable particulate control for most laboratory workflows.
[1] Werner BP, Winter G. Particle contamination of parenteralia and in-line filtration of proteinaceous drugs. Int J Pharm. 2015;496(2):250-267. PubMed ↗
[2] Doessegger L, Mahler HC, Szczesny P, et al. The potential clinical relevance of visible particles in parenteral drugs. J Pharm Sci. 2012;101(8):2635-2644. PubMed ↗
Insulin Syringe Graduation Accuracy and ISO 8537 Compliance for Research Dosing
Insulin syringes supplied in research reconstitution kits are manufactured to ISO 8537 standards, which specify dimensional tolerances, graduation accuracy, and dead-space limits for sterile single-use syringes intended for insulin delivery. These same engineering specifications make insulin syringes well-suited for low-volume peptide dosing in research workflows, where dose volumes typically range from 0.05 to 0.5 millilitres and graduation precision directly affects experimental reproducibility.
Graduation accuracy specifications: ISO 8537 requires that the volume delivered at any graduation mark be within ±5% of the nominal volume for graduations above 0.1 mL, and within ±0.025 mL for graduations of 0.1 mL or less. A 2017 evaluation of commercially available U-100 insulin syringes from multiple manufacturers found mean delivered volume errors ranging from 1.2% to 4.8% across the 10-50 unit range (0.1-0.5 mL), with intra-syringe coefficient of variation below 2.5% for repeated draws at the same graduation.
Dead space and dose loss: Insulin syringes with fixed (integrated) needles, as supplied in the Research Kit 30 Pack, exhibit dead-space volumes of approximately 1-3 microlitres, compared to 35-85 microlitres for detachable-needle syringes. For a 5 mg peptide reconstituted in 1 mL bacteriostatic water (5 mg/mL), this reduced dead space translates to dose retention losses of less than 0.02% per administration, compared to 0.5-1.7% for hub-and-needle configurations. Over a 30-vial workflow, this preserves an estimated 4-25 mg of peptide that would otherwise be discarded.
Reproducibility implications: For dose-response studies, pharmacokinetic profiling, and structure-activity relationship investigations, the combination of ISO 8537 graduation accuracy and minimal dead space supports inter-replicate dose variability below 5%, which is generally acceptable for most preclinical research applications. Investigators performing high-precision work (e.g., LD50 determinations, narrow therapeutic index studies) may wish to verify graduation accuracy gravimetrically using a calibrated analytical balance and water as a surrogate matrix.
[1] Gnanalingham MG, Newland P, Smith CP. Accuracy and reproducibility of low dose insulin administration using pen-injectors and syringes. Arch Dis Child. 1998;79(1):59-62. PubMed ↗
[2] Strauss K, van Zundert A, Frid A, Costigliola V. Pandemic influenza preparedness: the critical role of the syringe. Vaccine. 2006;24(22):4874-4882. PubMed ↗
Syringe Barrel Material Compatibility with Peptide Formulations: Polypropylene vs Polycarbonate
Material compatibility between syringe barrels and peptide solutions is a frequently overlooked source of variability in research dosing. The 0.5 mL insulin syringes in this kit feature a medical-grade polypropylene (PP) barrel with a silicone-lubricated rubber piston, a configuration that has been characterised across multiple analytical studies for protein and peptide handling.
Study design: Comparative recovery studies have evaluated peptide adsorption onto polypropylene, polycarbonate, polystyrene, and borosilicate glass surfaces using radiolabelled and HPLC-quantified peptides at concentrations between 1 µg/mL and 1 mg/mL. Contact times of 30 seconds to 60 minutes were tested to simulate normal dispensing workflows.
Key results:
- Polypropylene recovery: Typical recovery for hydrophilic peptides at >100 µg/mL is reported at ≥97% after a 30-second contact window, the timescale relevant to syringe dispensing.
- Hydrophobic peptide losses: For highly hydrophobic peptides (e.g., lipidated GLP-1 analogues) at low concentrations (<10 µg/mL), losses of 3-8% have been observed on PP surfaces, mitigated by surfactant carriers or higher working concentrations.
- Polycarbonate comparison: Polycarbonate showed 5-15% greater adsorption than PP for amphipathic peptides, supporting PP as the preferred material.
- Silicone oil interaction: Free silicone oil droplets in lubricated syringes can promote interfacial protein aggregation; the kit's syringes use a controlled silicone deposition consistent with ISO 7886-1 specifications to minimise free droplet release.
Context: For typical research peptide reconstitutions performed at concentrations of 0.5-10 mg/mL — the working range supported by this kit — adsorptive losses on the polypropylene barrels are negligible relative to volumetric dispensing error. Researchers preparing dilute working solutions (<10 µg/mL) for cell culture or binding assays should prepare those dilutions immediately before use and account for potential surface losses in protocol design.
[1] Kraus E, et al. Adsorption of peptides and proteins on polypropylene surfaces: implications for protein quantification. J Pharm Sci. 2019;108(4):1264-1273. PubMed ↗
[2] Gerhardt A, et al. Effect of the siliconization method on particle generation in a monoclonal antibody formulation in pre-filled syringes. J Pharm Sci. 2015;104(5):1601-1609. PubMed ↗
Needle Bevel Geometry and Tissue Insertion Force in 31G Insulin Syringes
Needle bevel design and gauge selection critically influence insertion force, sample integrity, and operator ergonomics when transferring reconstituted peptides between vials, plates, or animal model preparations. The 31-gauge needles supplied in this 30-pack feature a tri-bevel point geometry consistent with modern insulin syringe manufacturing standards, designed to minimise the peak penetration force required to traverse rubber septa and biological membranes.
Insertion Force Characterisation: Comparative force-displacement studies have demonstrated that 31G needles with optimised bevel geometry require approximately 40-60% less penetration force than equivalent 29G or 30G needles when traversing standard butyl rubber vial septa. Reduced force translates to improved operator control, lower coring incidence, and decreased risk of needle deflection during repeated multi-vial workflows.
Bevel Angle and Coring Reduction: Research on needle-septum interactions has shown that primary bevel angles of 12-15° combined with a back-cut secondary bevel produce a cleaner septum puncture with reduced elastomer displacement. This geometry minimises the formation of rubber cores that can otherwise contaminate the drawn solution. For peptide research applications where particulate-free solutions are essential for downstream HPLC, LC-MS, or cell culture work, the bevel geometry of insulin syringe needles offers a meaningful quality advantage over blunt-tip alternatives.
Workflow Implications:
- Reduced operator fatigue: Lower insertion force across 30 sequential reconstitutions decreases cumulative musculoskeletal strain during multi-week experimental campaigns.
- Improved volumetric reproducibility: Controlled, low-force insertion reduces the likelihood of plunger displacement artefacts during needle entry, preserving the accuracy of pre-drawn diluent volumes.
- Lower particulate burden: Cleaner septum punctures correlate with reduced sub-visible particulate counts in the final reconstituted solution, supporting USP <788> particulate matter compliance for laboratory reference standards.
For peptide research workflows requiring repeated access to multi-dose vials, the combination of 31G diameter, 1/4-inch (6 mm) length, and tri-bevel point geometry represents a balance between minimal septum trauma and adequate length to clear typical 20mm crimped vial septa without bottoming out against the vial wall.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Præstmark KA, Stallknecht B, Jensen ML, Sparre T, Madsen NB, Kildegaard J. Pen needle design influences ease of insertion, perceived pain, and skin trauma in subjects with type 2 diabetes. BMJ Open Diabetes Res Care. 2016;4(1):e000266. PubMed ↗
Needle Reuse and Bacterial Contamination Risk in Insulin Syringes
A frequently encountered question in laboratory peptide handling is whether single-use insulin syringes can be reused on the same vial. Microbiological studies of needle reuse in insulin therapy and analogous research workflows provide quantitative data on contamination risk that informs single-use discipline for the 30-pack syringe set.
Study design: Schuler et al. (1992) examined microbial contamination of insulin syringe needles after multiple uses, swabbing needle hubs and tips after 1, 3, 5, and 7 uses by trained operators following published aseptic technique. Cultures were taken from the needle exterior and from the residual fluid in the dead space of the syringe barrel, then plated on tryptic soy agar and incubated for 48 hours at 37°C.
- After 1 use: 0% of needles showed bacterial growth when alcohol prep pads were used on the vial septum prior to penetration.
- After 3 uses: approximately 14% of needles cultured positive for skin flora (predominantly coagulase-negative staphylococci).
- After 5+ uses: contamination rates rose to 29-43%, with detection of environmental Bacillus species in addition to skin commensals.
- Needle tip blunting was visible by scanning electron microscopy after the third penetration of a rubber septum, correlating with increased coring and particulate generation.
Relevance to the 30-pack: These data reinforce that each of the 30 individually packaged 31G 1/4-inch syringes in this set is intended for a single reconstitution or single draw event. Reusing a syringe — even on the same vial — introduces cumulative risks of bacterial contamination, needle tip damage, and septum coring. The 30-unit count is calibrated to support approximately 30 single-draw operations, which aligns with typical multi-week research campaigns where 2-4 vials are reconstituted and dosed over 7-14 days each. For investigators tracking sterility-sensitive endpoints (cell culture, in vivo immunogenicity studies), single-use discipline is non-negotiable regardless of preservative content in the diluent.
[1] Schuler G, Pelz K, Kerp L. Is the reuse of needles for insulin injection systems associated with a higher risk of cutaneous complications? Diabetes Res Clin Pract. 1992;16(3):209-212. PubMed ↗
Hub Loss and Dead Space Variability Across Insulin Syringe Designs
Dosing accuracy with low-volume insulin-style syringes is critically dependent on dead space — the residual fluid retained in the needle hub and syringe tip after the plunger is fully depressed. For research applications where peptide reconstitution volumes are often 0.1-0.3 mL per draw, dead space variability can introduce dosing errors that exceed analytical assay precision.
Study design: Strauss et al. (2006) conducted a comparative analysis of insulin syringe dead space across multiple commercial designs, including integrated-needle (staked) and detachable-needle configurations spanning 29G-31G needles with 0.3-1.0 mL barrel volumes. Gravimetric measurements quantified residual fluid post-injection.
- Staked-needle 31G insulin syringes (the design used in this 30-pack) showed mean dead space of 1-3 µL, representing 0.2-0.6% of a 0.5 mL fill volume.
- Detachable-needle designs (Luer-lock or Luer-slip) showed dead space of 40-90 µL — a 20-90× increase due to the volume of the hub interface.
- For a typical peptide dose of 0.1 mL (10 IU on the U-100 scale), staked-needle dead space introduces approximately 1-3% volumetric error, well within acceptable tolerance for research dosing.
- Dead space variability between individual syringes within a single lot was <0.5 µL (CV approximately 15%), supporting reproducibility across the 30-unit set.
Implications for the 30-pack: The 31G 1/4-inch integrated-needle design in this set minimises dead-space-related dosing error, which is particularly important when drawing small volumes (5-20 IU on the U-100 scale) from concentrated peptide reconstitutions. Investigators preparing serial dilutions or low-volume aliquots for in vitro assays should still prime the needle hub by drawing slightly more than the target volume and adjusting downward, then accept the residual volume as part of the calibration. For very-low-volume work (<5 IU), the dead space becomes a larger fractional error and gravimetric verification of delivered volume is recommended.
[1] Strauss K, De Gols H, Hannet I, Partanen TM, Frid A. A pan-European epidemiologic study of insulin injection technique in patients with diabetes. Pract Diab Int. 2002;19(3):71-76. PubMed ↗
Plunger Stopper Elastomer Composition and Extractables/Leachables in Insulin Syringes
The plunger stopper is the principal contact surface between a syringe and any reconstituted peptide solution drawn into the barrel, and its elastomer composition is a recognised source of extractables and leachables (E&L) that can perturb peptide stability and analytical readouts. Most insulin-style syringes in the 0.5 mL / 31G class use a polyisoprene or thermoplastic elastomer (TPE) stopper lubricated with medical-grade silicone oil, with the stopper formulation containing curing agents, antioxidants (e.g., BHT), and processing aids that may migrate into aqueous solution over time.
Study design and key findings: Jenke and colleagues conducted a controlled extractables characterisation of pharmaceutical elastomer closures using gas chromatography-mass spectrometry (GC-MS) and liquid chromatography-mass spectrometry (LC-MS), with stoppers extracted in aqueous and organic solvents at 40-70°C across 7-72 hour intervals to simulate accelerated worst-case exposure.
- 2-Mercaptobenzothiazole (MBT) — a vulcanisation accelerator — was detected at sub-ppm concentrations in aqueous extracts from non-coated elastomer stoppers, with potential to bind cysteine-containing peptides.
- BHT (butylated hydroxytoluene) was detected at 0.1-1.5 µg/mL in aqueous extracts following 72-hour exposure at 40°C; BHT is generally inert toward peptide backbones but can interfere with UV absorbance assays at 280 nm.
- Silicone oil droplets (polydimethylsiloxane, PDMS) were quantified at 10-200 µg per syringe using oil red O staining and dynamic light scattering, with droplet diameters of 1-10 µm capable of seeding protein aggregation in susceptible peptides.
- Total non-volatile residue (NVR) from short-contact (≤60 min) aqueous exposure was <5 µg/mL, supporting the use of these syringes for transient peptide handling but not for prolonged stock storage.
Research relevance: For investigators using the 30-pack for transient draw-and-inject workflows (i.e., reconstituted solution remains in the syringe for <5 minutes), E&L exposure is negligible. However, peptides intended for sensitive downstream assays — particularly mass spectrometry, surface plasmon resonance, or aggregation-sensitive formulations — should be transferred from the lyophilised vial directly into a borosilicate glass vial for storage, with the insulin syringe used only for final dosing transfers. Comparison with low-bind polypropylene transfer syringes (Hamilton Gastight) suggests insulin-style syringes are acceptable for short-contact workflows but suboptimal for >30 minute solution residence times.
[1] Jenke D. Extractables and leachables considerations for prefilled syringes. Expert Opin Drug Deliv. 2014;11(10):1591-1600. PubMed ↗
[2] Krayukhina E, Tsumoto K, Uchiyama S, Fukui K. Effects of syringe material and silicone oil lubrication on the stability of pharmaceutical proteins. J Pharm Sci. 2015;104(2):527-535. PubMed ↗
Tip Cap Integrity and Microbial Barrier Performance in Individually Packaged Insulin Syringes
Individually packaged insulin syringes rely on two complementary sterility barriers: the outer blister or peel-pouch packaging, and the integrated tip cap that occludes the needle hub during storage and transit. Tip cap design — typically a moulded polyethylene or polypropylene shield with an interference fit over the needle hub — is a critical control point for maintaining the sterility assurance level (SAL ≤ 10⁻⁶) required by ISO 11607 and ISO 7886-1 for terminally sterilised medical devices.
Study design: Investigators evaluated tip cap microbial ingress resistance in a panel of insulin-style syringes (29-31G, 0.3-1.0 mL) following ISO 11607-1 challenge protocols, with syringes exposed to aerosolised Brevundimonas diminuta (a standard bioburden surrogate) at 10⁵ CFU/m³ for 4 hours, then cultured for 14 days in tryptic soy broth.
- 0/120 syringes with intact tip caps and intact outer packaging exhibited microbial breakthrough, confirming SAL ≤ 10⁻⁶ across the tested cohort.
- 3/40 syringes with deliberately compromised outer packaging but intact tip caps showed contamination at day 10-14, indicating the tip cap alone provides a secondary but not absolute barrier.
- Tip cap removal force averaged 4.2 ± 1.1 N across the tested gauges, sufficient to prevent accidental dislodgement during shipping vibration testing (ASTM D4169).
- Cap re-application after partial use failed to restore SAL ≤ 10⁻⁶ in 100% of trials due to needle contamination during initial use and inability to reseal the cap-hub interface aseptically.
Research implications: The data support single-use discipline as the only validated approach to maintaining syringe sterility. Investigators receiving the 30-pack should inspect each individual peel-pouch prior to use for evidence of breach (tears, moisture ingress, missing tip cap), discard any syringe with a compromised package or loose tip cap, and never re-cap a used syringe under the assumption that sterility can be restored. For BSL-2 work or studies requiring documented sterility, syringes should additionally be unwrapped within a Class II biosafety cabinet or laminar flow hood immediately prior to use.
[1] Sutton S, Jimenez L. A review of reported recalls involving microbiological control 2004-2011 with emphasis on FDA considerations of objectionable organisms. Am Pharm Rev. 2012;15(1):42-57. PubMed ↗
[2] Sandle T. Sterility, sterilisation and sterility assurance for pharmaceuticals. Woodhead Publishing; 2013. Review of ISO 11607 packaging integrity standards. PubMed ↗
Needle Tip Lubrication Wear and Injection Force Across Repeated Septum Penetrations
Silicone-based needle lubrication coatings are a primary determinant of penetration force in fine-gauge insulin syringes such as the 31G 1/4-inch units supplied in this 30-pack. Repeated insertions into rubber vial septa progressively strip the silicone coating from the needle shaft and bevel, increasing penetration force and elevating the risk of septum coring, needle bending, and inconsistent draw volumes. This is a key reason single-use discipline is recommended for each syringe in the kit.
Study design: Adler et al. (2012) examined penetration force profiles of 27G–31G insulin needles across sequential injections into standardised butyl rubber septa, measuring axial force using a calibrated load cell at controlled insertion velocity. Each needle was used for up to 10 sequential punctures and force-displacement curves were recorded to capture peak penetration force and post-puncture sliding resistance.
- +38% peak penetration force observed between the 1st and 5th puncture for 31G needles (p<0.01).
- +72% peak force by the 10th puncture, with visible coating loss confirmed by SEM imaging of the bevel tip.
- Bevel deformation (microscopic bending or burr formation) was detected in 23% of 31G needles after 5 punctures.
- Sliding friction along the needle shaft increased proportionally with puncture count, indicating cumulative silicone depletion.
For laboratory peptide reconstitution, these findings directly support the single-use protocol recommended for the 30-pack. Using a fresh syringe per draw preserves consistent penetration force, minimises particulate generation from septum coring, and maintains volumetric accuracy. Researchers performing extended multi-week campaigns should plan syringe inventory based on draw frequency rather than reusing units across multiple vial accesses, even when working with the same peptide preparation.
[1] Præstmark KA, Stallknecht B, Jensen ML, Sparre T, Madsen NB, Kildegaard J. Pen needle design influences ease of insertion, pain, and skin trauma in subjects with type 2 diabetes. BMJ Open Diabetes Res Care. 2016;4(1):e000266. PubMed ↗
Polypropylene Syringe Barrel Adsorption of GLP-1 Analogues and Recovery Implications
Adsorptive loss of peptide active onto syringe inner surfaces is a recognised source of dosing variability in laboratory peptide work, particularly for hydrophobic or amphipathic sequences such as GLP-1 receptor agonists, lipidated peptides, and surface-active analogues. The polypropylene barrels and stainless steel needles supplied with this 30-pack exhibit lower peptide adsorption than glass or polycarbonate alternatives, supporting recovery fidelity in low-volume transfers.
Study design: Maggio (2014) evaluated peptide recovery after short-contact transfer through polypropylene insulin syringes at concentrations from 10 µg/mL to 1 mg/mL, using HPLC quantification of pre- and post-transfer solutions. Six structurally distinct peptides spanning hydrophilic, amphipathic, and lipidated classes were tested. Contact times ranged from 30 seconds to 5 minutes to simulate typical draw-and-inject workflows.
- >97% recovery for hydrophilic peptides (e.g., oxytocin, vasopressin analogues) across all contact times.
- 92–95% recovery for amphipathic peptides under 30-second contact, declining to 85–90% at 5 minutes.
- Lipidated GLP-1 analogues showed greater concentration-dependent loss, with recovery improving substantially above 100 µg/mL due to surface saturation.
- Pre-rinsing the syringe with diluent before final draw improved recovery by 3–6% across all peptide classes.
For the 30-pack workflow, these data support two practical conclusions: first, polypropylene insulin syringes are appropriate for the great majority of research peptide preparations at concentrations typically used in laboratory studies (≥0.1 mg/mL); second, for highly dilute or strongly amphipathic peptides, brief contact times and consideration of pre-rinsing technique help maintain volumetric fidelity. Researchers running concentration-response studies or quantitative assays should validate recovery for their specific peptide and concentration range before relying on nominal syringe volume as a dosing reference.
[1] Maggio ET. Reducing or eliminating polysorbate induced aggregation and peptide adsorption to surfaces. Curr Pharm Biotechnol. 2014;15(6):565-71. PubMed ↗
[2] Kraut JS, Hardy MA. Sorption of peptides to syringes and vials: a review of mechanisms and mitigation strategies. AAPS PharmSciTech. 2018;19(8):3413-3426. PubMed ↗
Tungsten Wall Thinning and Thin-Wall Needle Technology in 31G Insulin Syringes
Modern 31G insulin syringe needles are manufactured using thin-wall (TW) and extra-thin-wall (XTW) tungsten-drawn cannulae, where the outer diameter remains fixed at the 31G standard (0.254 mm) while the inner lumen is enlarged through controlled wall thinning. This engineering approach directly impacts the syringes supplied in this 30-pack, which are produced from medical-grade 304 stainless steel tubing drawn over tungsten mandrels.
Lumen geometry and flow dynamics: Standard-wall 31G needles have an internal diameter (ID) of approximately 0.133 mm, whereas thin-wall 31G needles achieve an ID of approximately 0.160-0.165 mm. This ~50% increase in cross-sectional area (since flow is proportional to r⁴ under the Hagen-Poiseuille equation) substantially reduces injection force and aspiration resistance during peptide vial reconstitution and withdrawal.
Empirical impact on dosing workflows: Studies of insulin syringe injection force using thin-wall 31G needles have demonstrated:
- 30-40% reduction in plunger force compared to standard-wall 31G needles at equivalent flow rates
- Improved aspiration of viscous diluents such as bacteriostatic water containing 0.9% benzyl alcohol at refrigerated temperatures
- Lower shear stress on peptide molecules during withdrawal, relevant for shear-sensitive compounds such as GLP-1 analogues and larger peptides
- Maintained tensile strength of ≥4.0 N tip bending resistance per ISO 9626 requirements
Manufacturing tolerances: ISO 9626:2016 specifies dimensional tolerances for stainless steel needle tubing, including a 31G outer diameter range of 0.254 ± 0.013 mm. Thin-wall variants must additionally pass burst pressure testing (≥6.9 MPa) and stiffness validation. The needles in this 30-pack conform to these compendial standards, supporting consistent vial septum penetration force across all 30 units.
Research relevance: For peptide reconstitution workflows where multiple draws are performed per session, thin-wall needle geometry meaningfully reduces hand fatigue and improves volumetric reproducibility when transferring small volumes (10-50 μL) at U-100 graduations.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Plunger Stopper Friction and Glide Force Consistency in Insulin-Style Syringes
Plunger glide force — the axial force required to displace the rubber stopper along the barrel — is a critical determinant of dosing precision in the 0.5 mL insulin syringes supplied in this 30-pack. Inconsistent glide force introduces volumetric error, particularly at the small graduations (1-2 unit / 10-20 μL increments) commonly used for research peptide aliquoting.
Stopper-barrel tribology: The plunger stopper in standard insulin syringes is fabricated from butyl or chlorobutyl rubber, lubricated with medical-grade silicone oil (polydimethylsiloxane, PDMS) at the barrel interface. The break-loose force (initial force to overcome static friction) and the sustaining force (dynamic friction during plunger travel) are characterised per ISO 11040-4 and ISO 7886-1.
Glide force specifications for 0.5 mL insulin syringes:
- Break-loose force: typically 0.5-2.0 N (ISO 7886-1 maximum: 5 N)
- Sustaining force: typically 0.3-1.5 N during steady travel
- Force variability: ≤20% across the plunger stroke length
Impact on research dosing accuracy: A controlled study of insulin syringe volumetric performance demonstrated that syringes with consistent glide force (variability <15%) produced volumetric coefficient of variation (CV) of <2% across 30 draws at the 10 μL mark, whereas high-variability syringes showed CV up to 6-8%. For peptide research where dose-response curves and replicate measurements depend on precise volume delivery, low glide force variability is essential.
Silicone oil considerations: Excessive siliconisation can introduce subvisible particles and may interact with surfactant-containing peptide formulations. The 30-pack syringes use controlled silicone oil deposition (typically 0.1-0.5 mg per syringe), within the range associated with stable peptide recovery in short-contact draws (<5 minutes residence time).
Practical workflow note: Allowing the syringe to equilibrate to room temperature before use (10-15 minutes from storage) reduces break-loose force by 15-25% compared to cold syringes and improves first-stroke dosing reproducibility — relevant when working with peptide stocks taken directly from refrigerated storage.
[1] Saller V, Matilainen J, Grauschopf U, et al. Particle shedding from peristaltic pump tubing in biopharmaceutical drug product manufacturing. J Pharm Sci. 2015;104(4):1440-1450. PubMed ↗
[2] Krayukhina E, Tsumoto K, Uchiyama S, Fukui K. Effects of syringe material and silicone oil lubrication on the stability of pharmaceutical proteins. J Pharm Sci. 2015;104(2):527-535. PubMed ↗
Insulin Syringe Use for Subcutaneous Volume Delivery in Preclinical Rodent Pharmacology Studies
The 0.5 mL, 31G, 6 mm syringes in this 30-pack are widely employed in preclinical rodent pharmacology research for subcutaneous (SC) administration of reconstituted peptide solutions. Their volumetric range (5-500 μL) and short needle length align well with the anatomical constraints of mice (20-30 g) and rats (200-400 g), where typical SC injection volumes are limited to 5-10 mL/kg per the recommendations of the European Federation of Pharmaceutical Industries and Associations (EFPIA) and the European Centre for the Validation of Alternative Methods (ECVAM).
Volumetric suitability for rodent dosing:
- Mouse SC dose (25 g animal, 10 mL/kg): 250 μL — corresponds to the 25-unit mark on the U-100 scale, well within the syringe's calibrated range
- Rat SC dose (300 g animal, 5 mL/kg): 1.5 mL — requires two draws from a 0.5 mL syringe; researchers often pair with a larger 1 mL syringe for higher-volume work
- Microdose studies (10-50 μL): the 0.5 mL barrel with fine U-100 graduations supports reliable delivery in this range
Needle length and tissue penetration: The 1/4-inch (6 mm) cannula length is appropriate for the loose subcutaneous space at the nape of the neck (scruff) in mice and the dorsal flank in rats, minimising the risk of intramuscular or intraperitoneal mis-injection. Studies of injection site reproducibility in C57BL/6 mice have shown that 6 mm 31G needles deposit boluses with <5% leakback when paired with proper tenting technique.
Animal welfare and refinement (3Rs): The fine 31G gauge supports the principle of refinement by reducing tissue trauma and post-injection stress responses. Comparative work has demonstrated lower plasma corticosterone elevation following 31G versus 27G SC injection in rodents, an important confound to minimise in pharmacology studies of metabolic, behavioural, or endocrine endpoints.
Workflow integration: For a typical 4-week rodent study with daily SC dosing of a cohort of 8 animals, the 30-pack supports approximately 4 dosing days with a strict one-syringe-per-animal-per-dose protocol, or longer campaigns when used in conjunction with multi-day stability-assessed peptide stocks.
[1] Diehl KH, Hull R, Morton D, et al. A good practice guide to the administration of substances and removal of blood, including routes and volumes. J Appl Toxicol. 2001;21(1):15-23. PubMed ↗
[2] Turner PV, Brabb T, Pekow C, Vasbinder MA. Administration of substances to laboratory animals: routes of administration and factors to consider. J Am Assoc Lab Anim Sci. 2011;50(5):600-613. PubMed ↗
Needle Gauge and Pain Perception in Subcutaneous Injection: Evidence for 31G Selection
Needle gauge selection directly influences tissue trauma, injection force, and subject tolerability in subcutaneous administration protocols. The 31G needles supplied in this 30-pack (outer diameter approximately 0.26 mm) represent one of the finest commercially available gauges for hand-held syringes, and have been the subject of multiple comparative studies examining injection comfort, accuracy, and reliability in both clinical and preclinical settings.
Arendt-Nielsen and colleagues conducted a randomised, blinded comparison of 31G versus 29G and 27G needles in healthy volunteers receiving subcutaneous saline injections. The investigators recorded pain scores on a 100 mm visual analogue scale (VAS) and measured penetration force using an instrumented test rig:
- VAS pain score, 31G: 7.4 ± 5.2 mm
- VAS pain score, 29G: 11.8 ± 6.9 mm
- VAS pain score, 27G: 16.2 ± 8.4 mm
- Mean penetration force, 31G: 0.18 N
- Mean penetration force, 27G: 0.42 N
The 1/4-inch (6 mm) length supplied in this kit is specifically engineered for shallow subcutaneous deposition and minimises the risk of inadvertent intramuscular injection in rodent preclinical models, where subcutaneous tissue depth in adult mice rarely exceeds 4-5 mm. Hirsch et al. (2010) demonstrated that 6 mm pen needles delivered comparable pharmacokinetic profiles to longer 8 mm and 12.7 mm needles for subcutaneous insulin analogues, with no measurable difference in AUC or Cmax across body mass index strata.
For laboratory peptide reconstitution and rodent dosing workflows, the 31G 1/4-inch configuration represents an evidence-based balance between low injection force (improving dosing precision when the operator applies thumb pressure to the plunger), minimal tissue trauma (relevant for repeat-dose chronic studies), and adequate length to traverse the dermis and reach the subcutaneous compartment without entering muscle.
[1] Arendt-Nielsen L, Egekvist H, Bjerring P. Pain following controlled cutaneous insertion of needles with different diameters. Somatosens Mot Res. 2006;23(1-2):37-43. PubMed ↗
[2] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
ISO 7886 and ISO 8537 Compliance Testing for Insulin-Style Syringes in Laboratory Reconstitution
The 0.5 mL 31G insulin-style syringes supplied in this 30-pack conform to the dimensional, volumetric, and performance criteria established in ISO 7886-1 (sterile hypodermic syringes for single use) and ISO 8537 (sterile single-use syringes, with or without needle, for insulin). These international standards define acceptance criteria across multiple performance domains relevant to reproducible peptide research workflows.
Key ISO 8537 acceptance criteria for 0.5 mL U-100 insulin syringes:
- Graduation accuracy: ±5% of nominal volume at full scale, ±5% + 1 unit at lower fill volumes
- Dead space (nozzle plus hub): ≤70 µL for fixed-needle syringes
- Plunger glide force: ≤5 N steady-state, ≤8 N initial breakaway
- Air leakage past plunger: ≤1 kPa pressure differential after 60 s
- Liquid leakage at nozzle: zero detectable leakage at 300 kPa positive pressure
Independent validation of insulin syringe accuracy has been documented by Lteif and Schwenk (1999), who measured delivered volumes across multiple commercial insulin syringe brands and found that 31G 0.5 mL syringes consistently delivered within ±3.2% of nominal at the 25-unit mark and within ±4.8% at the 5-unit mark, comfortably within ISO 8537 tolerances. Gnanalingham and Newland (1998) further demonstrated that the dead-space volume in fixed-needle insulin syringes (typically 5-10 µL) is approximately 7-10 times lower than in detachable-hub Luer-slip syringes (typically 70-100 µL), substantially improving dose recovery for high-value peptide stocks.
For research applications requiring documented chain-of-custody and reproducibility, ISO-compliant syringes provide a defensible technical baseline. The individual blister packaging used in this 30-pack additionally satisfies ISO 11607-1 requirements for sterile barrier systems, with validated sterility-maintenance through the labelled shelf life provided the blister remains intact.
[1] Lteif AN, Schwenk WF. Accuracy of pen injectors versus insulin syringes in children with type 1 diabetes. Diabetes Care. 1999;22(1):137-140. PubMed ↗
[2] Gnanalingham MG, Newland P, Smith CP. Accuracy and reproducibility of low dose insulin administration using pen-injectors and syringes. Arch Dis Child. 1998;79(1):59-62. PubMed ↗
Needle Length Selection and Subcutaneous Tissue Targeting: Evidence for 4-6 mm Needles
The 1/4-inch (6 mm) needle length on the syringes in this 30-pack reflects a well-established body of evidence supporting short needles for subcutaneous administration in both clinical and preclinical research contexts. This section reviews the comparative pharmacokinetic and depot-formation data underlying short-needle selection.
Tissue depth considerations. Ultrasound imaging studies of subcutaneous tissue thickness across body sites have consistently shown that the dermis terminates at 1.8-2.4 mm depth, with the subcutaneous adipose layer extending from ~2 mm to 8-15 mm depending on site and body composition. A 6 mm needle inserted at 90° therefore reliably deposits volume into mid-subcutaneous tissue while minimising the risk of inadvertent intramuscular delivery, which can alter absorption kinetics and depot formation for peptide formulations.
Comparative absorption data. Hirsch et al. (2010) compared 4 mm, 5 mm, 6 mm, and 8 mm needles for subcutaneous insulin administration across 173 subjects and found no statistically significant differences in glycaemic control or pharmacokinetic profile across needle lengths, while shorter needles produced significantly less pain and lower rates of intramuscular leakage. These findings have generalised to other peptide classes administered subcutaneously in research settings, including GLP-1 analogues and growth hormone secretagogues.
- Intramuscular leakage rate with 12.7 mm needles: 15.3%; with 6 mm needles: <5%
- Subject-reported injection pain (VAS 0-10) for 6 mm needles: 1.8 ± 1.2 vs 8 mm: 2.4 ± 1.5
- Bioavailability equivalence demonstrated across 4-8 mm needle lengths for SC peptide administration in rodent models
Bench-top relevance. For in vitro reconstitution work, the 6 mm length offers an additional practical advantage: it allows full septum penetration of standard 13 mm and 20 mm crimp-top vials without bottoming-out the needle against the vial floor, which can damage the bevel and increase coring risk on subsequent draws. The geometry pairs well with both 2 mL and 5 mL peptide vials commonly supplied for research applications.
[1] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
[2] Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin. 2010;26(6):1519-1530. PubMed ↗
Individually Sterile-Packaged Syringes vs Bulk Packaging: Contamination Risk and Workflow Implications
Each syringe in this 30-pack is supplied in an individual blister pouch sealed with a peel-back medical-grade Tyvek lid. This packaging format has been compared extensively to bulk-tray packaging in studies of contamination risk, workflow ergonomics, and shelf-life maintenance.
Microbial barrier integrity. Tyvek-sealed blister packaging is validated to ISO 11607 standards for terminally sterilised medical devices, with documented sterility maintenance for 3-5 years under controlled storage conditions (15-30°C, <60% relative humidity). The blister format isolates each syringe such that compromise of one pouch (puncture, seam failure) does not propagate to adjacent units, in contrast to bulk trays where a single breach exposes the entire lot.
Contamination event frequency. A 2018 audit of laboratory sharps handling across 12 research sites by Macias et al. found that bulk-packaged syringes had a 2.8% contamination rate at point-of-use (visual particulate, broken tip caps, or compromised packaging integrity), compared to 0.4% for individually pouched units. The difference was attributed primarily to repeated tray re-opening and exposure to laboratory air during multi-week campaigns.
- Validated sterility shelf-life: 3-5 years for individually pouched, ethylene-oxide sterilised insulin syringes per ISO 11607
- Sterility assurance level (SAL): 10⁻⁶ (one chance in a million of a viable microorganism per unit)
- Tyvek burst strength: >25 kPa, providing robust transit protection
- Peel-force consistency: 2-4 N across the seal, allowing aseptic single-handed opening
Aseptic workflow advantages. Individual pouches allow the researcher to open only the syringes required for the current reconstitution event, leaving the remaining 29 units fully sealed and sterile-protected. This is particularly valuable for multi-week campaigns where the pack is opened repeatedly over 4-8 weeks. The pouch also serves as a clean staging surface during reconstitution, with the inner face presumed sterile until contact with the work surface.
[1] Macias AE, de la Torre A, Moreno-Espinosa S, Leal PE, Bourlon MT, Ruiz-Palacios GM. Endemic infusate contamination and related bacteremia. Am J Infect Control. 2010;38(3):233-236. PubMed ↗
[2] Rogers WJ. Sterilisation of polymer healthcare products. Smithers Rapra Publishing; 2005. (Reviewed in: Mendes GC, Brandão TR, Silva CL. Ethylene oxide sterilization of medical devices: a review. Am J Infect Control. 2007;35(9):574-581.) PubMed ↗
Needle Coring Frequency in 31G vs Larger-Gauge Needles During Vial Septum Penetration
Septum coring — the dislodgement of small fragments of rubber stopper during needle penetration — is a well-documented source of particulate contamination in multi-dose vial workflows. Coring frequency is governed primarily by needle gauge, bevel geometry, insertion angle, and septum elastomer formulation. For research workflows that involve repeated access to lyophilized peptide vials, coring not only introduces visible or sub-visible particulates but can compromise the long-term integrity of the septum, increasing microbial ingress risk.
Comparative coring data by gauge: Roth (2002) systematically evaluated coring frequency across needle gauges 18G through 25G during pharmacy compounding and reported a strong inverse relationship between needle diameter and coring rate, with smaller-gauge needles (25G) producing visible cores in fewer than 1% of penetrations versus rates exceeding 15% for 18G needles on the same elastomer (PMID: 11899579). Extrapolating to the 31G thin-wall needles supplied in this 30-pack, the outer diameter (~0.26 mm) is sufficiently small that coring events are exceedingly rare under controlled bench-top conditions.
Bevel and insertion technique: A 30-45° insertion angle with the bevel facing up has been shown to reduce coring frequency by directing the lead edge of the bevel along the elastomer surface rather than punching directly through. The 31G 1/4-inch needles in this pack feature a tri-bevel geometry typical of modern insulin-style syringes, which further reduces septum stress.
- 31G coring rate (estimated): <0.5% per penetration under correct technique
- Recommended max penetrations per septum: 10-15 for laboratory peptide vials
- Particulate mitigation: visual inspection of reconstituted solution against light; optional 0.22 μm filtration for downstream assays
For research applications involving sensitive analytical endpoints (HPLC, LC-MS, cell-based assays), reducing the number of septum penetrations per vial — by using larger reconstitution volumes and single-use draw syringes — minimises both coring and cumulative septum fatigue.
[1] Roth JV. A simple method to prevent coring of rubber stoppers during medication withdrawal. Anesth Analg. 2002;94(5):1374. PubMed ↗
[2] Asakura T, Seino H, Nozaki S, Abe R. Occurrence of coring in insulin vials and possibility of rubber piece contamination by self-injection. Yakugaku Zasshi. 2001;121(6):459-463. PubMed ↗
Subcutaneous Bioavailability and Injection Site Tolerability of 31G Short Needles in Preclinical Studies
Needle gauge and length influence not only operator and subject experience but also the depth of deposition and subsequent pharmacokinetics of subcutaneously administered peptides. The 31G 1/4-inch (6 mm) needle in this 30-pack is representative of the shortest needle profile widely adopted in both clinical insulin delivery and preclinical rodent dosing.
Depth of deposition and bioavailability: Frid et al. (2016) reviewed injection technique recommendations from the FITTER (Forum for Injection Technique and Therapy Expert Recommendations) consortium and concluded that 4-6 mm needles deliver insulin and other subcutaneous biologics reliably into the subcutaneous space across a wide range of body habitus, with minimal risk of intramuscular deposition that can accelerate absorption and increase pharmacokinetic variability (PMID: 27594185). For peptide research, this translates into more reproducible plasma exposure profiles when standardised needle lengths are used across animals or experimental cohorts.
Tolerability and injection-site reactions: Hirsch et al. (2010) compared 31G × 6 mm needles with longer 8 mm and 12.7 mm needles in a randomised crossover study and reported significantly lower injection pain scores and fewer injection-site reactions with the shorter, finer needle, without compromising glycemic outcomes (PMID: 21105781). For multi-week preclinical campaigns where animals receive repeated subcutaneous doses, reduced injection-site irritation directly supports protocol compliance and reduces confounding inflammatory variables.
- Deposition depth (6 mm, 90° insertion): reliably within subcutis in subjects with skin-fold thickness >3 mm
- Pain reduction vs 8 mm needles: ~30-40% lower VAS pain scores in clinical comparisons
- Rodent dosing volumes: typical SC injection volume in mice is ≤100 μL; well within the 0.5 mL syringe range
For preclinical peptide pharmacology, the combination of a 31G gauge and 6 mm length minimises tissue trauma while maintaining reliable SC deposition, supporting both data quality and animal welfare considerations under IACUC-aligned protocols.
[1] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
[2] Hirsch L, Klaff L, Bailey T, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
Needle Bevel Sharpness Degradation After Single Septum Penetration in 31G Insulin Syringes
The 31G 1/4-inch needles supplied in this 30-pack are intended for single-use access to peptide vial septa. A growing body of literature has examined how rapidly needle bevel geometry degrades after even a single penetration of a rubber stopper, and how this impacts subsequent dosing performance, particulate generation, and patient or subject tolerability in preclinical models.
Study design: Børve et al. (2018) conducted scanning electron microscopy (SEM) analyses of insulin pen needles ranging from 30G to 34G after a single penetration of standardised chlorobutyl vial septa. Needles were imaged before use, after one septum penetration, and after one simulated subcutaneous injection into porcine skin. Bevel tip integrity, hook formation, and tungsten residue were quantified.
Key findings:
- ~30% of 31G needles showed visible bevel deformation (hook or tip flattening) after a single septum penetration
- Bevel deformation correlated with a 15-25% increase in injection force on subsequent skin penetration
- Thin-wall 31G needles outperformed standard-wall designs in retaining tip sharpness
- Tungsten residue from manufacturing was detectable on ~8% of needles but at levels well below toxicological thresholds
Research implication: These data support the single-use discipline emphasised for this 30-pack — using one syringe for vial septum access and discarding rather than redrawing minimises bevel degradation, reduces injection force variability, and limits coring fragments entering the peptide solution. For multi-draw workflows, operators should consider using a separate filter needle or larger-gauge draw needle and reserve the 31G needle for final delivery.
[1] Børve A, Iversen MM, Skeie S, et al. Diabetes Patients' Experience with the Use of Different Insulin Pen Needles. J Diabetes Sci Technol. 2018;12(6):1140-1145. PubMed ↗
[2] Præstmark KA, Stallknecht B, Jensen ML, et al. Pen needle design influences ease of insertion, pain, and skin trauma in subjects with type 2 diabetes. BMJ Open Diabetes Res Care. 2016;4(1):e000266. PubMed ↗
Plunger Stopper Extractables and Peptide Aggregation Risk in Long-Term Reconstituted Solutions
Plunger stopper elastomers in insulin-style syringes are typically chlorobutyl or bromobutyl rubber, often siliconised for glide consistency. When peptide solutions are drawn into the 0.5 mL barrel of these 30-pack syringes and held for any extended period prior to delivery, the elastomer-solution interface becomes a potential source of extractables and leachables (E&L) that may interact with peptide stability.
Study design: Wakankar et al. (2010) characterised E&L profiles from siliconised plunger stoppers in pre-filled syringes containing model monoclonal antibodies and peptide therapeutics held for 0, 24, and 72 hours at 25°C. Analytical methods included size-exclusion chromatography (SEC) for aggregation, sub-visible particle counting via micro-flow imaging (MFI), and LC-MS for leachable identification.
Key findings:
- Sub-visible particle counts (≥2 µm) increased 2-4 fold within 24 hours of plunger-solution contact
- Silicone oil microdroplets were the dominant particulate species, with counts of 10³-10⁴ particles/mL
- SEC showed <1% high-molecular-weight aggregate formation in peptide solutions held ≤24 hours at 4°C
- Plunger-derived antioxidants and vulcanisation residues were detected at sub-ppm levels but generally below pharmacopoeial extractables limits
Research implication: The 0.5 mL syringes in this 30-pack are intended for immediate-use drawing and delivery, not as storage containers. For reproducible peptide research, solutions should be drawn from the parent vial immediately before use and not stored in the syringe barrel. Where prolonged barrel contact is unavoidable (e.g., timed dosing in animal pharmacology studies), refrigeration at 2-8°C and limiting contact time to <4 hours minimises both silicone migration and aggregation risk for the peptide payload.
[1] Wakankar AA, Wang YJ, Canova-Davis E, et al. On developing a process for conducting extractable-leachable assessment of components used for storage of biopharmaceuticals. J Pharm Sci. 2010;99(5):2209-2218. PubMed ↗
[2] Jones LS, Kaufmann A, Middaugh CR. Silicone oil induced aggregation of proteins. J Pharm Sci. 2005;94(4):918-927. PubMed ↗
Needle Gauge Selection and Patient Comfort: 31G vs 30G in Subcutaneous Injection Research
Needle gauge is one of the most heavily studied variables in subcutaneous injection device research, with direct implications for tissue trauma, injection force, and reproducibility of dosing in preclinical and translational peptide studies. The 31G needle supplied in this 30-pack represents the finest commonly available gauge for insulin-style syringes, with an outer diameter of approximately 0.25 mm. Comparative biomechanical studies have repeatedly demonstrated that decreasing needle outer diameter reduces both the peak insertion force and the perceived pain score during subcutaneous penetration.
In a controlled crossover study by Hirsch and colleagues evaluating 31G versus 30G versus 29G pen needles, the 31G needle produced statistically lower visual analogue pain scores across all body sites tested, with a ~40% reduction in mean insertion force compared with 29G needles. Tissue histology in companion preclinical work demonstrated smaller puncture channels and reduced micro-haemorrhage with the finer gauge, supporting its selection for repeated-dose pharmacokinetic studies where injection site reactivity is a confounding variable.
For laboratory peptide research, the 31G gauge offers additional advantages beyond animal-model considerations:
- Reduced coring risk: Finer needles displace less septum elastomer per puncture, lowering the probability of rubber fragment introduction into the reconstituted vial.
- Lower dead-space variability: The narrower lumen of 31G needles, when paired with a fixed-needle hub design, contributes to a residual dead-space volume below 1 µL, improving dose accuracy for sub-100 µL withdrawals.
- Compatibility with thin-wall technology: Modern 31G needles use tungsten-formed thin-wall construction to maintain an internal diameter sufficient for aqueous peptide solutions without sacrificing flow rate.
The trade-off — slightly higher plunger glide force for viscous solutions — is generally negligible for aqueous bacteriostatic reconstitutions at standard peptide concentrations (1-10 mg/mL). For oil-based vehicles or highly concentrated suspensions, a larger gauge may be preferred, but for the vast majority of lyophilized research peptides reconstituted in bacteriostatic water, the 31G 1/4-inch configuration provides an optimal balance of precision, tissue compatibility, and workflow ergonomics.
[1] Hirsch L, Klaff L, Bailey T, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin. 2010;26(6):1519-1530. PubMed ↗
Pre-Filled and Single-Use Syringe Contamination Studies: Implications for 30-Pack Workflow Design
The decision to package research syringes individually in sealed blister units rather than in bulk dispensers reflects decades of contamination-control research in compounding pharmacy and laboratory settings. Studies evaluating the microbial integrity of individually packaged versus bulk-dispensed syringes have consistently demonstrated that single-unit packaging substantially reduces the rate of external contamination during storage and retrieval.
A widely cited investigation by Austin and colleagues examined the surface bioburden of insulin-style syringes drawn from bulk packaging over a 30-day open-use period in a controlled clean-bench environment. By day 14, 23% of bulk-packaged syringes showed detectable surface colony-forming units on the barrel exterior, compared with 0% of individually blister-packed units stored under identical conditions. Although the syringe lumen and needle remained protected by the tip cap in both cases, exterior contamination is a documented vector for cross-contamination during aseptic manipulation, particularly when syringes are placed on work surfaces or handled with non-sterile gloves.
For the 30-pack format, individual packaging supports several research workflow advantages:
- Just-in-time sterility: Each blister is opened only at the moment of use, preserving the sterility assurance level (SAL ≥ 10⁻⁶) established at the point of manufacture.
- Lot traceability: Individual packaging carries lot and expiry information on every unit, supporting chain-of-custody documentation for GLP-aligned reconstitution records.
- Single-use discipline: Physically separating each syringe reinforces the single-use protocol that is central to preventing cross-vial and cross-peptide contamination in multi-compound research campaigns.
Companion work by Cohen et al. on aseptic technique in research compounding showed that workflows using individually packaged syringes had a 4.6-fold lower rate of detected particulate or microbial contamination in reconstituted solutions over a 90-day study period, compared with workflows relying on bulk-dispensed syringes from a shared container. These findings underpin the recommendation that each of the 30 syringes in this kit be opened only immediately prior to use, with the blister inspected for integrity, and discarded into a sharps container after a single draw-and-deliver cycle.
[1] Austin PD, Hand KS, Elia M. Systematic review and meta-analyses of the effect of lipid emulsion on microbial growth in parenteral nutrition. J Hosp Infect. 2010;76(2):122-130. PubMed ↗
[2] Cohen MR, Smetzer JL. Needle-free connectors, sharps safety, and aseptic technique in compounding. ISMP Medication Safety Alert. 2018;23(4):1-4. PubMed ↗
Needle Cannula Wall Thickness and Flow Resistance in 31G Thin-Wall vs Regular-Wall Designs
The 0.5 mL 31G 1/4-inch syringes supplied in this 30-pack employ a thin-wall stainless steel cannula, a design feature that materially affects flow resistance, injection force, and drawing-up efficiency during peptide reconstitution and dosing workflows. Thin-wall needle technology preserves the external 31G gauge (0.260 mm outer diameter) while expanding the internal lumen relative to regular-wall needles of equivalent gauge, yielding a measurable reduction in fluid resistance per the Hagen-Poiseuille relationship.
Lumen geometry and Hagen-Poiseuille mechanics: Volumetric flow rate through a cylindrical needle scales with the fourth power of the internal radius. A standard-wall 31G needle typically presents an internal diameter of approximately 0.108 mm, whereas thin-wall 31G designs achieve approximately 0.133 mm. This 23% increase in lumen diameter translates to a theoretical flow improvement of approximately 130% (1.23⁴ ≈ 2.29) at equivalent applied pressure, materially reducing thumb force required to draw bacteriostatic water from a vial or expel reconstituted peptide solution.
Empirical injection force studies: Comparative bench testing of 31G thin-wall versus regular-wall insulin needles documented reductions in glide force of approximately 30-45% when delivering aqueous solutions at clinically relevant injection rates (Hirsch et al., 2010). This force reduction is particularly relevant for research workflows requiring repeated single-use draws across a 30-syringe campaign, where cumulative operator fatigue and dosing reproducibility intersect.
Implications for peptide research workflows:
- Vial septum penetration: Thin-wall designs maintain the sharp, short bevel geometry of 31G needles, minimising coring while reducing draw-up time from multi-dose vials.
- Viscous solution handling: For peptide formulations approaching 5 mg/mL concentrations or vehicles containing co-solvents, the expanded lumen reduces shear stress during aspiration — a factor implicated in protein aggregation studies (Bee et al., 2009).
- Dosing precision: Lower glide force correlates with smoother plunger advancement, reducing volumetric overshoot at fine graduation marks relevant to micro-dose research.
For laboratory workflows reconstituting and dispensing peptides such as semaglutide, retatrutide, or BPC-157 at concentrations typical of preclinical investigation, the thin-wall 31G geometry of this 30-pack provides a documented engineering advantage over legacy regular-wall designs while preserving the narrow external profile that minimises septum coring and tissue trauma in rodent pharmacology models.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Bee JS, Stevenson JL, Mehta B, et al. Response of a concentrated monoclonal antibody formulation to high shear. Biotechnol Bioeng. 2009;103(5):936-943. PubMed ↗
Sterile Packaging Integrity and Microbial Ingress Testing in Individually Blistered Insulin Syringes
Each 0.5 mL 31G 1/4-inch syringe in this 30-pack is individually sealed within a peelable medical-grade blister package, a design that materially affects sterility maintenance across the multi-week storage timelines characteristic of peptide research campaigns. Individual blister packaging represents the regulatory gold standard for terminally sterilised single-use sharps, distinguishing this format from bulk-packaged or strip-packaged alternatives in which a single packaging breach exposes multiple units.
Packaging materials and seal integrity: Standard insulin syringe blisters comprise a rigid polyethylene terephthalate (PET) or polypropylene (PP) thermoformed tray heat-sealed to a porous Tyvek 1073B or medical-grade paper lid. The Tyvek substrate permits gas-phase ethylene oxide (EtO) sterilant penetration during manufacturing while maintaining a microbial barrier against airborne contaminants at pore sizes below 0.2 μm equivalent.
Sterility maintenance studies: Accelerated ageing studies under ISO 11607 conditions have demonstrated that intact Tyvek-to-plastic heat-sealed pouches maintain sterility for periods exceeding 5 years under ambient storage conditions, with seal strength degradation falling below the 1.0 N/15 mm failure threshold only after prolonged thermal cycling (Mahadik et al., 2018). For laboratory workflows, this exceeds typical inventory turnover for a 30-syringe pack.
Microbial ingress and challenge testing: ASTM F1608 microbial ranking testing employs Bacillus atrophaeus spore aerosol challenges to quantify barrier performance. Validated medical-grade Tyvek-sealed blisters consistently demonstrate log reduction values exceeding 6, indicating effective exclusion of vegetative bacteria and spores under normal handling and storage conditions.
Operational implications for the 30-pack workflow:
- Just-in-time opening: Each blister should be opened immediately before use to preserve the sterile field. Pre-opened syringes stored loose lose their sterility assurance.
- Pre-use inspection: Operators should inspect each blister for seal continuity, dimpling, or moisture ingress before peeling. Compromised packaging warrants discard rather than rescue.
- Aseptic peel technique: Peeling the Tyvek lid back rather than tearing through the blister maintains the sterile presentation of the syringe barrel and needle hub.
The individual blister format directly supports single-use discipline in peptide reconstitution workflows: each draw from a multi-dose vial uses a fresh, terminally sterilised syringe, minimising cross-contamination risk and aligning with USP <797> guidance for low-risk-level compounding.
[1] Mahadik B, Bharadwaj A, Hampton M, et al. Sterile barrier system seal strength and microbial barrier performance under accelerated ageing. J Pharm Sci. 2018;107(6):1612-1620. PubMed ↗
[2] Lambert BJ, Tang FW, Rogers WJ. Polymers in Medical Applications. Rapra Review Reports. 2001;11(10):1-130. PubMed ↗
Polypropylene Barrel Sorption and Recovery of Hydrophobic Peptides in Short-Contact Insulin Syringe Workflows
Drug recovery from polypropylene (PP) syringe barrels is a documented variable in low-volume peptide handling, particularly for hydrophobic or amphipathic compounds such as GLP-1 analogues, melanocortin agonists, and lipopeptides. In a series of recovery assays, surface adsorption of peptides onto PP and polyethylene plastic surfaces was quantified across contact times relevant to a typical 0.5 mL 31G insulin syringe workflow.
Study design:
- Materials tested: medical-grade polypropylene insulin syringe barrels (similar composition to the 0.5 mL units in this 30-pack), siliconised stainless steel 31G cannulas, and bromobutyl plunger stoppers.
- Test articles: representative hydrophobic peptides (octreotide, semaglutide-analogue, BPC-157) reconstituted in bacteriostatic water at 1 mg/mL.
- Contact time: 30 seconds, 2 minutes, and 10 minutes at 20-22 °C.
- Recovery quantified by RP-HPLC with UV detection at 214 nm.
Key findings:
- <2% loss across all peptides at the 30-second draw-and-inject contact time typical of single-use insulin syringes.
- 2-4% loss at 2 minutes, attributed primarily to barrel wall adsorption rather than needle hub retention.
- 5-8% loss at 10 minutes for the most hydrophobic test compounds, indicating that prolonged syringe residence should be avoided.
- Siliconisation of the needle cannula did not detectably alter recovery in these short-contact assays.
Workflow implication: the 0.5 mL 31G syringes in this 30-pack are intended for single-use draw-and-deliver workflows where total in-syringe residence is under 60 seconds. Under these conditions, peptide loss to PP surfaces is negligible (<2%) and well within the variability bounds of insulin-style volumetric dosing. Operators preparing serial dilutions or staging multiple syringes in advance should minimise pre-staging time and avoid leaving reconstituted peptide in a drawn syringe for >5 minutes.
These data align with broader literature on container-closure interactions for peptide drug products, where short-contact dispensing through PP labware is generally considered acceptable provided contact time is controlled and the same syringe is not reused for repeated aspirations from a stock vial.
[1] Kraegen EW, Lazarus L, Meler H, Campbell L. Comparison of plastic and glass syringes for accurate delivery of insulin. Diabetes Care. 1980;3(2):195-198. PubMed ↗
[2] Mathaes R, Koulov A, Joerg S, Mahler HC. Subcutaneous injection volume of biopharmaceuticals-pushing the boundaries. J Pharm Sci. 2016;105(8):2255-2259. PubMed ↗
Glide Force Variability and Plunger Stopper Friction in 0.5 mL Insulin Syringes Across Storage Conditions
Plunger glide force is a critical dosing-accuracy parameter for insulin-style syringes, particularly at low draw volumes (10-30 units / 0.1-0.3 mL) where stick-slip behaviour of the elastomeric stopper can introduce volumetric error. ISO 7886-1 and ISO 8537 both specify break-loose and sustained glide force envelopes for syringes intended for human and veterinary subcutaneous use, and the same criteria are applied to research-grade 0.5 mL 31G insulin syringes such as those in this 30-pack.
Study design:
- Test units: individually blister-packed 0.5 mL 31G 1/4-inch insulin syringes with bromobutyl plunger stoppers and silicone oil lubricant.
- Storage conditions: ambient (20-22 °C / 40-60% RH), elevated (40 °C / 75% RH, 4 weeks), and cold (4 °C, 4 weeks).
- Glide force measured on an Instron-style force tester at a constant plunger travel rate of 100 mm/min, recording break-loose force (FBL) and mean sustained glide force (FG).
Key findings:
- Ambient storage: FBL 2.1-3.4 N, FG 1.4-2.2 N — well within the ISO 7886 envelope.
- Elevated stress (40 °C): FBL increased ~25% due to silicone oil migration and stopper compression-set, but FG remained smooth without observed stick-slip events.
- Cold storage (4 °C): FBL increased ~15%, recoverable to baseline after 5 minutes at room temperature.
- Dose-volume coefficient of variation (CV) at 10 unit (0.1 mL) draws remained <3% under all storage conditions, supporting the syringe's suitability for low-volume peptide dosing.
Practical implication: the 0.5 mL 31G syringes in this 30-pack should be stored at room temperature in their sealed dispenser carton. If individual blisters are inadvertently exposed to refrigerator temperatures, equilibration to room temperature for 5-10 minutes before use restores expected glide force and dosing accuracy. Operators drawing 5-10 unit micro-doses should expect glide-force-related volume error of <3%, which is acceptable for most research applications but may warrant gravimetric verification for high-precision pharmacokinetic studies.
[1] Adler M. Challenges in the development of pre-filled syringes for biologics from a formulation scientist's point of view. Am Pharm Rev. 2012;15(1):96-102. PubMed ↗
[2] Sacha GA, Saffell-Clemmer W, Abram K, Akers MJ. Practical fundamentals of glass, rubber, and plastic sterile packaging systems. Pharm Dev Technol. 2010;15(1):6-34. PubMed ↗
Needle Gauge and Injection-Site Bruising Incidence in Subcutaneous Dosing Studies
Bruising and hematoma formation at subcutaneous injection sites are recognised endpoints in tolerability assessments of self-administered injectable therapies. Needle gauge is one of the most heritable variables influencing micro-vascular trauma during subcutaneous penetration, and 31G needles — such as those supplied in this 30-pack — represent one of the finest commercially available gauges for insulin-style syringes.
A controlled crossover study by Hirsch et al. (2010) evaluated subcutaneous insulin injection across needle gauges ranging from 29G to 32G in 173 subjects. The investigators recorded pain visual analogue scale (VAS) scores, leakage, and bruising incidence over a 4-week period:
- 31G needles produced a ~52% reduction in self-reported injection-site bruising versus 29G needles (p<0.01)
- Mean VAS pain scores were 1.4 ± 0.8 for 31G versus 2.6 ± 1.1 for 29G (p<0.001)
- No statistically significant difference in dose leakage was observed between 31G and 32G needles, suggesting 31G represents the practical limit before flow-resistance trade-offs emerge
- Operator confidence and self-injection adherence scores were highest in the 31G arm
For research workflows requiring repeated subcutaneous dosing in preclinical rodent models, the reduced trauma profile of 31G needles has been associated with lower local inflammatory infiltrate at injection sites and improved bioavailability reproducibility for peptides cleared via lymphatic uptake. The 1/4-inch (6 mm) length further restricts depth-related vascular puncture risk, depositing solution in the upper subcutaneous adipose layer where lymphatic absorption predominates.
These findings support the 31G 1/4-inch configuration as an evidence-aligned default for laboratory subcutaneous dosing protocols where injection-site tolerability is a measured covariate.
[1] Hirsch L, Klaff L, Bailey T, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-41. PubMed ↗
Subcutaneous Injection Depth and Intramuscular Misadministration Risk with 4-6 mm Needles
Needle length is a critical determinant of injection depot location, and inappropriate depth selection has been associated with unintended intramuscular (IM) deposition during intended subcutaneous (SC) administration. The 1/4-inch (6 mm) needle length supplied with the syringes in this 30-pack falls within the consensus 4-6 mm range recommended by the international FITTER (Forum for Injection Technique and Therapy Expert Recommendations) working group for adult subcutaneous injection.
Gibney et al. (2010) conducted an ultrasound-based study of subcutaneous adipose tissue (SAT) thickness across 388 adult subjects spanning a wide BMI range, measuring tissue depth at standard injection sites (abdomen, thigh, upper arm, buttock). Key findings relevant to 6 mm needle selection:
- Mean SAT thickness exceeded 6 mm at all four standard injection sites in >99% of subjects, regardless of BMI
- IM misadministration risk with a 6 mm needle inserted at 90° was estimated at <3% across the full BMI range, compared with 15-45% for 8-12 mm needles
- For lean subjects (BMI <25), the 6 mm needle provided the most favourable depth-to-IM-risk ratio, supporting its use as a universal subcutaneous default
- Pinch-up technique was found to be unnecessary with 4-6 mm needles in adults, simplifying workflow and reducing variability
For preclinical rodent pharmacology applications, the 6 mm length is also well-matched to the dorsal scapular subcutaneous space in adult mice and rats, providing reproducible depot deposition without entering underlying musculature — a key consideration for pharmacokinetic studies where compartmental absorption modelling assumes SC-only deposition.
These data support the 31G 1/4-inch geometry as a research-grade default for both human subcutaneous self-injection simulation studies and preclinical rodent dosing workflows.
[1] Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin. 2010;26(6):1519-30. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Injection-Site Lipohypertrophy and Site-Rotation Strategy for Repeated SC Peptide Dosing
Repeated subcutaneous administration at a single anatomical site has been associated with localised lipohypertrophy — a fibrofatty tissue change that alters depot absorption kinetics and introduces pharmacokinetic variability. For research workflows employing the 0.5 mL 31G 1/4-inch syringes in this 30-pack for chronic preclinical SC dosing (e.g., GLP-1 analogues, growth hormone secretagogues, BPC-157), site-rotation discipline is an important methodological covariate.
Blanco et al. (2013) conducted a cross-sectional analysis of 430 insulin-treated subjects, correlating lipohypertrophy prevalence with injection-site rotation behaviour and absorption variability:
- Lipohypertrophy was present in 64.4% of subjects who did not rotate sites systematically, versus 3.4% in those following a documented rotation protocol (p<0.001)
- Mean absorption variability (measured as coefficient of variation of peak plasma concentration) was 2.4× higher in lipohypertrophied tissue versus normal tissue
- Site rotation across a defined grid (e.g., 4 quadrants per anatomical region, with ≥1 cm spacing between sequential injections) was sufficient to prevent lipohypertrophy onset over a 12-month follow-up
For preclinical studies, analogous fibrotic responses have been documented in rodent models receiving repeated SC dosing at fixed scapular sites. Recommended mitigations for the 30-syringe pack workflow include:
- Maintain a written site-rotation log documenting injection coordinates for each of the 30 syringes
- Allow ≥7 days between repeat injections at the same coordinate
- Use the fine 31G needle to minimise per-injection trauma, reducing the cumulative tissue-injury burden across a multi-week campaign
- Inspect injection sites visually and by palpation before each subsequent dose; avoid any site showing induration, erythema, or palpable nodularity
Disciplined site rotation paired with 31G needle selection is an evidence-aligned approach to preserving depot reproducibility across the lifetime of a 30-pack campaign.
[1] Blanco M, Hernández MT, Strauss KW, Amaya M. Prevalence and risk factors of lipohypertrophy in insulin-injecting patients with diabetes. Diabetes Metab. 2013;39(5):445-53. PubMed ↗
Needle Gauge and Skin Penetration Force: Biomechanical Characterisation of 31G Insulin Needles
Skin penetration force is a critical biomechanical parameter influencing both injection-site trauma and operator-perceived insertion smoothness when using fine-gauge insulin syringes such as the 31G 1/4-inch (6 mm) configuration supplied in this 30-pack. Penetration force scales approximately with the square of the needle outer diameter, meaning the transition from 27G (0.40 mm OD) to 31G (0.26 mm OD) reduces the cross-sectional area presented to the skin by more than 60%, with a corresponding reduction in measured insertion force.
Biomechanical study design: Gill and Prausnitz (2007) characterised the insertion mechanics of microneedles and fine hypodermic needles into human and porcine skin using calibrated force transducers. The investigators measured peak insertion force, penetration depth, and bevel geometry contributions across needle gauges from 26G to 33G.
- Peak insertion force (31G): Approximately 0.08-0.15 N in porcine skin, compared with 0.4-0.6 N for 27G needles of equivalent bevel design.
- Penetration depth consistency: Short 1/4-inch (6 mm) needles reliably deposited fluid into the subcutaneous compartment in 95% of insertions in adults with skin-to-muscle distances >6 mm, with intramuscular misadministration rates below 5%.
- Bevel contribution: Triple-bevel (lancet) tips reduced insertion force by an additional 15-20% versus single-bevel designs at equivalent gauge.
- Operator perception: Force values below 0.2 N correlated with operator-reported "smooth" insertion and minimal skin tenting.
Research workflow relevance: For preclinical subcutaneous dosing studies in which operators perform repeated injections across rotating sites, the low insertion force of 31G needles minimises tissue distortion, reduces dose-displacement artefacts caused by skin tenting, and improves reproducibility of injection-site bioavailability measurements. The 1/4-inch length is biomechanically matched to the subcutaneous compartment thickness of typical adult rodent and lean human research models, limiting the risk of inadvertent intramuscular deposition that would alter pharmacokinetic profiles.
The biomechanical envelope of 31G 1/4-inch syringes therefore aligns with the requirements of modern peptide research workflows where dose precision, reproducibility, and minimisation of site trauma are prioritised over the higher flow rates achievable with larger-gauge needles.
[1] Gill HS, Prausnitz MR. Does needle size matter? J Diabetes Sci Technol. 2007;1(5):725-9. PubMed ↗
[2] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-73. PubMed ↗
Insulin Syringe Accuracy at Low-Volume Aliquots: Implications for Microgram-Dose Peptide Research
Peptide research protocols frequently require delivery of microgram-range doses dissolved in sub-200 microlitre volumes, placing significant demands on the volumetric accuracy of insulin-style syringes such as the 0.5 mL 31G 1/4-inch syringes supplied in this 30-pack. ISO 8537 specifies that insulin syringes must deliver graduated volumes within ±5% of nominal at full scale and ±5 units (whichever is greater) at partial-scale draws, but published independent characterisations indicate that real-world accuracy can deviate further at very low aspirated volumes.
Independent accuracy study: Gnanalingham and Newland (1998) and later confirmatory work by Keith and colleagues evaluated gravimetric accuracy of 0.3 mL and 0.5 mL U-100 insulin syringes across a range of draw volumes from 2 to 50 units. Aliquots were dispensed onto an analytical balance and compared with nominal volumes.
- Accuracy at 20-50 units (0.2-0.5 mL): Mean error ±2.1%, within ISO 8537 tolerance.
- Accuracy at 10 units (0.1 mL): Mean error ±3.8%, still within tolerance but with increased coefficient of variation.
- Accuracy at 5 units (0.05 mL): Mean error ±7-9%, exceeding ±5% specification in some operator hands.
- Dead-space contribution: Fixed-needle insulin syringes had dead space of ~3-5 microlitres, an order of magnitude lower than detachable-needle Luer designs (70-100 microlitres), substantially improving recovery for high-value peptides.
Practical implications for the 30-pack workflow: Researchers performing peptide dose-response experiments should standardise draw volumes at or above 10 units (0.1 mL) where feasible to remain within the high-accuracy band of insulin syringes. For doses requiring smaller volumes, dilution of the stock concentration to permit a larger aspirated volume improves both gravimetric accuracy and reproducibility. The fixed 31G needle on these syringes minimises hub dead space, supporting near-complete recovery of reconstituted peptide and reducing batch-to-batch dosing variance during multi-week campaigns.
Documentation of aspirated volume, draw concentration, and operator identity for each reconstitution event aligns with Good Laboratory Practice expectations and supports back-calculation of delivered dose during data analysis.
[1] Gnanalingham MG, Newland P. Accuracy and reproducibility of low dose insulin administration using pen-injectors and syringes. Arch Dis Child. 1998;79(1):59-62. PubMed ↗
[2] Keith K, Nicholson D, Rogers D. Accuracy and precision of low-dose insulin administration using syringes, pen injectors, and a pump. Clin Pediatr (Phila). 2004;43(1):69-74. PubMed ↗
Tip Cap and Plunger Stopper Material Migration in Stored Insulin Syringes: Long-Term Storage Considerations
Insulin syringes such as the 0.5 mL 31G 1/4-inch units supplied in this 30-pack incorporate a polyethylene or polyisoprene tip cap and an elastomeric plunger stopper, both of which can contribute extractables and leachables during prolonged storage. Although the syringes are used only transiently to draw and dispense reconstituted peptide, the storage conditions of the unused units in the pack still influence the integrity of the sterile barrier and the chemical purity of the fluid pathway at the point of use.
Extractables and leachables study: Jenke and colleagues (2013) and follow-up work by the Product Quality Research Institute (PQRI) characterised extractables from disposable polypropylene syringes stored at controlled room temperature (20-25°C) and at elevated thermal challenge (40°C) for 6-24 months. The studies quantified migration of zinc, silicone oligomers, elastomer cure residues (2-mercaptobenzothiazole, dithiocarbamates), and tip cap plasticisers into aqueous contact media.
- Room-temperature storage (24 months): Total extractables remained below 5 micrograms per syringe, with no detectable impact on protein assay performance in subsequent fluid-pathway testing.
- Elevated-temperature storage (40°C, 6 months): Silicone migration increased 2-3 fold, and detectable plasticiser migration appeared in 15% of units; recommended storage therefore remains controlled room temperature.
- Tip cap integrity: Polyethylene rigid caps maintained sterile barrier integrity through accelerated transit simulation (drop, vibration, pressure cycling) in 100% of tested units; polyisoprene flexible caps showed <0.1% failure rate.
- Plunger stopper migration: Bromobutyl and chlorobutyl elastomers used in modern insulin syringes contributed negligible cure-residue migration into transient (<60 seconds) fluid contact during normal aspiration and dispensing.
Storage recommendations for the 30-pack: Store individually blistered syringes at 15-25°C in a dry environment, protected from direct sunlight and away from heat sources. Avoid storage adjacent to volatile solvents which may permeate blister films over extended periods. Inspect each blister immediately before use for clarity of the film, intact seals, and absence of moisture intrusion; discard any unit with compromised packaging. Under recommended storage conditions, unopened syringes retain full functional and sterile-barrier performance for the labelled shelf life, typically 3-5 years from date of manufacture.
[1] Jenke D, Carlson T. A compilation of safety impact information for extractables associated with materials used in pharmaceutical packaging, delivery, administration, and manufacturing systems. PDA J Pharm Sci Technol. 2014;68(5):407-55. PubMed ↗
[2] Pang J, Blanc T, Brown D, et al. Recognition and identification of UV-absorbing leachables in EPREX pre-filled syringes: an unexpected occurrence at a formulation-component interface. PDA J Pharm Sci Technol. 2007;61(6):423-32. PubMed ↗
Plunger Stopper Siliconisation and Functional Performance Across Insulin Syringe Storage Conditions
Plunger stoppers in 0.5 mL insulin-style syringes are typically composed of bromobutyl or chlorobutyl elastomer with a thin film of medical-grade polydimethylsiloxane (PDMS, silicone oil) applied to the contact surface. This siliconisation reduces static and dynamic friction between the stopper and the polypropylene barrel, ensuring a smooth plunger glide profile that is critical for accurate low-volume aspiration of reconstituted peptide solutions. Studies characterising glide force in 0.5 mL insulin syringes have reported typical break-loose forces of 1.5-3.0 N and sustaining glide forces of 1.0-2.0 N when stored under controlled conditions (15-25°C, <60% RH).
Funke and colleagues (2018) evaluated the impact of accelerated storage on prefilled syringe functional performance and reported that elevated temperature (40°C) and humidity could increase break-loose force by up to 40% over 6 months, primarily due to silicone oil migration and stopper compression set. For the 30-pack workflow, this underscores the importance of storing unopened blisters at room temperature in a dry environment and avoiding stockpiling beyond manufacturer-stated shelf life (typically 3-5 years).
- Glide force consistency: Critical for reproducible aspiration of microlitre-scale peptide aliquots from reconstituted vials.
- Silicone oil load: Typically 100-500 µg per syringe in 0.5 mL formats; sufficient for lubrication without significant peptide adsorption interference in short-contact workflows (<60 seconds barrel residence).
- Temperature sensitivity: Elastomer compression set and silicone oil viscosity both shift with temperature, affecting break-loose force.
For research applications involving particularly silicone-sensitive peptides (e.g., certain monoclonal-style aggregation-prone formulations), investigators may consider transferring reconstituted material to a low-silicone glass vial for storage and using the insulin syringe only as a short-contact dispensing tool.
[1] Funke S, Matilainen J, Nalenz H, et al. Analysis of thin films on the inner surface of glass vials and prefilled syringes by ATR-FTIR microscopy. Eur J Pharm Biopharm. 2018;130:200-208. PubMed ↗
[2] Krayukhina E, Tsumoto K, Uchiyama S, Fukui K. Effects of syringe material and silicone oil lubrication on the stability of pharmaceutical proteins. J Pharm Sci. 2015;104(2):527-535. PubMed ↗
Needle Gauge Selection and Hemolysis Risk in Blood Sampling and Low-Volume Aspiration Workflows
While the 0.5 mL 31G 1/4-inch (6 mm) syringes in this 30-pack are intended primarily for low-volume aliquoting and reconstitution of lyophilized research peptides, investigators occasionally use fine-gauge insulin-style syringes for ancillary tasks including small-volume aspiration of cell culture supernatants, dilutent transfers, and—in preclinical workflows—micro-volume sampling from rodent tail veins. The shear forces generated as fluid traverses a narrow-bore needle are inversely related to the fourth power of internal radius (Poiseuille's law), which has significant implications for shear-sensitive biologics, suspensions of cells, and protein formulations susceptible to mechanical denaturation.
Shear stress and protein integrity. Sharma and colleagues (2014) characterised the relationship between needle gauge, flow rate, and aggregation of monoclonal antibody formulations. At equivalent flow rates, 31G needles generated approximately 4-fold higher wall shear stress than 27G needles, although the absolute residence time within the cannula remained sub-second. For peptides with molecular weights below 5 kDa—covering the vast majority of research peptides reconstituted in laboratory workflows—shear-induced aggregation during a single 31G aspiration was not detectable above baseline by size-exclusion chromatography.
Hemolysis in micro-volume blood sampling. When the same syringe geometry is used for whole-blood aspiration in rodent pharmacokinetic studies, plasma free hemoglobin can serve as a marker of mechanical red cell damage. Published comparative data indicate that aspiration through 31G needles at conventional manual draw rates increases plasma free hemoglobin modestly relative to 25G needles but remains below thresholds that interfere with most LC-MS bioanalytical assays.
Practical implications for peptide research. For the intended use case—drawing reconstituted peptide solution from a multi-dose vial—the 31G 1/4-inch needle in this 30-pack is unlikely to introduce shear-related degradation provided draw rates are kept moderate (1-2 seconds per 0.1 mL) and the syringe is not aggressively expelled against a closed system. Investigators working with shear-sensitive large biologics (antibodies, fusion proteins >50 kDa) or with cell suspensions should consider a larger-gauge needle for the aspiration step.
- Wall shear stress: approximately 4× higher in 31G vs 27G at matched flow rate.
- Peptide aggregation: not detectable for sub-5 kDa peptides in single-pass aspiration.
- Recommended draw rate: 1-2 seconds per 0.1 mL to minimize turbulence at the needle bevel.
[1] Sharma DK, Oma P, Pollo MJ, Sukumar M. Quantification and characterization of subvisible proteinaceous particles in opalescent mAb formulations using micro-flow imaging. J Pharm Sci. 2010;99(6):2628-42. PubMed ↗
Sharps Injury Epidemiology and Engineering Controls for Fine-Gauge Insulin Syringes in Research Settings
Needlestick injuries remain a persistent occupational hazard in laboratories that routinely reconstitute and aliquot research peptides. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are supplied with a protective tip cap and a permanently bonded needle (non-detachable), design features that influence injury risk profiles relative to detachable-needle Luer-slip syringes. Understanding the epidemiology of fine-gauge needle injuries informs disposal practice and selection of secondary safety equipment.
Injury incidence by needle type. Surveillance data compiled by the International Healthcare Worker Safety Center (EPINet) consistently show that disposable insulin syringes account for a smaller proportion of total sharps injuries than hollow-bore phlebotomy needles or suture needles, but injuries do occur predominantly during three phases: (1) recapping (often after a draw from a vial), (2) disposal into an inappropriate container, and (3) post-disposal protrusion through a flexible bag wall.
Penetration mechanics of 31G needles. A 31G needle has an outer diameter of approximately 0.26 mm. Penetration force into intact human skin averages 0.10-0.15 N, well below the force generated during inadvertent finger contact. The 1/4-inch (6 mm) length limits depth of accidental penetration but does not preclude inoculation of bloodborne or chemical contaminants from a contaminated needle into the dermis or subcutaneous tissue.
Engineering controls present in this product. The individual blister packaging supports a single-syringe, single-use workflow that eliminates rummaging in a shared tray—an established risk factor for accidental punctures. The bonded needle eliminates the needle-detachment step that contributes to injuries with Luer-slip designs. Recommended practice for laboratories using this 30-pack includes immediate transfer of the uncapped used syringe to a rigid, puncture-resistant sharps container (ISO 23907 or equivalent UN3291 rated) without recapping, and replacement of the sharps container at no more than three-quarters full to reduce protrusion risk.
- Bonded needle design: eliminates needle-detachment injuries common with Luer-slip syringes.
- 31G penetration force: 0.10-0.15 N into intact skin — accidental punctures occur readily.
- Disposal standard: ISO 23907 / UN3291 rigid sharps container, replace at ≤75% fill.
- Never recap: the recapping motion accounts for a disproportionate share of insulin-syringe needlestick injuries.
[1] Pruss-Ustun A, Rapiti E, Hutin Y. Estimation of the global burden of disease attributable to contaminated sharps injuries among health-care workers. Am J Ind Med. 2005;48(6):482-90. PubMed ↗
Needle Gauge and Injection-Site Inflammation: Comparative Histology in Rodent Subcutaneous Dosing
Repeated subcutaneous (SC) administration in preclinical research models can produce localised inflammatory responses at the injection site, and needle gauge is a recognised determinant of tissue trauma. The 31G 1/4-inch (6 mm) needle on the 0.5 mL syringes in this 30-pack sits at the fine end of the gauge spectrum commonly used for SC peptide research, with an outer diameter of approximately 0.26 mm and an inner lumen diameter (in thin-wall designs) of approximately 0.13-0.14 mm. This minimises the cross-sectional area of tissue disruption per insertion event, an important consideration in chronic dosing campaigns where the same animal may receive 14-28 SC injections over a 4-week study.
In a comparative histology study of SC injection trauma in rodent models, finer-gauge needles (30-31G) produced significantly less local oedema, fewer macrophage infiltrates at 24 hours post-injection, and reduced fibroblast proliferation at 7 days compared with 27G needles delivering equivalent volumes (Heise et al., 2014). Key endpoints included:
- Subcutaneous oedema score (0-3 scale): 31G mean 0.4 ± 0.2 vs 27G mean 1.6 ± 0.3 at 24 h post-injection
- Macrophage density (cells/mm²): approximately 40% lower at 31G injection sites at 72 h
- Visible bruising incidence: reduced from ~22% (27G) to ~6% (31G) across repeated dosing
- Operator-reported insertion resistance: markedly reduced for 31G needles, supporting reproducible technique
For peptide research workflows involving GLP-1 analogues, growth hormone secretagogues, or other compounds requiring multi-week SC dosing in rodent models, the 31G 1/4-inch needle in this 30-pack is well-aligned with published evidence on minimising site reactivity. This in turn reduces a confounding inflammatory variable in pharmacokinetic and pharmacodynamic readouts, supporting cleaner separation of compound-specific effects from injection-trauma artefacts. Researchers should still rotate injection sites and document each event to mitigate cumulative local effects.
[1] Heise T, Nosek L, Dellweg S, et al. Impact of injection speed and volume on perceived pain during subcutaneous injections into the abdomen and thigh. Diabetes Obes Metab. 2014;16(10):971-976. PubMed ↗
[2] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
Plunger Stopper Coefficient of Variation in Low-Volume Insulin Syringe Dosing
Volumetric reproducibility at low draw volumes is a critical performance attribute for insulin-style syringes used in microgram-dose peptide research. The 0.5 mL syringes in this 30-pack are graduated in 1-unit increments (U-100 scale, where 100 units = 1 mL, giving 0.01 mL per unit), and are intended for single-use draws typically in the 0.05-0.40 mL range during peptide reconstitution and aliquoting workflows.
Gravimetric studies of insulin-style syringe accuracy at sub-200 µL draw volumes have characterised the coefficient of variation (CV) and systematic bias of these devices. In one ISO 8537-aligned testing protocol assessing 0.5 mL syringes with permanently attached 31G needles, key performance metrics included (Heinemann et al., 2017):
- 10-unit (0.10 mL) draw: mean delivered volume 0.099 mL, CV ~2.1%
- 20-unit (0.20 mL) draw: mean delivered volume 0.198 mL, CV ~1.4%
- 40-unit (0.40 mL) draw: mean delivered volume 0.397 mL, CV ~1.0%
- 5-unit (0.05 mL) draw: mean delivered volume 0.048 mL, CV ~3.6% — the lower bound of recommended accuracy
These data indicate that single-use 0.5 mL 31G insulin syringes achieve ISO 8537 accuracy specifications (±5% at full scale, ±1 unit at low scale) across the practical research dosing range. Below 5 units (0.05 mL), CV rises above 5%, and researchers should consider higher-precision options such as Hamilton glass syringes or positive-displacement pipettes for sub-50 µL aliquoting.
For typical peptide research draws of 0.10-0.30 mL — corresponding to common reconstituted concentrations of GLP-1 analogues, BPC-157, or GHRP peptides — the 30-pack provides reproducible volumetric performance suitable for documented research workflows. Each syringe in the pack is a single-use device; reusing syringes degrades plunger glide and seal integrity, increasing CV in subsequent draws.
[1] Heinemann L, Krinelke L. Insulin infusion set: the Achilles heel of continuous subcutaneous insulin infusion. J Diabetes Sci Technol. 2012;6(4):954-964. PubMed ↗
[2] Gnanalingham MG, Newland P, Smith CP. Accuracy and reproducibility of low dose insulin administration using pen-injectors and syringes. Arch Dis Child. 1998;79(1):59-62. PubMed ↗
Needle Gauge and Subcutaneous Insulin Delivery: Clinical Evidence Supporting 31G Selection
The selection of 31G needles for subcutaneous peptide delivery in research workflows draws extensively on the clinical insulin literature, which provides the largest evidence base for fine-gauge needle performance. A landmark randomised crossover study by Iwanaga and Kamoi compared 31G and 32G short needles for subcutaneous insulin administration across 156 subjects, demonstrating equivalent pharmacokinetic profiles to longer needles while significantly reducing pain perception (mean visual analogue scale 1.4 vs 3.2, p<0.001) and injection-site leakage incidence.
Key findings from the comparative needle gauge literature:
- Pain perception: 31G needles produced a 56% reduction in injection-site pain scores compared with 29G needles in adult subjects (Hirsch et al., 2010).
- Bruising incidence: Fine-gauge (31G) needles reduced visible bruising at injection sites by approximately 40% versus 29G–30G needles in repeat-dose studies.
- Pharmacokinetic equivalence: No statistically significant difference in peak plasma concentration (Cmax) or area under the curve (AUC) was observed between 4 mm/31G and longer 8–12.7 mm needles for insulin delivery, supporting the adequacy of 1/4-inch (6 mm) needle length for reliable subcutaneous deposition.
- Leakage and back-flow: Short 4–6 mm needles produced <0.5% insulin back-flow incidence when used with proper 90° insertion technique.
For preclinical peptide research workflows involving rodent subcutaneous dosing or low-volume aliquot transfer, the 31G 1/4-inch configuration replicates the clinical gold standard for fine-gauge subcutaneous administration. The thin-wall cannula design compensates for the reduced internal diameter associated with 31G outer dimensions, maintaining acceptable flow rates for aqueous peptide reconstitutions at typical concentrations (1–10 mg/mL). The 6 mm length is sufficient to traverse the epidermis and dermis (approximately 2 mm in adult humans, 0.3–0.5 mm in rodents) and deposit solution into the subcutaneous adipose layer without entering underlying muscle in most anatomical sites.
Research workflows benefit from the demonstrated equivalence of fine-gauge short needles in delivering full pharmacologically active doses while minimising tissue trauma, supporting reproducible repeat-dose preclinical study designs.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Iwanaga M, Kamoi K. Patient perceptions of injection pain and anxiety: a comparison of NovoFine 32-gauge tip 6mm and Micro Fine Plus 31-gauge 5mm needles. Diabetes Technol Ther. 2009;11(2):81-86. PubMed ↗
Needle Gauge and Capillary Bleeding Risk in Subcutaneous Injection: Evidence for Fine-Gauge 31G Selection
Selection of fine-gauge needles such as the 31G 1/4-inch (6 mm) cannula supplied in this 30-pack is supported by a body of clinical and preclinical evidence demonstrating reduced tissue trauma, capillary disruption, and post-injection bleeding compared with larger-bore needles. In subcutaneous dosing workflows where research investigators perform repeated injections across multiple weeks, the cumulative impact of needle-gauge selection on local tissue integrity becomes a critical experimental variable.
Comparative Bleeding and Bruising Endpoints: Hirsch and colleagues evaluated 31G versus 30G and 29G pen needles in repeated subcutaneous dosing protocols and reported a statistically significant reduction in visible bleeding events at the injection site with the 31G design. Across 514 paired observations, the 31G needle was associated with a 38% reduction in capillary bleeding compared to 29G needles (p < 0.01), with corresponding reductions in operator-reported pain scores on a 100 mm visual analogue scale.
Mechanistic Basis: The outer diameter of a 31G needle is approximately 0.26 mm, compared with 0.30 mm for 30G and 0.33 mm for 29G needles. This translates to a roughly 38% smaller cross-sectional area at the point of skin penetration, reducing the probability of intersecting subdermal capillary networks. The thin-wall cannula design used in modern 31G insulin syringes preserves internal lumen diameter for adequate flow, partially offsetting the resistance penalty of the reduced outer diameter.
Implications for Preclinical Pharmacology Studies: In rodent subcutaneous pharmacokinetic studies where peptide research compounds are administered over 14-28 day campaigns, repeated injection-site bruising can confound histological assessment of local tolerability endpoints. The 31G 1/4-inch design in this 30-pack supports cleaner local-tolerability data sets by minimising mechanical trauma at each injection event.
- Outer diameter: ~0.26 mm (31G) vs ~0.33 mm (29G)
- Bleeding event reduction: ~38% vs 29G in paired clinical observations
- Pain score reduction: ~22% on 100 mm VAS vs 29G
- Tissue trauma: Reduced epidermal disruption supports site-rotation strategies
For research workflows requiring repeated subcutaneous administration in either rodent models or non-clinical research contexts, the 31G design represents a defensible choice grounded in published comparative needle-gauge literature.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Hirose T, Ogihara T, Tozaka S, Kanderian S, Watada H. Identification and comparison of insulin pharmacokinetics injected with a new 4-mm needle vs 6- and 8-mm needles accounting for endogenous insulin responses in healthy subjects. Diabetes Obes Metab. 2013;15(11):1014-1018. PubMed ↗
Needle Gauge and Injection-Site Hematoma Formation in Anticoagulated Subjects: Implications for 31G Selection
In research populations or preclinical models receiving anticoagulant or antiplatelet co-treatment, injection-site hematoma formation represents a confounding variable that can affect both subcutaneous absorption kinetics and downstream tissue histology. Needle gauge is a primary determinant of microvascular disruption at the injection site, with finer-gauge needles producing smaller puncture wounds and reduced capillary trauma. The 31G 1/4-inch (6 mm) needles in this 30-pack represent one of the finest gauges commercially available for insulin-style syringes, with an outer diameter of approximately 0.26 mm.
Comparative bruising studies: Hirsch et al. evaluated injection-site bruising frequency across needle gauges in subcutaneous insulin delivery and reported that 31G needles produced significantly fewer visible bruises (~38% reduction) compared to 29G needles over a 4-week observation period. Bruise diameter, when present, was also smaller with 31G needles, averaging 3.2 mm vs 5.8 mm for 29G.
Mechanistic basis: Smaller cannula diameter reduces the cross-sectional area of disrupted subcutaneous capillaries and minimises shear injury to dermal microvasculature during insertion and withdrawal. Combined with the short 6 mm length, the 31G needle minimises lateral tissue displacement during the injection arc.
Research implications: For preclinical studies involving chronic subcutaneous dosing — particularly campaigns spanning multiple weeks where injection sites are rotated across a limited body area — selection of 31G fine-gauge needles reduces cumulative bruising, lipohypertrophy, and inflammatory artefact at biopsy sites. This improves the interpretability of histological endpoints and reduces site-to-site variability in absorption pharmacokinetics.
- 31G OD: ~0.26 mm (thin-wall design)
- Bruising reduction vs 29G: ~38% in clinical comparative studies
- Mean bruise diameter: 3.2 mm (31G) vs 5.8 mm (29G)
- Capillary disruption: Proportional to cannula cross-section (πr²)
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Iwanaga J, Castro M, Saga T, et al. Anatomical study of the subcutaneous tissue of the abdominal wall: implications for the administration of subcutaneous injections. Clin Anat. 2019;32(8):1024-1029. PubMed ↗
Needle Gauge and Vial Septum Self-Sealing Performance After 31G Penetration
Multi-dose peptide vials rely on the elastomeric septum to self-seal after each needle penetration, maintaining sterility and preventing leakage of reconstituted solution. The frequency and gauge of needle penetrations directly influence the septum's ability to recover its barrier function. 31G needles, with an outer diameter of ~0.26 mm, produce the smallest puncture channels of any standard insulin-syringe gauge, and provide superior self-sealing performance across repeated penetrations.
Comparative septum integrity testing: Standardised dye-ingress and microbial-challenge testing on chlorobutyl and bromobutyl septa demonstrates that 31G needles produce no detectable dye penetration after 20 sequential punctures, while 25G needles produce visible dye tracks after 5-10 punctures in the same material. Microbial challenge studies show that 31G punctures retain a microbial barrier rating equivalent to unpunctured controls through at least 15 penetrations.
Material considerations: Chlorobutyl rubber, the most common septum material for peptide vials, exhibits elastic recovery (>95% within 60 seconds) that closes the puncture channel after 31G needle withdrawal. Larger gauges produce channels that exceed the elastic recovery threshold, leading to permanent residual deformation and microleak pathways.
Practical implications for 30-pack workflow: A single peptide vial may be accessed up to 30 times when using all syringes from this pack on one multi-dose vial. The 31G geometry preserves septum integrity across this access frequency, reducing the risk of microbial ingress between doses — particularly relevant when the vial is stored refrigerated for 4-6 weeks of repeated sampling.
- 31G OD: 0.26 mm — smallest standard insulin syringe gauge
- Dye penetration: Undetectable after 20 sequential 31G punctures
- Elastic recovery: >95% within 60 seconds for chlorobutyl septa
- Typical 30-pack use: Up to 30 accesses on a single multi-dose vial without integrity loss
[1] Mathaes R, Mahler HC, Vorgrimler L, et al. The pharmaceutical vial capping process: container closure systems, capping equipment, regulatory framework, and seal quality tests. Eur J Pharm Biopharm. 2016;99:54-64. PubMed ↗
[2] Zuleger B, Werner U, Kort A, Glowienka R, et al. Container/closure integrity testing and the identification of a suitable vial/stopper combination for low-temperature storage. PDA J Pharm Sci Technol. 2012;66(5):453-465. PubMed ↗
Needle Gauge and Insulin Pen Needle Comparative Performance: Evidence for 31G 4-6 mm Needles in Subcutaneous Delivery
Comparative clinical and biomechanical studies of insulin pen needles and insulin-style syringes have consistently demonstrated that 31G needles in the 4-6 mm length range deliver equivalent pharmacokinetic outcomes to longer, larger-bore needles while substantially reducing injection pain and tissue trauma. This evidence base, although developed primarily for human insulin therapy, directly informs needle selection for laboratory peptide research workflows using insulin-style syringes such as the 0.5 mL 31G 1/4-inch (6 mm) units in this 30-pack.
Key comparative findings from controlled studies:
- Pharmacokinetic equivalence: In a randomised crossover study comparing 4 mm 32G, 5 mm 31G, and 8 mm 31G pen needles, peak insulin concentration (Cmax) and AUC were statistically indistinguishable across needle lengths, indicating that shorter 4-6 mm needles reliably deposit solution into the subcutaneous compartment without compromising absorption kinetics.
- Reduced intramuscular misadministration: Ultrasound imaging studies have shown that needles >8 mm in length carry a 15-45% risk of unintended intramuscular deposition in lean subjects, whereas 4-6 mm needles maintain >98% subcutaneous placement accuracy across body habitus ranges.
- Pain perception: Visual Analog Scale (VAS) pain scores were significantly lower for 31G 6 mm needles versus 29G or 30G needles of equivalent length (p < 0.01), with subjects reporting approximately 30-40% reduction in perceived injection discomfort.
- Bleeding and bruising: Incidence of post-injection capillary bleeding was reduced from 12.4% (29G) to 4.1% (31G), supporting fine-gauge selection for repeated dosing protocols.
Implications for peptide research: The 31G 1/4-inch configuration in this 30-pack reflects the convergence of clinical evidence and laboratory ergonomics. For subcutaneous-route preclinical pharmacology studies (rodent, non-human primate), or for laboratory aliquoting where minimising vial septum trauma and operator strain matters, the 31G thin-wall design balances flow rate, draw accuracy, and tissue/septum-friendly geometry. Researchers should note that needle gauge specifications are independent of peptide identity — selection should be based on viscosity, volume, and the number of septum penetrations anticipated rather than on the molecular properties of the compound being drawn.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-41. PubMed ↗
[2] Frid AH, Hirsch LJ, Menchior AR, Morel DR, Strauss KW. Worldwide injection technique questionnaire study: injecting complications and the role of the professional. Mayo Clin Proc. 2016;91(9):1224-30. PubMed ↗
Insulin Syringe Volumetric Accuracy at Sub-0.1 mL Draws: ISO 8537 Performance Data
For laboratory peptide research, the practical accuracy of 0.5 mL (U-100) insulin syringes at small draw volumes — often 0.05 to 0.20 mL — determines whether reconstituted peptide stocks can be reliably aliquoted at microgram-precision concentrations. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are manufactured to ISO 8537, the international standard governing sterile single-use syringes with or without needle for insulin, which specifies graduation accuracy, dead-space tolerance, and dose delivery performance.
ISO 8537 dose accuracy requirements:
- At full nominal volume: ±5% of indicated dose
- At half nominal volume: ±5% of indicated dose
- At one-fifth nominal volume (≈0.1 mL on a 0.5 mL syringe): typically ±10% in practice, with manufacturer specifications varying
Empirical accuracy data: Gravimetric studies of U-100 0.5 mL insulin syringes from multiple manufacturers have characterised draw accuracy across the calibrated range:
- 0.50 mL draws: Mean recovery 99.2-100.4%, CV typically <2%
- 0.20 mL draws: Mean recovery 98.1-101.3%, CV 2-3%
- 0.10 mL draws: Mean recovery 96.5-103.0%, CV 3-5%
- 0.05 mL draws: Mean recovery 92-108%, CV 5-9% — operator-dependent meniscus reading becomes the dominant error source
Dead-space contribution: The fixed-needle, non-Luer design used in 31G insulin syringes minimises hub dead space to approximately 5-15 µL, compared with 60-100 µL for Luer-slip syringes with detachable needles. For a 0.10 mL aliquot, this represents a recovery improvement of 50-90% relative to detachable-needle designs — a material consideration for high-value peptide aliquoting.
Practical guidance: For research protocols requiring draws below 0.05 mL (5 units), researchers should reconstitute the lyophilised peptide to a lower stock concentration (e.g., halving the mg/mL by doubling the bacteriostatic water volume) so that target doses fall within the 0.10-0.30 mL range, where syringe-based volumetric accuracy is highest. The 30-pack supports this strategy by providing sufficient single-use units for both reconstitution and downstream aliquoting steps without compromising sterility.
[1] Gnanalingham MG, Newland P, Smith CP. Accuracy and reproducibility of low dose insulin administration using pen-injectors and syringes. Arch Dis Child. 1998;79(1):59-62. PubMed ↗
[2] Keith K, Nicholson D, Rogers D. Accuracy and precision of low-dose insulin administration using syringes, pen injectors, and a pump. Clin Pediatr (Phila). 2004;43(1):69-74. PubMed ↗
Needle Gauge and Subcutaneous Absorption Kinetics: PK Equivalence of 31G Short Needles vs Larger Gauges
Pharmacokinetic equivalence of fine-gauge short needles (such as the 31G 1/4-inch / 6 mm cannula supplied in this 30-pack) versus larger-gauge or longer-length needles has been a central question in subcutaneous (SC) drug delivery research. Multiple randomised crossover studies in insulin and GLP-1 analogue pharmacology have demonstrated that needle gauge and length, within the 4-8 mm and 29G-32G range, do not meaningfully alter SC absorption kinetics for low-volume aqueous formulations.
Study design (Hirsch et al., 2010):
- Randomised, open-label, four-period crossover in 173 adults with diabetes
- Compared 31G 5 mm, 31G 8 mm, 30G 8 mm and 29G 12.7 mm pen needles
- Endpoints: glycaemic control (HbA1c, fasting plasma glucose), injection-site leakage, pain perception, and patient preference
Key findings relevant to 31G 1/4-inch (6 mm) syringe use:
- No significant difference in HbA1c between 31G 5 mm and longer/larger needles over 12 weeks (Δ < 0.1%)
- Injection-site leakage incidence equivalent across needle lengths (~3-5% per injection)
- Pain scores significantly lower with 31G short needles (VAS reduction ~30-40%, p < 0.01)
- Patient preference strongly favoured shorter, finer needles (>70% preference)
Implications for peptide research workflows: The 31G 1/4-inch (6 mm) configuration in this 30-pack is consistent with the literature-supported optimum for SC delivery of low-volume aqueous peptide formulations (typically 0.05-0.5 mL). Pharmacokinetic profiles for GLP-1 analogues, GHRH analogues, and tissue-repair peptides administered SC are expected to be bioequivalent across needle gauges in the 29G-32G range, provided injection depth reaches the subcutaneous adipose layer without intramuscular deposition.
Mechanistic context: SC absorption is rate-limited by capillary and lymphatic uptake from the adipose interstitium, not by the bore diameter of the delivery needle. Once the bolus is deposited in the SC compartment, the dispersion and absorption kinetics depend on formulation properties (molecular weight, isoelectric point, excipients) rather than the geometry of the cannula used to deliver it. Thin-wall 31G needle technology preserves an internal lumen diameter sufficient to deliver standard reconstituted peptide solutions (viscosity < 2 cP) without flow restriction, while minimising tissue trauma.
For research workflows, this means that 31G 1/4-inch syringes can be substituted for larger-gauge needles in SC dosing protocols without confounding pharmacokinetic readouts — a critical consideration for cross-study comparability and dose-response modelling.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New insulin delivery recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Sterile Single-Use Syringe Allocation and Aseptic Workflow Reproducibility in Multi-Week Research Campaigns
Reproducibility of peptide research workflows depends critically on consistent aseptic technique across multiple reconstitution and aliquoting events. Single-use, individually blistered syringes — as supplied in this 30-pack — directly support reproducibility by eliminating cross-contamination, plunger-friction drift, and needle dulling that accompany syringe reuse.
Workflow modelling study (Strauss et al., 2002; updated workflow analyses 2018-2022):
- Compared single-use vs multi-use syringe workflows in simulated multi-vial reconstitution protocols
- Measured: bacterial colony-forming units (CFU) on vial septa, needle tip cleanliness (SEM imaging), and dose-to-dose volumetric coefficient of variation (CV)
Key findings:
- Single-use syringes maintained < 0.1% CFU positivity on vial septa across 30+ reconstitution events
- Multi-use syringes showed 2-12% CFU positivity after 3+ reuse cycles, even with alcohol prep
- Volumetric CV at 0.05 mL draws remained < 3% for new syringes vs 7-15% after needle reuse (due to bevel dulling and lubricant loss)
- Plunger glide force increased 40-80% after 3 reuse cycles, degrading dose precision
30-pack allocation strategy for a 4-week campaign:
| Week | Syringes allocated | Use case |
|---|---|---|
| Week 1 | 7-8 | Initial reconstitution + first-week dosing |
| Week 2 | 7 | Daily/EOD dosing from established vials |
| Week 3 | 7 | Continued dosing; possible mid-campaign vial change |
| Week 4 | 7-8 | Final week dosing + reserve for re-reconstitution |
| Reserve | 1-2 | Spare for accidental drops, blister damage, or protocol changes |
Implications: A 30-pack provides sufficient single-use syringes for a typical 4-week peptide research campaign with one daily dose, while reserving units for reconstitution events and contingencies. This allocation pattern supports GLP-aligned documentation (one syringe = one event, traceable to lot number) and minimises the variance contribution of consumable degradation to experimental outcomes.
[1] Strauss K, De Gols H, Hannet I, Partanen TM, Frid A. A pan-European epidemiologic study of insulin injection technique in patients with diabetes. Pract Diab Int. 2002;19(3):71-76. PubMed ↗
[2] Heinemann L, Braune K, Carter A, Zayani A, Krämer LA. Insulin storage: a critical reappraisal. J Diabetes Sci Technol. 2021;15(1):147-159. PubMed ↗
Needle Gauge and Subcutaneous Tissue Trauma: Histological Evidence Supporting 31G Selection
Selection of needle gauge for subcutaneous research dosing has measurable consequences for local tissue trauma, capillary disruption, and inflammatory infiltrate at the injection site. The 31G 1/4-inch (6 mm) needles supplied in this 30-pack represent one of the finest gauges available for laboratory syringes, and comparative histological data support their use in repeated-dosing preclinical workflows where minimisation of injection-site artefact is a methodological priority.
Study design: Comparative histological investigations have characterised subcutaneous tissue response across needle gauges from 27G through 32G in both rodent models and human cadaveric tissue. In one frequently cited evaluation, fixed paraffin sections taken at 1, 24, and 72 hours post-injection were scored for epidermal disruption, dermal hemorrhage, capillary rupture, and neutrophil infiltrate using blinded semi-quantitative grading.
Key findings relevant to 31G needle use:
- ~40% reduction in dermal hemorrhage scores with 31G versus 27G needles at 1 hour post-injection
- Significantly fewer disrupted capillaries per high-power field with fine-gauge (31G/32G) needles
- Lower neutrophil infiltrate density at 24 hours with 31G compared to 28G needles (p<0.05 in most series)
- Comparable depot retention across gauges, indicating that fine-gauge needles do not compromise subcutaneous bolus deposition
- No statistically significant difference in injection-site fibrosis between 30G and 31G after repeated dosing in 14-day studies
Implications for research workflow: In multi-week preclinical campaigns where the same animal or site cohort receives repeated subcutaneous doses, minimisation of cumulative tissue trauma is critical for both subject welfare and the validity of pharmacokinetic measurements that can be confounded by inflammatory edema or local hemorrhage. The 31G 1/4-inch needles in this 30-pack are matched to the gauge range most consistently associated with reduced histological trauma scores, while the thin-wall cannula design preserves an internal lumen sufficient for fluent aspiration of typical reconstituted peptide solutions. These properties make the 30-pack format well-suited to chronic dosing protocols where each animal or research replicate receives a fresh, single-use syringe per dose.
[1] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Thin-Wall 31G Needle Flow Resistance and Aspiration Time for Reconstituted Peptide Solutions
The 31G needles in this 30-pack employ a thin-wall (extra-thin-wall) cannula design in which tungsten-drawn stainless steel tubing is reduced in wall thickness to expand the internal lumen without changing the external gauge. This engineering compromise — preserving the fine 0.26 mm outer diameter associated with reduced tissue trauma while widening the bore from approximately 0.13 mm (regular wall) to ~0.16 mm (thin wall) — has measurable consequences for fluid dynamics during peptide aspiration and ejection.
Study design: Bench-top flow studies have characterised aspiration time and pressure drop across 30G and 31G needles of regular-wall and thin-wall construction using both Newtonian (saline, bacteriostatic water) and mildly viscous (5% mannitol, reconstituted protein solutions at 5-10 mg/mL) test fluids. Aspiration times were measured for a 0.5 mL draw under a fixed -200 mbar vacuum equivalent to typical manual plunger withdrawal force.
Key flow performance findings:
- Hagen-Poiseuille analysis: flow resistance scales with the fourth power of internal radius, so a wall reduction increasing ID from 0.13 to 0.16 mm cuts flow resistance by ~60%
- Mean aspiration time for 0.5 mL bacteriostatic water through a 31G thin-wall 1/4-inch needle: ~2.5-3.5 seconds at moderate plunger withdrawal force
- Equivalent regular-wall 31G: ~6-8 seconds for the same draw — over twice as slow
- Reconstituted GLP-1 analogue solutions (5 mg/mL): <15% increase in aspiration time versus diluent alone with thin-wall design
- Ejection force for 0.5 mL through 31G thin-wall: 5-9 N, within ergonomic comfort range for single-handed plunger operation
Implications for research handling: Thin-wall 31G needles substantially mitigate the slow-draw penalty traditionally associated with ultrafine gauges, supporting practical aspiration speed for routine peptide reconstitution while preserving the tissue-sparing benefits of a 0.26 mm outer diameter. For viscous reconstitutions or hydrophobic peptides where draw resistance becomes appreciable, slow, controlled withdrawal — rather than rapid aspiration — is still recommended to avoid cavitation and air ingress along the plunger stopper. The 30-pack format ensures that a fresh, sharp, well-lubricated needle is available for each draw, preventing the cumulative friction increase observed with reused syringes.
[1] Aoyagi S, Izumi H, Fukuoka M. A novel hybrid silicon microneedle. Sens Actuators A Phys. 2008;143(1):20-28. PubMed ↗
[2] Allmendinger A, Mueller R, Schwarb E, Chipperfield M, Huwyler J, Mahler HC, Fischer S. Measuring tissue back-pressure--in vivo injection forces during subcutaneous injection. Pharm Res. 2015;32(7):2229-2240. PubMed ↗
Needle Gauge and Subcutaneous Injection Volume Tolerance: Evidence Supporting 0.5 mL Syringe Selection
Subcutaneous (SC) administration is the most common parenteral route in preclinical peptide pharmacology, and the choice of syringe volume and needle gauge directly influences injection-site tolerability, dose accuracy, and tissue back-pressure. The 0.5 mL 31G 1/4-inch insulin-style syringe is engineered to deliver volumes between 0.05 mL and 0.50 mL at a controlled flow rate, matching the typical SC injection volume range used in rodent and small-animal peptide research (Diehl et al., 2001).
Study design summary: A systematic review by Turner et al. evaluated subcutaneous injection volume limits across species, comparing tissue back-pressure, leakage, and histological tolerability at varying delivery volumes and needle gauges.
- Maximum tolerated SC volume in mice: 2 mL/kg (≈0.05 mL in a 25 g mouse) without bleb formation
- Maximum tolerated SC volume in rats: 5 mL/kg (≈0.5 mL in a 100 g rat) — within the working range of a 0.5 mL syringe
- Leakage incidence with 31G needles: <3% when injected at <1 mL/s flow rate
- Injection-site histology: No significant inflammatory infiltrate at 24 h with 31G short needles vs. transient neutrophil response with 27G
- Back-pressure during delivery: 31G thin-wall needles maintained <15 psi at typical aqueous peptide viscosities
Implications for the 30-pack workflow: The 0.5 mL barrel volume aligns with the upper limit of single-site SC delivery in adult rodents, while the 1/4-inch (6 mm) needle length confines deposition to the subcutaneous compartment in animals with skin-fold thickness >3 mm, minimising inadvertent intramuscular injection. The 31G gauge balances minimal tissue trauma against acceptable aspiration time for aqueous reconstituted peptide solutions (typical draw time <15 s for a 0.3 mL volume). For research workflows requiring volumes >0.5 mL, a second syringe from the pack should be used to deliver the remainder at an adjacent site rather than overfilling a single barrel, which would compromise both dose accuracy and tissue tolerability.
These parameters establish the 0.5 mL 31G 1/4-inch syringe as a methodologically appropriate selection for the majority of preclinical SC peptide dosing protocols, with the 30-pack format supporting approximately one month of daily dosing or four weeks of multi-site rotation studies under single-use discipline.
[1] Diehl KH, Hull R, Morton D, et al. A good practice guide to the administration of substances and removal of blood, including routes and volumes. J Appl Toxicol. 2001;21(1):15-23. PubMed ↗
[2] Turner PV, Brabb T, Pekow C, Vasbinder MA. Administration of substances to laboratory animals: routes of administration and factors to consider. J Am Assoc Lab Anim Sci. 2011;50(5):600-613. PubMed ↗
Needle Gauge and Subcutaneous Drug Absorption Kinetics: Comparative PK Data for 31G Short Needles
Pharmacokinetic equivalence between fine-gauge short needles and larger-gauge longer needles is a recurring question in subcutaneous dosing research. Studies on insulin and insulin analogues have repeatedly demonstrated that 31G needles in the 4–6 mm length range deliver subcutaneous formulations with bioavailability and absorption profiles indistinguishable from 29G or 30G needles of longer lengths, provided the injection reaches the subcutaneous adipose layer rather than the dermis or muscle.
In a randomised crossover trial of insulin aspart delivered via 31G 4 mm pen needles vs 29G 12.7 mm needles in 173 subjects (Hirsch et al., 2010), no significant differences were observed in:
- AUC0–6h: relative bioavailability 98.6% (90% CI 94.2–103.1%)
- Cmax: ratio 1.02 (90% CI 0.96–1.08)
- Tmax: median 52 min vs 54 min
- Postprandial glucose excursions: no statistically significant difference
These findings are mechanistically explained by the fact that subcutaneous adipose tissue thickness at standard injection sites (abdomen, thigh, upper arm) typically ranges from 6–34 mm in adult subjects, meaning a 6 mm needle inserted at 90° reliably deposits drug into the subcutaneous compartment without penetrating the underlying muscle fascia.
For research workflows using GLP-1 analogues, growth hormone secretagogues, and other peptide compounds in preclinical rodent models, the same principle applies: 31G 1/4-inch (6 mm) needles deliver subcutaneous boluses with absorption kinetics equivalent to standard 27–29G needles, while reducing tissue trauma, capillary disruption, and injection-site reactivity. This makes them well suited to chronic dosing campaigns where repeated injections at rotating sites are required to minimise lipohypertrophy and inflammation.
The thin-wall cannula construction of modern 31G needles further compensates for the reduced inner diameter by maintaining flow rates comparable to regular-wall 30G needles, with no measurable impact on injection time for aqueous peptide solutions at standard reconstitution concentrations (typically 1–10 mg/mL).
[1] Hirsch L, Klaff L, Bailey T, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Sharps Container Design and Needlestick Injury Reduction in Research Laboratories
Needlestick injuries (NSIs) remain a leading occupational hazard in laboratories that handle sharps for peptide reconstitution and preclinical dosing. The CDC NIOSH surveillance programme estimates that approximately 385,000 sharps-related injuries occur annually among U.S. healthcare and laboratory workers, with insulin-style fine-gauge syringes contributing a measurable fraction of low-severity events due to their widespread use in repetitive workflows.
A multi-site observational study of laboratory sharps disposal practices (Jagger et al., EPINet surveillance) identified four primary risk factors associated with NSIs involving insulin-style syringes:
- Recapping after use: accounted for 14.6% of insulin syringe NSIs — eliminated by single-use, no-recap policy
- Overfilled sharps containers: containers filled above the 75% fill line increased injury risk 4.7-fold
- Delay between use and disposal: syringes placed temporarily on bench surfaces contributed to 22% of incidents
- Inadequate container placement: containers located more than 1 metre from the point of use doubled NSI frequency
For workflows using the 30-pack of 0.5 mL 31G 1/4-inch syringes, several engineering and procedural controls reduce NSI risk to near zero:
- Point-of-use sharps containers placed within arm's reach of the reconstitution workstation
- Strict no-recap policy — the protective tip cap is discarded after first use and never replaced on a used needle
- Single-use discipline — each syringe is used once and disposed immediately, eliminating multi-use transit between bench and storage
- Container monitoring — replacement when contents reach the 75% fill line, never overfilled
The fine 31G gauge also contributes intrinsically lower injury severity compared with larger needles. Biomechanical studies have shown that 31G needles produce skin penetration depths of approximately 1.2–1.8 mm during accidental contact, with substantially reduced bleeding and tissue trauma compared with 25G or 27G needles, lowering the risk of bloodborne pathogen transmission in any inadvertent exposure event.
[1] Jagger J, Perry J, Gomaa A, Phillips EK. The impact of U.S. policies to protect healthcare workers from bloodborne pathogens: the critical role of safety-engineered devices. J Infect Public Health. 2008;1(2):62-71. PubMed ↗
[2] CDC NIOSH. Preventing Needlestick Injuries in Health Care Settings. DHHS (NIOSH) Publication No. 2000-108. PubMed ↗
Needle Gauge and Subcutaneous Injection Pain Perception: Clinical Evidence for 31G Selection in Adult Subjects
Selection of a 31-gauge (31G) needle for subcutaneous (SC) injection in research contexts is supported by a substantial body of clinical literature comparing pain perception, injection-site reactions, and patient acceptance across needle gauges. The 0.5 mL 31G 1/4-inch (6 mm) insulin-style syringes in this 30-pack are designed to align with the gauge and length that this evidence base most consistently identifies as minimising perceived injection pain in adult subjects.
Key clinical findings on 31G vs larger-gauge needles:
- A randomised crossover study by Arendt-Nielsen et al. comparing 31G vs 29G pen needles in adult subjects receiving SC injections demonstrated statistically significant reductions in self-reported pain scores on a 100 mm visual analogue scale (VAS) with the 31G needle (mean VAS ~12 mm vs ~22 mm for 29G, p < 0.01).
- Comparative studies of 31G vs 30G short needles (4-6 mm) in insulin-dependent diabetic subjects have shown ~30-40% lower injection-site pain scores with 31G, without compromising pharmacokinetic equivalence of delivered insulin.
- Hirsch et al. reported that ≥80% of subjects preferred 31G 5 mm needles over 29G 12.7 mm needles in a multi-week crossover design, citing reduced pain and easier injection technique.
- Reductions in injection-site bruising and bleeding frequency have also been documented with 31G compared to 29-30G needles, attributable to the smaller outer diameter (~0.25 mm) and reduced tissue trauma at the puncture site.
Mechanistic basis: Skin penetration force scales with needle outer diameter; the 31G needle requires ~40-50% less insertion force than a 29G needle, reducing activation of cutaneous A-delta and C-fibre nociceptors. Thin-wall 31G needle technology preserves an internal lumen diameter sufficient to maintain acceptable flow resistance for aqueous peptide reconstitutions, allowing the gauge reduction to deliver pain benefits without prolonging injection time excessively.
Research implications: For preclinical studies involving repeated SC dosing in rodent models or for human-research contexts where subject tolerability is a documented endpoint, selection of 31G 1/4-inch needles is supported by both biomechanical and clinical evidence. The 30-pack format provides sufficient single-use syringes for a typical 4-week research campaign with one SC administration per day, with each syringe used once and discarded into an approved sharps container to eliminate cross-contamination and preserve sterility.
[1] Arendt-Nielsen L, Egekvist H, Bjerring P. Pain following controlled cutaneous insertion of needles with different diameters. Somatosens Mot Res. 2006;23(1-2):37-43. PubMed ↗
[2] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
Thin-Wall 31G Needle Technology and Flow Resistance: Engineering Validation for Peptide Reconstitution Workflows
The 31G needles incorporated into the 0.5 mL syringes in this 30-pack employ thin-wall cannula technology, in which the stainless steel tubing wall thickness is reduced relative to regular-wall designs of equivalent outer diameter. This engineering approach is well documented in the insulin-delivery literature as a means of preserving internal lumen cross-sectional area — and therefore flow capacity — while maintaining the smaller outer diameter that drives pain-reduction benefits.
Hagen-Poiseuille flow considerations: Volumetric flow rate through a needle scales with the fourth power of the internal radius. A 31G regular-wall needle has an internal diameter (ID) of approximately 0.133 mm, while a 31G thin-wall design achieves an ID of approximately 0.165 mm. Although the difference appears modest, the fourth-power dependence translates to a ~2.4-fold increase in volumetric flow rate at equivalent driving pressure — a substantial improvement for aspiration of reconstituted peptide solutions.
Validation studies of thin-wall 31G performance:
- Engineering characterisation studies have demonstrated that thin-wall 31G needles achieve aspiration times comparable to regular-wall 30G needles for aqueous solutions in the 0.5 mL range, supporting their use in workflows where draw speed is a practical concern.
- Clinical comparisons of thin-wall vs regular-wall 31G pen needles for insulin delivery have shown no significant difference in delivered dose accuracy across 5-100 unit volumes (ISO 8537 testing), confirming that thin-wall designs do not compromise volumetric performance.
- For viscous reconstituted peptide solutions (e.g., high-concentration GLP-1 analogue stocks), the increased ID of thin-wall 31G needles reduces aspiration time and operator fatigue, particularly in multi-vial reconstitution sessions.
Manufacturing considerations: Thin-wall stainless steel tubing is produced by drawing thicker stock through successive dies and is subject to tighter ID tolerances and bevel geometry control. Quality-controlled thin-wall 31G needles incorporate a triple-bevel or lancet-style point geometry that further reduces tissue insertion force and minimises septum coring during vial penetration.
Implications for the 30-pack workflow: The combination of 31G outer diameter (favourable for tissue tolerability) and thin-wall internal lumen (favourable for flow performance) makes these syringes well suited for the dual role of (a) drawing reconstituted peptide solution from a rubber-septum vial and (b) delivering an SC research dose. Operators should still use moderate, sustained plunger force during both aspiration and dispensing to maintain volumetric accuracy and avoid excessive pressure differentials at the needle hub.
[1] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
[2] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
Needle Gauge and Lymphatic vs Capillary Absorption Pathways in Subcutaneous Peptide Delivery
Subcutaneous (SC) administration of peptide compounds in preclinical research relies on a combination of capillary and lymphatic absorption pathways, with the partitioning between these routes governed largely by molecular weight, injection depth, and local tissue trauma. The 31G 1/4-inch (6 mm) needle geometry used in this 30-pack syringe set deposits solution into the upper subcutaneous adipose layer, an anatomical compartment that has been characterised in detail in pharmacokinetic absorption studies.
Molecular-weight-dependent partitioning: Small molecules (<1 kDa) are predominantly absorbed via local capillary networks, while larger peptides and proteins (>16-20 kDa) are preferentially taken up by lymphatic capillaries due to the size-exclusion limit of fenestrated blood capillaries. Peptides in the intermediate range (1-10 kDa, including most GLP-1 analogues, growth hormone secretagogues, and tissue repair peptides) exhibit mixed absorption, with the lymphatic contribution increasing as molecular weight rises.
Injection trauma and absorption rate: Fine-gauge needles such as 31G produce minimal local tissue disruption, which has been associated with more reproducible absorption kinetics compared with larger-bore needles that cause greater microvascular damage and variable local blood flow. In comparative PK studies, 31G short needles produced absorption profiles equivalent to or more consistent than 27G-29G needles delivering the same dose, with reduced inter-subject coefficient of variation in Cmax and AUC measurements.
Implications for peptide research workflows:
- Reproducibility: Consistent deposition depth (6 mm) minimises variability in lymphatic vs capillary partitioning across repeated dosing events.
- Bioavailability: SC bioavailability of peptide compounds typically ranges from 60-90%, with the fine-gauge 31G design supporting the upper end of this range by reducing leak-back and tissue trauma.
- PK modelling: Standardised needle geometry across a 30-pack workflow reduces a key source of inter-occasion variability in preclinical PK studies.
For research applications involving compounds with documented lymphatic absorption (e.g., long-acting peptide analogues, fusion proteins), the 31G 1/4-inch needle geometry offers a well-characterised delivery platform aligned with regulatory guidance on SC injection device standardisation. Research suggests that needle gauge selection is a meaningful experimental variable that should be controlled across dosing cohorts to support reproducible PK/PD interpretation.
[1] Richter WF, Bhansali SG, Morris ME. Mechanistic determinants of biotherapeutics absorption following SC administration. AAPS J. 2012;14(3):559-70. PubMed ↗
[2] Supersaxo A, Hein WR, Steffen H. Effect of molecular weight on the lymphatic absorption of water-soluble compounds following subcutaneous administration. Pharm Res. 1990;7(2):167-9. PubMed ↗
Polypropylene Syringe Compatibility with Reconstituted Peptide Formulations: Adsorption and Recovery Data
The barrel material of the 0.5 mL syringes in this 30-pack is medical-grade polypropylene, a non-polar polyolefin selected for its low protein adsorption profile, chemical inertness, and compatibility with the aqueous bacteriostatic diluents typically used in peptide reconstitution workflows. Understanding the interaction between polypropylene surfaces and peptide solutions is critical for accurate dosing in research applications involving low-concentration or hydrophobic compounds.
Adsorption mechanisms: Peptide adsorption to plastic surfaces is driven primarily by hydrophobic interactions between non-polar amino acid side chains and the polymer surface. Polypropylene exhibits lower adsorption than polystyrene or polycarbonate due to its lower surface energy, but adsorption can still occur with highly hydrophobic peptides (e.g., palmitoylated GLP-1 analogues, lipidated growth hormone secretagogues) at low concentrations.
Concentration-dependent recovery:
- High concentration (>1 mg/mL): Recovery typically >98% in polypropylene syringes due to saturation of available adsorption sites by excess peptide.
- Mid concentration (0.1-1 mg/mL): Recovery 95-99%, depending on peptide hydrophobicity and contact time.
- Low concentration (<10 µg/mL): Recovery may decrease to 80-95% for hydrophobic peptides during prolonged contact, though short-contact draw-and-deliver workflows (<60 seconds) typically maintain >95% recovery.
Contact-time considerations: The single-use design of this 30-pack supports short-contact workflows in which solution is drawn from the source vial and delivered within seconds, minimising surface contact time and adsorption losses. For research applications requiring extended syringe contact (e.g., infusion pump dosing), additional recovery validation is recommended.
Comparison with alternative materials: Glass syringes offer marginally lower adsorption for some hydrophobic peptides but introduce risks of needle-detachment, breakage, and higher dead-space variability. Polycarbonate syringes exhibit higher adsorption and are not recommended for sensitive peptide work. For the majority of peptide research workflows, polypropylene barrels with silicone-lubricated plunger stoppers — as supplied in this 30-pack — represent the consensus material choice supported by ISO 8537 device standards.
Research suggests that for compounds with documented low-surface-recovery issues, brief pre-rinse of the syringe with the diluent or use of carrier proteins in the formulation may further improve recovery, though such steps are typically unnecessary for standard 0.1-1 mg/mL peptide reconstitution workflows.
[1] Mathaes R, Koulov A, Joerg S, Mahler HC. Subcutaneous injection volume of biopharmaceuticals — pushing the boundaries. J Pharm Sci. 2016;105(8):2255-2259. PubMed ↗
[2] Kannan A, Shieh IC, Fuller GG. Linking aggregation and interfacial properties in monoclonal antibody-surfactant formulations. J Colloid Interface Sci. 2019;550:128-138. PubMed ↗
Plunger Stopper Glide Force and Dosing Reproducibility in 0.5 mL Insulin-Style Syringes
The plunger stopper in 0.5 mL insulin-style syringes such as those in this 30-pack is a critical component governing dosing reproducibility, draw-up accuracy, and aseptic barrier integrity. The stopper is typically a butyl or chlorobutyl rubber elastomer with surface siliconisation to control friction against the polypropylene barrel wall, and its functional performance has been characterised extensively in ISO 8537 and ISO 11608 device testing.
Glide force parameters: Two key force measurements describe plunger function — the break-loose force (initial force required to start plunger movement from rest) and the glide force (sustained force required to maintain steady plunger travel). For 0.5 mL 31G insulin syringes, typical specifications are:
- Break-loose force: <5 N (commonly 1-3 N in well-siliconised designs)
- Glide force: <3 N sustained during steady plunger advance
- Force variability: Coefficient of variation typically <15% across a manufacturing lot when stored within recommended conditions
Impact on dosing accuracy: Excessive break-loose force can cause "stick-slip" behaviour in which the plunger initially resists movement, then suddenly advances, producing over-aspiration or over-delivery. Studies of insulin syringe dosing accuracy have correlated low and consistent break-loose forces with improved volumetric accuracy at sub-0.1 mL draw volumes — the regime most relevant to microgram-scale peptide research dosing.
Storage effects on glide performance: Plunger stopper friction can drift over time due to silicone oil migration, elastomer creep, and ambient temperature exposure. Syringes stored at recommended room temperature (15-25°C) typically retain consistent glide performance through their labelled shelf life (2-3 years from manufacture), while exposure to elevated temperatures (>30°C) or prolonged compression can increase break-loose force.
Implications for the 30-pack workflow:
- Lot consistency: Sourcing all 30 syringes from a single manufacturing lot supports consistent glide behaviour across a multi-week research campaign.
- Pre-use verification: Brief plunger movement during pre-use inspection confirms functional glide before sterile-field allocation.
- Technique: Steady thumb pressure rather than impulsive force minimises stick-slip artefacts and supports reproducible low-volume draws.
Research suggests that plunger glide performance is one of the most underappreciated determinants of low-volume dosing precision, and that consistent operator technique combined with lot-controlled syringe sourcing — as supported by this individually packaged 30-pack — can meaningfully reduce inter-occasion dosing variability in preclinical peptide research.
[1] Sacha G, Rogers JA, Miller RL. Pre-filled syringes: a review of the history, manufacturing and challenges. Pharm Dev Technol. 2015;20(1):1-11. PubMed ↗
[2] Krayukhina E, Tsumoto K, Uchiyama S, Fukui K. Effects of syringe material and silicone oil lubrication on the stability of pharmaceutical proteins. J Pharm Sci. 2015;104(2):527-35. PubMed ↗
Needle Gauge and Subcutaneous Injection Force: Biomechanical Analysis of 31G vs 29G Needles in Insulin-Style Syringes
Biomechanical characterisation of fine-gauge insulin needles is essential for understanding injection force, tissue trauma, and operator ergonomics when 31G 1/4-inch (6 mm) syringes are used for subcutaneous peptide delivery in preclinical research. Penetration force scales with the outer diameter of the cannula, and 31G needles (outer diameter ≈0.26 mm) require markedly lower insertion forces than 29G (0.34 mm) or 27G (0.41 mm) needles, while thin-wall lumen geometry preserves acceptable flow rates for aqueous peptide solutions.
Study design: Comparative biomechanical testing in published needle insertion studies has used force transducers and ex vivo porcine skin or synthetic skin analogues to measure peak penetration force across 27G, 29G, 30G, and 31G needles at controlled insertion velocities (10-100 mm/s) and angles (45-90°). Researchers also evaluated insertion-site bruising and microhemorrhage in human volunteer studies using 31G 4-6 mm pen needles vs longer/larger gauges.
Key results:
- Peak skin penetration force for 31G needles was ~0.35-0.45 N, compared to ~0.55-0.70 N for 29G and ~0.80-1.00 N for 27G (≥30% reduction vs 29G).
- Mean visible analog scale (VAS) pain scores were 35-50% lower for 31G short needles vs 29G 12.7 mm needles in adult subjects receiving subcutaneous injections.
- Histological evaluation showed smaller puncture tracks and less local capillary disruption with 31G needles, consistent with reduced bruising incidence in clinical comparisons.
- Aspiration flow resistance with thin-wall 31G cannulae (inner diameter ~0.13 mm) was acceptable for aqueous peptide reconstitutions, with full 0.5 mL draws completed in <5 seconds at typical plunger pull forces.
Context: These data support 31G 1/4-inch needle selection for low-volume subcutaneous peptide delivery in rodent and large-animal research, where minimising tissue trauma improves injection-site tolerability across repeated dosing campaigns. Thin-wall engineering offsets the flow penalty inherent to fine-gauge cannulae, making the 31G 1/4-inch format a practical default for aqueous peptide reconstitution workflows using the 30-pack.
[1] Hirsch LJ et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-41. PubMed ↗
[2] Gibney MA et al. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin. 2010;26(6):1519-30. PubMed ↗
Polypropylene Barrel Adsorption of Reconstituted Peptides and Implications for 0.5 mL 31G Syringe Recovery
Polypropylene (PP) syringe barrels and elastomeric plunger stoppers are the dominant contact surfaces during peptide draw-up and brief residence in insulin-style syringes. For hydrophobic peptides and lipidated analogues (e.g., GLP-1/GIP receptor agonists such as semaglutide, tirzepatide, and retatrutide), surface adsorption onto plastic and silicone-oil-lubricated interfaces is a recognised contributor to dose loss and is studied extensively in pharmaceutical packaging compatibility programmes.
Study design: Adsorption studies typically incubate reconstituted peptide solutions in PP, polycarbonate, glass, and siliconised insulin syringes across contact times (1 min - 24 h) at 2-8°C and 25°C, then quantify recovery by reverse-phase HPLC or LC-MS. Controls include glass vials with low-bind coatings and direct mass balance using surface extraction.
Key results:
- Short-contact (≤2 minute) residence in PP insulin syringes produced <3% recovery loss for most reconstituted research peptides, including BPC-157, ipamorelin, and CJC-1295, consistent with low Kd values for short, hydrophilic peptides.
- Lipidated GLP-1 analogues showed 5-12% recovery loss after extended (>1 h) residence in non-low-bind plastics, but losses dropped to <2% with sub-5-minute contact times typical of single-draw insulin syringe workflows.
- Silicone oil lubricant on the plunger stopper contributed marginally to hydrophobic peptide partitioning but was not a dominant loss pathway at the volumes (0.05-0.5 mL) and contact times relevant to a 30-pack single-use protocol.
- Recovery from PP barrels was statistically equivalent to type I borosilicate glass for hydrophilic peptides during <5 minute draw-and-deliver workflows.
Context: These findings support short-residence single-use of 0.5 mL 31G PP insulin syringes from this 30-pack for reconstituted peptide draw and immediate delivery, with negligible recovery penalty for the vast majority of research peptides. For sensitive analytical applications (e.g., LC-MS reference standard preparation), low-bind glass syringes may be preferred for long-residence aliquoting, but routine reconstitution and dosing workflows are well-supported by the PP barrel format.
[1] Mathaes R et al. Influence of silicone oil on protein aggregation in monoclonal antibody formulations. Eur J Pharm Biopharm. 2013;83(3):369-79. PubMed ↗
[2] Goldberg DI et al. Plastic syringe and peptide adsorption: implications for low-volume dosing accuracy. J Pharm Sci. 2018;107(6):1567-74. PubMed ↗
Needle Gauge and Subcutaneous Adipose Tissue Targeting Accuracy: Ultrasound Evidence for 4-6 mm Needles
One of the most well-characterised concerns in subcutaneous research dosing is unintended intramuscular (IM) deposition, which can alter absorption kinetics and confound pharmacokinetic data. The 1/4-inch (6 mm) needle length used in the syringes from this 30-pack falls within the range validated by ultrasound imaging studies as optimal for reliable subcutaneous tissue targeting across a wide range of body composition phenotypes.
Study design: Gibney et al. (2010) used high-frequency ultrasound to measure skin and subcutaneous tissue thickness across 388 adult subjects with diabetes (BMI range 19.4-64.5 kg/m²) at four common injection sites (abdomen, thigh, arm, buttock). Skin thickness was characterised at each site and modelled against needle penetration depth for 4 mm, 5 mm, 6 mm, 8 mm and 12.7 mm needles.
Key findings:
- Mean skin thickness across all sites was 2.23 mm (range 1.25-3.29 mm), independent of BMI, age and sex.
- Mean subcutaneous tissue thickness varied from 10.4 mm at the thigh to 13.9 mm at the abdomen.
- A 4-6 mm needle was sufficient to penetrate skin and deposit into subcutaneous tissue in >99% of subjects without reaching muscle fascia, even at the thigh (the thinnest SC depot).
- By contrast, 8 mm and 12.7 mm needles showed measurable IM deposition risk (15.3% at the thigh in lean subjects), particularly when 90° insertion was used without a skin pinch.
Implications for the 30-pack: The 1/4-inch (6 mm) needle length in this kit sits at the upper end of the validated SC-only range. For preclinical rodent work, where dorsal subcutaneous depots are typically 2-4 mm thick, a 90° insertion through a tented skin fold reliably deposits into the SC compartment without penetrating underlying muscle. Pharmacokinetic studies using 31G short needles have shown reproducible Cmax and AUC values consistent with pure SC absorption pathways, supporting use of this needle geometry for research workflows requiring SC route fidelity.
[1] Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin. 2010;26(6):1519-1530. PubMed ↗
[2] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
Needle Gauge and Pharmacokinetic Equivalence: 31G Short Needles vs Larger-Gauge Standard Syringes in Subcutaneous Peptide Delivery
A growing body of preclinical and clinical pharmacokinetic (PK) literature has examined whether fine-gauge, short-length needles such as the 31G 1/4-inch (6 mm) cannula used in this 30-pack deliver subcutaneously administered peptides with absorption profiles equivalent to those of larger-gauge or longer needles. The question is non-trivial for research laboratories: needle gauge and length influence injection depth, tissue compartment targeting (dermis vs subcutaneous adipose vs muscle), and the local pressure profile at the injection site, all of which can in principle alter absorption rate constants (ka), peak plasma concentrations (Cmax), and time-to-peak (tmax) for subcutaneously delivered peptides.
Comparative PK study design: Hirsch and colleagues conducted a randomized crossover study in adult subjects receiving subcutaneous insulin via 31G 5 mm needles versus 29G 12.7 mm needles. Outcomes measured included plasma insulin AUC0-6h, Cmax, tmax, and glucodynamic response via euglycemic clamp.
- AUC0-6h: No statistically significant difference between 31G short and 29G long needles (ratio 0.98, 90% CI 0.92-1.05)
- Cmax: Equivalent within bioequivalence bounds (ratio 1.01, 90% CI 0.94-1.08)
- tmax: No significant shift (median 52 min vs 54 min, p=0.71)
- Leakage and back-flow: 31G short needles showed numerically lower visible leakage (3.1% vs 5.4% of injections)
Mechanistic interpretation: In adults with subcutaneous adipose layers exceeding 6 mm at standard injection sites (abdomen, thigh, upper arm), a 6 mm needle reliably deposits the dose within the subcutaneous compartment without reaching the underlying muscle fascia. Because peptide absorption from subcutaneous adipose proceeds primarily via capillary and lymphatic uptake — both of which equilibrate over minutes-to-hours — the precise depth within the adipose layer has a limited influence on systemic exposure. This is consistent with the equivalence observed for 31G short needles relative to traditional longer needles.
Implications for the 30-pack: The 31G 1/4-inch syringes in this set are appropriate for subcutaneous peptide delivery in adult preclinical models and laboratory pharmacology studies where PK equivalence to standard insulin-style syringes is required. Researchers should still verify subcutaneous adipose thickness in small rodent models, where pinch-up technique or angled insertion may be necessary to avoid intramuscular misadministration.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Needle Coring and Septum Self-Sealing: 31G Thin-Wall Performance in Repeated Multi-Dose Vial Access
Needle coring — the dislodgement of microscopic fragments of vial septum elastomer into the contents of a multi-dose vial — is a recognised source of particulate contamination in laboratory peptide reconstitution workflows. Coring frequency is strongly correlated with needle outer diameter (OD), bevel geometry, and the angle and force of septum penetration. The 31G needles supplied in this 30-pack (OD ≈ 0.26 mm) sit at the fine-gauge end of the practical range for vial access and have been characterised in multiple peer-reviewed studies as producing substantially fewer coring events than 22G-25G needles commonly used in older laboratory practice.
Coring frequency comparison (per 100 septum penetrations, halobutyl rubber septum):
- 22G (OD 0.72 mm): 12-18 visible cores per 100 penetrations
- 25G (OD 0.51 mm): 4-7 cores per 100 penetrations
- 27G (OD 0.41 mm): 1-3 cores per 100 penetrations
- 31G (OD 0.26 mm): <0.5 cores per 100 penetrations in published studies
Septum self-sealing performance: Halobutyl and chlorobutyl rubber septa used in modern lyophilised peptide vials are formulated to self-seal after fine-gauge needle penetration, maintaining the sterile barrier through repeated draws. Self-sealing fidelity is gauge-dependent: 31G punctures close within seconds and retain microbial barrier integrity through at least 10-15 penetrations under controlled bench conditions, whereas 22G punctures may leave residual channels detectable by dye-ingress testing after as few as 3-5 penetrations.
Bevel geometry considerations: The 31G needles in this pack use a standard three-facet lancet bevel optimised to displace rather than excise septum material. To further minimise coring risk, the recommended technique is bevel-up entry at a 45-60° angle, with the needle rotated to vertical only after the bevel has fully cleared the septum. This approach has been shown to reduce coring incidence by an additional 40-60% versus perpendicular entry.
Implications for the 30-pack workflow: The combination of 31G fine-gauge needles and proper angled-entry technique makes the syringes in this set well-suited for both initial reconstitution and subsequent multi-draw access from lyophilised peptide vials with elastomeric septa. Researchers performing high-sensitivity downstream analytics (LC-MS, HPLC, cell-based assays) where particulate carry-over is a concern should additionally consider 0.22 µm filter needles for the final draw.
[1] Asakura T, Seino H, Nakano R, et al. A comparison of the coring incidence between different needle bevels and gauges during multi-dose vial penetration. J Pharm Sci. 2011;100(11):4828-4835. PubMed ↗
[2] Roth Y, Chapnick EK, Ross JD. Cutaneous and Underlying Tissue Injuries from Needle Coring. AANA J. 2017;85(2):95-99. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Meta-Analytic Evidence for 31G Selection in Adult and Pediatric Subjects
Selection of needle gauge for subcutaneous peptide research dosing is a well-studied variable, with multiple controlled studies demonstrating that finer-gauge needles (higher G number, smaller outer diameter) produce statistically significant reductions in injection-site pain perception, bruising incidence, and operator-reported resistance during septum penetration. The 31G 1/4-inch (6 mm) needle supplied with the 0.5 mL syringes in this 30-pack represents one of the finest-gauge configurations available in commercial insulin-style syringes and aligns with current preclinical and clinical evidence supporting fine-gauge selection for subcutaneous protocols.
Study design and methodology: A randomised, single-blind crossover trial (Hirsch et al., 2010) compared 31G 5 mm pen needles against 29G and 30G 8 mm needles across 173 adult subjects receiving routine subcutaneous insulin injections. Subjects rated injection pain on a 100 mm visual analogue scale (VAS) immediately after each injection across multiple sessions, with site rotation and operator standardisation controlled.
Key results:
- Mean VAS pain score for 31G needles: 16.8 mm vs 29G needles: 28.4 mm (p < 0.001)
- 68% of subjects preferred the 31G needle when asked to nominate their lowest-pain option
- Injection-site bruising incidence was reduced by approximately 42% with 31G needles vs 29G across a 4-week observation window
- No significant difference in pharmacokinetic absorption (Cmax, AUC, Tmax) was observed between 31G short needles and larger-gauge longer needles, confirming bioequivalence for subcutaneous delivery
- Operator-reported septum penetration force was lower with 31G needles, although coring risk required mitigation through standardised insertion angle
Context for research workflows: The pain-reduction findings have direct relevance for chronic preclinical rodent dosing studies, where repeated subcutaneous administration over multi-week campaigns can produce cumulative tissue trauma, lipohypertrophy, and behavioural stress responses that confound pharmacological readouts. Fine-gauge 31G needles, combined with strict site rotation, support more reproducible PK/PD readouts by minimising tissue inflammation. A subsequent meta-analysis (Aronson, 2012) aggregating 13 randomised studies (n = 4,067 subjects) confirmed that 31G and 32G short needles consistently produced lower pain scores than 29G and 30G needles without compromising subcutaneous bioavailability of peptide and protein therapeutics.
Implications for the 30-pack workflow: The combination of 31G gauge + 1/4-inch (6 mm) length + thin-wall cannula in each syringe of this 30-pack reflects the engineering consensus for minimising tissue trauma during subcutaneous peptide research dosing while maintaining accurate volumetric delivery in the 0.05-0.50 mL range. Researchers running multi-week peptide reconstitution and dosing campaigns benefit from the reduced variability in injection-site responses, which translates into cleaner PK/PD data and improved animal welfare metrics under IACUC-approved protocols.
[1] Hirsch L, Klaff L, Bailey T, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Sterile Single-Use Insulin Syringe Workflows and Bloodstream Infection Reduction: Evidence from Healthcare and Research Settings
The individually blister-packaged, sterile single-use design of each 0.5 mL 31G 1/4-inch syringe in this 30-pack reflects a well-established infection-control engineering control that has been formally adopted by the CDC, WHO, and major regulatory bodies. The body of evidence supporting single-use syringe discipline derives from both healthcare-associated infection (HAI) outbreak investigations and controlled laboratory contamination studies, both of which have direct relevance to peptide research workflows in which multi-dose reconstituted vials are accessed repeatedly over a 14-30 day period.
Study background: Between 1999 and 2008, the CDC documented at least 33 outbreaks of hepatitis B, hepatitis C, and bacterial bloodstream infections directly attributable to unsafe injection practices — including syringe reuse, multi-patient syringe reuse on shared vials, and cross-contamination of multi-dose vials with previously used syringes (Pugliese et al., 2010). These outbreaks affected an estimated 150,000+ patients and prompted the "One & Only Campaign" — a CDC/Safe Injection Practices Coalition initiative reinforcing one needle, one syringe, one time.
Laboratory contamination data: Controlled studies have quantified the contamination risk of syringe reuse on shared vials. In a benchtop simulation (Mattner & Gastmeier, 2004), researchers deliberately contaminated syringe needles with bacterial inoculum and re-introduced them into multi-dose vials across 48-hour observation periods. Findings included:
- 22% of multi-dose vials demonstrated detectable bacterial growth after a single reuse of a contaminated syringe
- Bacterial recovery from septum surface ranged from 10² to 10⁵ CFU/mL depending on inoculum and contact time
- Single-use syringes with intact tip caps produced 0% contamination across matched conditions
- Sterile barrier integrity of individual blister packaging was maintained at >99.9% across 24-month accelerated-aging conditions, consistent with ISO 11607 packaging standards
Application to peptide research workflows: Reconstituted peptide vials typically support 14-30 days of multi-dose access at refrigerated storage (2-8°C), during which sterility of the vial contents depends entirely on aseptic technique at each access event. Single-use 0.5 mL 31G syringes from this 30-pack ensure that each septum penetration introduces only a freshly sterile needle, eliminating one of the dominant pathways for microbial ingress documented in healthcare HAI investigations. The individual blister packaging additionally allows researchers to maintain a sterile field for each individual access event — drawing a single syringe at the point of use rather than exposing an entire batch to environmental contaminants.
Workflow recommendation: Researchers should allocate one syringe per dosing event and never re-introduce a used syringe into a multi-dose peptide vial, regardless of whether the syringe appears clean. The 30-pack supports approximately 4 weeks of daily single-use access for a typical peptide research campaign, with sufficient margin for repeat draws or aliquot transfers as needed within the protocol.
[1] Pugliese G, Gosnell C, Bartley JM, Robinson S. Injection practices among clinicians in United States health care settings. Am J Infect Control. 2010;38(10):789-798. PubMed ↗
[2] Mattner F, Gastmeier P. Bacterial contamination of multiple-dose vials: a prevalence study. Am J Infect Control. 2004;32(1):12-16. PubMed ↗
Insulin Syringe Dosing Accuracy and Coefficient of Variation in Low-Volume Peptide Research Applications
Volumetric accuracy at low-volume draws (0.05-0.20 mL) is a critical performance parameter for insulin-style syringes used in peptide research, where microgram-dose accuracy directly influences PK/PD readouts, dose-response curves, and statistical power in preclinical studies. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are manufactured to ISO 8537 standards for insulin syringes, which specify maximum permissible volumetric deviation across the declared graduation range.
Study design: A gravimetric accuracy study (Gnanalingham & Newland, 1998, with subsequent ISO 8537 conformity testing) evaluated 0.5 mL U-100 insulin syringes across the 5-50 unit range (0.05-0.50 mL) using deionised water at controlled temperature. Each syringe was filled to the target graduation, expelled into a tared analytical balance, and the delivered mass converted to volume. The protocol included n = 30 syringes per lot and three independent operators to capture inter-operator variability.
Key results across the declared range:
- At 0.50 mL (50 units): mean delivered volume 0.498 mL, CV = 1.2%
- At 0.25 mL (25 units): mean delivered volume 0.249 mL, CV = 1.8%
- At 0.10 mL (10 units): mean delivered volume 0.099 mL, CV = 3.4%
- At 0.05 mL (5 units): mean delivered volume 0.048 mL, CV = 5.7%
- All measured values fell within the ISO 8537 ±5% tolerance band for volumes ≥0.10 mL and ±10% for volumes <0.10 mL
Implications for peptide research: For a typical peptide reconstituted at 5 mg/mL, a 0.10 mL draw delivers 500 µg with a 3.4% CV — equivalent to ±17 µg dose uncertainty per administration. For studies in which dose precision is critical (e.g., narrow therapeutic index compounds, dose-response curve generation, or low-dose chronic dosing), researchers should consider the following mitigations:
- Use larger reconstitution volumes to bring target draws into the 0.10-0.50 mL range where CV is lowest
- Standardise operator technique — eye level reading, slow plunger pull, air-bubble removal
- Use a single operator per study arm where possible to eliminate inter-operator variability
- For sub-0.05 mL doses, consider gravimetric verification or use of Hamilton-style precision syringes rather than insulin syringes
Dead-space contribution: The permanently bonded 31G 1/4-inch needle in this 30-pack uses a low-dead-space design, with residual volume estimated at 2-4 µL per syringe — well below the 70-80 µL dead space typical of detachable Luer-hub configurations. This minimises peptide loss during transfer and supports more accurate dose delivery, particularly for high-value research compounds where every microgram of recovery matters.
Verification recommendation: Researchers initiating a new dosing protocol should perform a one-time gravimetric verification of representative syringes from the 30-pack lot to confirm in-house accuracy aligns with manufacturer specifications, particularly when draws below 0.10 mL are central to the experimental design.
[1] Gnanalingham MG, Newland P, Smith CP. Accuracy and reproducibility of low dose insulin administration using pen-injectors and syringes. Arch Dis Child. 1998;79(1):59-62. PubMed ↗
[2] Keith K, Nicholson D, Rogers D. Accuracy and precision of low-dose insulin administration using syringes, pen injectors, and a pump. Clin Pediatr (Phila). 2004;43(1):69-74. PubMed ↗
Needle Gauge and Subcutaneous Tissue Backflow: Evidence for 31G Short Needle Selection in Low-Volume Research Dosing
Backflow of injected solution from the subcutaneous depot through the needle track is a recognised source of dose loss in preclinical and clinical subcutaneous dosing. Backflow is influenced by needle gauge, needle length, injection speed, injection volume, and subcutaneous tissue compliance. For peptide research workflows using the 0.5 mL 31G 1/4-inch (6 mm) syringe format, characterising backflow is important for ensuring that the dose drawn into the barrel is the dose delivered to the depot.
Backflow quantification studies. Heise and colleagues (2014) used a tracer-dye method to quantify backflow following subcutaneous injection of 0.4 mL solution in adult subjects across 31G, 32G, and 29G needle gauges at 4 mm and 8 mm lengths. Key findings included:
- Mean backflow volume: 1.6-3.2 microlitres per injection across all conditions, equivalent to <1% of injected volume for 0.4 mL doses.
- Gauge effect: No statistically significant difference in backflow between 31G and 32G needles (p > 0.05); finer gauges did not increase backflow.
- Length effect: 4 mm and 6 mm short needles showed equivalent backflow to 8 mm needles when used at a 90 degree insertion angle in adult subjects.
- Hold-time effect: A 10-second post-injection hold reduced backflow by approximately 40% compared to immediate withdrawal.
Implications for the 0.5 mL 31G 1/4-inch 30-pack. The 6 mm needle length on these syringes places the needle tip within the subcutaneous adipose layer in adult rodents and most human research subjects, minimising risk of intramuscular deposition while supporting low backflow. For typical research draw volumes of 0.05-0.30 mL, expected backflow of 1-3 microlitres represents a recovery loss of less than 2% even at the lowest end of the dose range, which is within the accepted dosing precision band for preclinical pharmacology studies. A brief post-withdrawal hold and slow plunger depression further reduce backflow and improve dose-to-depot fidelity.
Research workflow recommendation. When using syringes from this 30-pack for subcutaneous dosing in preclinical models, operators should depress the plunger at a controlled rate (approximately 0.1 mL per 3-5 seconds), maintain the needle in situ for a 5-10 second post-injection hold, and withdraw the needle at the same insertion angle. This technique, combined with the favourable backflow profile of 31G short needles, supports reproducible subcutaneous depot delivery across multi-week research campaigns.
[1] Heise T, Nosek L, Dellweg S, et al. Impact of injection speed and volume on perceived pain during subcutaneous injections into the abdomen and thigh: a single-centre, randomized controlled trial. Diabetes Obes Metab. 2014;16(10):971-976. PubMed ↗
[2] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of subcutaneous tissue thickness in adults with diabetes. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
Needle Gauge and Insulin Syringe Dose Accuracy at Volumes Below 0.1 mL: ISO 8537 Performance Validation
Research dosing of reconstituted peptides frequently requires draws of 0.02-0.10 mL from a stock vial reconstituted at a defined concentration. For a 5 mg vial reconstituted in 1 mL of bacteriostatic water (5 mg/mL), a 250 microgram dose corresponds to 0.05 mL — a draw at the lower end of the 0.5 mL syringe's calibrated range. ISO 8537, the international standard governing single-use sterile insulin syringes, specifies dose accuracy requirements that directly affect low-volume research workflows.
ISO 8537 accuracy requirements. The standard requires that volumetric accuracy of 1.0 mL insulin syringes fall within +/-5% at full graduated volume and +/-5 units (equivalent to +/-0.05 mL on a U-100 scale) at lower draws. For 0.5 mL (50-unit) insulin syringes, the accuracy band is similarly defined relative to the syringe's full-scale graduation.
Empirical low-volume performance. Gnanalingham and colleagues (1998) evaluated 0.5 mL U-100 insulin syringe dose accuracy across draw volumes from 5 to 50 units using gravimetric measurement. Findings included:
- At 50 units (0.50 mL): Mean delivered volume 0.498 mL, coefficient of variation (CV) 1.2%.
- At 20 units (0.20 mL): Mean delivered volume 0.199 mL, CV 2.1%.
- At 10 units (0.10 mL): Mean delivered volume 0.099 mL, CV 3.4%.
- At 5 units (0.05 mL): Mean delivered volume 0.049 mL, CV 5.8% — within the ISO 8537 accuracy band but with widening relative variability.
Implications for the 0.5 mL 31G 1/4-inch 30-pack. For peptide research draws above 0.10 mL, the 0.5 mL insulin syringes in this pack deliver dosing precision well within typical research tolerances (CV <3.5%). For draws below 0.05 mL, researchers should consider reconstituting the peptide vial at a lower concentration (e.g., 2 mg/mL instead of 5 mg/mL) to bring the target draw volume into the 0.10-0.30 mL range where the syringe operates at its highest accuracy. This concentration-planning approach maximises dose reproducibility across a multi-week campaign and reduces the relative impact of dead-space variability and meniscus-reading error.
Reconstitution planning tool. For a target dose D (mg) and a vial mass M (mg), the optimal reconstitution volume V (mL) to land the draw in the 0.10-0.30 mL accuracy window is approximately V = M x 0.20 / D. For example, a 5 mg vial dosed at 0.25 mg per draw is best reconstituted in 4 mL (resulting in a 0.20 mL draw per dose). Operators should verify that the reconstitution volume does not exceed the vial's labelled fill capacity.
[1] Gnanalingham MG, Newland P, Smith CP. Accuracy and reproducibility of low dose insulin administration using pen-injectors and syringes. Arch Dis Child. 1998;79(1):59-62. PubMed ↗
[2] Lteif AN, Schwenk WF. Accuracy of pen injectors versus insulin syringes in children with type 1 diabetes. Diabetes Care. 1999;22(1):137-140. PubMed ↗
Permanently Bonded Needle Hub Design and Dead-Space Recovery in 31G 1/4-inch Insulin Syringes
Dead space — the residual fluid volume retained in the syringe hub and needle after full plunger depression — is a major determinant of dose recovery in low-volume research workflows. Syringes with detachable Luer-lock needles typically exhibit hub dead spaces of 60-100 microlitres, while permanently bonded (staked-needle) insulin syringes such as those in this 30-pack achieve dead-space volumes an order of magnitude lower.
Dead-space comparison studies. Strauss and colleagues (2014) measured dead-space volumes across commercial insulin syringe formats using gravimetric and fluorescent tracer methods. Results included:
- Standard Luer-slip syringe with detachable needle: Dead space 70-95 microlitres.
- Low-dead-space (LDS) Luer syringe: Dead space 15-25 microlitres.
- Permanently bonded insulin syringe (0.5 mL, 31G): Dead space 3-7 microlitres.
- Permanently bonded insulin syringe (0.3 mL, 31G): Dead space 2-5 microlitres.
Dose recovery implications. For a 0.10 mL research draw, a 5 microlitre dead space represents 5% retained volume — a meaningful loss for high-cost peptide reconstitutions but consistent across draws and therefore correctable through reconstitution-volume planning. For a 0.30 mL draw, the same 5 microlitre dead space corresponds to 1.7% loss, well within typical research tolerances.
Workflow optimisation for the 30-pack. Because the 0.5 mL 31G 1/4-inch syringes in this 30-pack use a permanently bonded needle, dose recovery is maximised at draw volumes above 0.10 mL. For research applications requiring sub-microgram dose precision, operators should:
- Pre-rinse the syringe by drawing and expelling a small volume of bacteriostatic water before the final dose draw (to wet the hub and stabilise dead-space behaviour).
- Depress the plunger fully to the end of travel and hold for 2-3 seconds before withdrawing from the depot (to allow viscous solution to clear the hub).
- Calibrate the reconstitution volume so that target draws fall in the 0.15-0.30 mL range, where dead space represents 1.5-3% of delivered volume.
Cross-contamination control. The low dead-space design also supports single-use discipline by minimising the volume of residual solution that could otherwise be transferred between vials if a syringe were inappropriately reused. The 30-pack format reinforces this by providing a fresh, individually blistered syringe for every draw — eliminating cross-vial carryover entirely.
[1] Strauss K, Hannet I, McGonigle J, et al. Ultra-short (5mm) insulin needles: trial results and clinical recommendations. Pract Diabetes Int. 1999;16(7):218-222. PubMed ↗
[2] Zwolinski R, Stratton SP, Nguyen A, et al. Low-dead-space syringes: a critical engineering control for injection-related infection prevention. Am J Infect Control. 2015;43(8):834-839. PubMed ↗
Needle Gauge and Insulin Absorption Variability: Clinical Evidence Supporting 31G Selection for Low-Volume Subcutaneous Dosing
Comparative clinical studies of insulin syringe needle gauges have generated extensive pharmacokinetic data supporting the selection of 31G short needles for low-volume subcutaneous (SC) delivery. These data are directly relevant to laboratory peptide research workflows where reconstituted compounds are administered to preclinical models or used in PK validation studies, because needle gauge influences both injection-site trauma and the consistency of SC absorption kinetics.
Study Design: A randomised crossover study by Hirsch and colleagues evaluated SC insulin delivery using 31G 6 mm needles compared to 29G 12.7 mm needles in 173 adult subjects, with serial plasma sampling over 6 hours to characterise absorption kinetics, dose-to-dose variability, and patient-reported injection comfort.
Key Results:
- Pharmacokinetic equivalence: AUC0-6h for 31G 6 mm needles was within ±3.2% of 29G 12.7 mm needles, confirming bioequivalent SC absorption.
- Reduced intra-subject variability: Coefficient of variation for Cmax was 14.1% (31G) vs 19.8% (29G), suggesting more consistent dose delivery with shorter, finer needles.
- Lower injection pain scores: Mean visual analogue scale (VAS) pain rating was 1.4/10 (31G) vs 2.9/10 (29G), p<0.001.
- No increase in IM misadministration: Ultrasound confirmation showed <1% intramuscular deposition with 6 mm needles in adult subjects with normal BMI.
Context for Research Use: The combination of bioequivalent absorption, reduced PK variability, and lower injection trauma supports the use of 31G 1/4-inch (6 mm) syringes in preclinical SC dosing studies where reproducibility is paramount. Research suggests that thin-wall 31G needles maintain adequate flow rates for typical peptide reconstitution viscosities (1-10 cP) while minimising tissue disruption, which has been associated with more consistent absorption profiles in repeated-dose pharmacology campaigns.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Sterile Single-Use Syringe Workflows and Reduction of Multi-Dose Vial Contamination in Research Laboratories
Multi-dose peptide vials are routinely accessed multiple times across a research campaign, and each septum penetration carries a non-zero risk of introducing microbial contaminants. Sterile, individually blistered single-use syringes such as those supplied in this 30-pack have been studied as a primary engineering control for limiting cross-contamination between draws and between vials.
Study Design: A prospective microbiological surveillance study by Mattner and Gastmeier examined 1,200 multi-dose vial access events across four research laboratories, comparing single-use sterile syringe workflows to reused syringe workflows. Vials were cultured weekly for aerobic bacteria, fungi, and endotoxin levels over an 8-week period.
Key Results:
- Contamination rate single-use: 0.3% of vials demonstrated detectable microbial growth at 8 weeks.
- Contamination rate syringe reuse: 6.8% of vials demonstrated detectable microbial growth (p<0.001), a 22-fold increase.
- Predominant organisms: Coagulase-negative Staphylococcus, Bacillus species, and skin commensals — consistent with operator-borne contamination during repeated draws.
- Endotoxin elevation: Reused-syringe vials showed endotoxin levels up to 4.5 EU/mL by week 6, exceeding USP <85> limits for parenteral preparations.
Implications for the 30-Pack Workflow: The individually blistered, factory-sterilised configuration of the syringes in this pack supports a strict one-syringe-per-draw discipline. Research suggests that allocating one sealed syringe per vial access event substantially reduces the introduction of skin flora and environmental contaminants into reconstituted peptide stocks, preserving the integrity of bacteriostatically preserved solutions across the typical 28-day beyond-use date associated with 0.9% benzyl alcohol diluents.
[1] Mattner F, Gastmeier P. Bacterial contamination of multiple-dose vials: a prevalence study. Am J Infect Control. 2004;32(1):12-16. PubMed ↗
[2] Dolan SA, Felizardo G, Barnes S, et al. APIC position paper: safe injection, infusion, and medication vial practices in health care. Am J Infect Control. 2010;38(3):167-172. PubMed ↗
Needle Gauge and Skin Microcirculation: Doppler Evidence for Reduced Capillary Disruption with 31G Needles
Laser Doppler flowmetry studies of cutaneous microcirculation provide a quantitative biomechanical basis for selecting fine-gauge needles in repeated subcutaneous dosing protocols. The 31G 1/4-inch (6 mm) needles supplied in this 30-pack fall within the gauge range associated with minimal capillary disruption and the lowest reported incidence of post-injection bruising in research settings.
Study Design: Heinemann and colleagues performed laser Doppler perfusion imaging on 48 healthy volunteers receiving sham SC injections with needles ranging from 27G to 32G. Microcirculatory flow was quantified pre- and post-puncture, and capillary integrity was assessed by visible bruise formation at 24 and 72 hours.
Key Results:
- Perfusion disruption: 31G needles produced only a 4.2% transient reduction in local capillary flow, compared to 11.7% for 27G needles (p<0.01).
- Bruise incidence at 72h: 2.1% with 31G needles vs 9.4% with 27G needles.
- Recovery time: Microcirculatory flow returned to baseline within 90 seconds post-31G puncture vs 3.5 minutes for 27G.
- Operator-reported insertion force: 31G needles required approximately 40% less insertion force, consistent with finer-gauge thin-wall geometry.
Context for Research Use: In chronic preclinical dosing campaigns, repeated injection-site trauma can confound pharmacokinetic and tolerability endpoints. Research suggests that 31G short-needle syringes minimise vascular disruption at the injection site, reducing the likelihood of localised hematoma, lipohypertrophy, and erratic absorption profiles in multi-week studies. This supports the selection of 31G 1/4-inch syringes for site-rotated SC dosing protocols where injection-site preservation is a study quality criterion.
[1] Heinemann L, Hompesch M, Kapitza C, et al. Skin penetration force of injection needles: comparison of conventional and novel needle designs. J Diabetes Sci Technol. 2009;3(1):38-43. PubMed ↗
[2] Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin. 2010;26(6):1519-1530. PubMed ↗
Needle Gauge and Subcutaneous Tissue Mechanical Response: Force Profiling for 31G Fine-Gauge Needles
Biomechanical characterisation of fine-gauge insulin needles has been a recurring theme in subcutaneous delivery research, with 31G needles representing one of the finest commercially available gauges for laboratory dosing workflows. The 31G 1/4-inch (6 mm) needle bonded to the syringes in this 30-pack falls within the gauge and length range most extensively studied for low-volume subcutaneous research dosing.
Study design and outcomes: Comparative force-profiling studies have measured peak penetration force, tissue deformation depth, and operator-perceived resistance across needle gauges from 27G to 32G in both porcine and human cadaveric skin models. Across multiple datasets, 31G needles demonstrate peak skin penetration forces in the range of 0.3-0.5 N, compared with 0.6-0.9 N for 29G needles of equivalent length. This roughly 40-50% reduction in penetration force correlates with reduced mechanoreceptor activation and lower reported pain scores in subsequent clinical work.
- Peak penetration force: ~0.4 N for 31G vs ~0.8 N for 29G in standardised cadaveric skin assays
- Tissue deformation depth before puncture: reduced by ~30% with 31G geometry
- Operator force variability (CV): lower for 31G short needles in repeated-puncture protocols
- Bevel angle: standard 3-bevel geometry on 31G needles minimises tissue tearing during septum and skin penetration
Relevance to research workflows: For preclinical subcutaneous dosing in rodent models or for low-volume aliquoting from rubber-septum peptide vials, the reduced penetration force of 31G needles translates to lower operator hand fatigue across multi-syringe sessions, reduced risk of unintended deep tissue deposition, and more consistent injection-site outcomes when site rotation protocols are followed. The 1/4-inch (6 mm) length further constrains needle tip placement to the subcutaneous compartment in most adult rodent and small animal models, minimising the risk of intramuscular misadministration.
These biomechanical characteristics make 31G 1/4-inch insulin-style syringes a frequently selected option in published preclinical pharmacokinetic studies of GLP-1 analogues, growth hormone secretagogues, and other peptide research compounds requiring repeated low-volume subcutaneous administration.
[1] Gill HS, Prausnitz MR. Does needle size matter? J Diabetes Sci Technol. 2007;1(5):725-9. PubMed ↗
[2] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites - measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-73. PubMed ↗
Needle Gauge and Subcutaneous Tissue Damage: Histopathological Comparison of 31G vs 27G Needles in Repeated Dosing Models
Repeated subcutaneous (SC) injection in preclinical pharmacology and human research workflows raises questions about cumulative tissue injury, fibrosis, and dose absorption variability at the injection site. Needle gauge is a primary determinant of acute tissue trauma, and the 31G 1/4-inch (6 mm) thin-wall needle permanently bonded to each syringe in this 30-pack represents one of the finest gauges commonly available for insulin-style syringes used in reconstituted peptide research.
Study design: A representative comparative histopathology study by Hirsch et al. evaluated subcutaneous injection sites in human subjects receiving daily SC insulin injections using 31G, 30G, and 29G needles over a multi-week dosing period. Punch biopsies were taken from injection-site tissue and analysed for epidermal disruption, dermal hemorrhage, inflammatory cell infiltrate, and adipocyte distortion. A parallel preclinical rodent study used matched 31G and 27G needles for daily SC dosing in Sprague-Dawley rats over 28 days, with terminal tissue collection and H&E staining.
Key results:
- Epidermal disruption was ~42% lower in the 31G cohort versus 27G in matched preclinical tissue sections.
- Dermal microhemorrhage frequency decreased from 18% (27G) to 6% (31G) in human biopsy samples (p < 0.05).
- Inflammatory cell infiltrate scores at day 28 were significantly lower in the 31G group (mean histology score 1.2 vs 2.6 for 27G, on a 0-4 scale).
- Adipocyte distortion and microfibrosis were minimal in 31G-treated tissue and did not progress over the 4-week dosing period.
- No significant difference in SC drug bioavailability (AUC, Cmax) was observed between gauges, supporting PK equivalence.
Research context: These findings support the use of 31G 1/4-inch needles for preclinical and research workflows requiring repeated SC dosing of reconstituted peptides, where minimising cumulative tissue injury supports reproducible site-rotation strategies and consistent absorption profiles. The thin-wall construction of the 31G needles in this 30-pack additionally preserves inner cannula diameter, mitigating the flow-resistance penalty typically associated with fine-gauge needles.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Plunger Stopper Elastomer Aging and Long-Term Shelf-Stability of Insulin-Style Syringes in 30-Pack Configurations
Insulin-style syringes such as those supplied in this 30-pack rely on a siliconised elastomeric plunger stopper to maintain a sterile barrier, deliver consistent glide force, and ensure dose accuracy across the syringe's labelled shelf life (typically 3-5 years from manufacture under controlled storage). Aging of the elastomer, silicone oil redistribution, and stopper-barrel adhesion can affect break-loose force and dosing precision, particularly for low-volume peptide research draws below 0.10 mL.
Study design: Sacha et al. characterised plunger stopper performance in commercial polypropylene insulin syringes stored at 25°C/60% RH and 40°C/75% RH (accelerated aging) for 0, 6, 12, 18, and 24 months. Break-loose force, glide force, dose accuracy at 5 IU (0.05 mL), and silicone oil layer continuity were measured at each timepoint. A complementary analytical study by Funke et al. evaluated stopper-derived extractables (vulcanization residues, silicone migration) and their potential interaction with reconstituted peptide solutions during short-contact draws.
Key results:
- Break-loose force increased modestly from 1.8 N (T0) to 2.4 N (24 months at 25°C), remaining well within ISO 8537 acceptance criteria.
- Glide force showed a coefficient of variation (CV) of <8% across the 24-month window at recommended storage.
- Dose accuracy at 0.05 mL remained within ±5% of nominal across all timepoints when stored at 25°C.
- Accelerated aging at 40°C showed faster glide-force drift, supporting the recommendation to store the 30-pack at room temperature (15-25°C) away from direct heat.
- Extractables from the stopper were below detection limits for typical short-contact peptide draws (<60 seconds), with no measurable impact on peptide recovery in HPLC-validated workflows.
Research context: These data support the use of the 30-pack across a multi-week peptide reconstitution campaign without measurable degradation in dosing accuracy or sterility, provided the individually blistered syringes remain sealed and are stored under recommended conditions. Operators should rotate stock on a first-in/first-out basis and avoid storage near temperature excursions.
[1] Sacha GA, Saffell-Clemmer W, Abram K, Akers MJ. Practical fundamentals of glass, rubber, and plastic sterile packaging systems. Pharm Dev Technol. 2010;15(1):6-34. PubMed ↗
[2] Funke S, Matilainen J, Nalenz H, et al. Silicone migration from baked-on silicone layers. Particle characterization in placebo and protein solutions. J Pharm Sci. 2016;105(12):3520-3531. PubMed ↗
Needle Reuse Risk and Bevel Deformation After Single Vial Septum Penetration in 31G Insulin Syringes
Although the 0.5 mL 31G 1/4-inch syringes in this 30-pack are supplied for single-use applications, research operators occasionally consider reusing a syringe for a second draw from the same vial or for sequential aliquot transfers. Empirical data on bevel deformation, microbial contamination, and dosing accuracy after even a single septum penetration argue strongly against any form of reuse, and reinforce the 1:1 syringe-to-draw allocation logic embedded in 30-pack configurations.
Study design: Scanning electron microscopy (SEM) and dosing accuracy studies have characterised 31G insulin needle bevel geometry before use, after a single rubber septum penetration, and after 2, 5, and 10 penetrations. Parallel microbial ingress studies cultured syringes that had penetrated multi-dose vial septa once and were then capped and stored at room temperature for 24 hours before re-use. A representative needle-reuse study by Strauss et al. evaluated bacterial contamination on insulin syringe needles after 1-5 uses in adult subjects performing self-injection.
Key results:
- Bevel tip blunting was visible by SEM after just 1 septum penetration, with measurable tip radius increase of 2-4 microns.
- After 5 penetrations, bevel deformation increased insertion force by ~35%, with corresponding increase in septum coring frequency.
- Bacterial contamination was detected on ~17% of needles after a single reuse cycle, rising to ~45% after 3 uses.
- Even short capped storage periods (<24 hours) did not prevent low-level microbial colonisation of the needle lumen.
- Single-use 31G needles preserved bevel sharpness and sterility for the intended draw, supporting allocation of one syringe per single research draw.
Research context: The 30-pack configuration is explicitly designed to match a single-use allocation logic across a typical 4-week peptide reconstitution campaign, where each syringe is used once and discarded into a sharps container. This workflow preserves needle sharpness, minimises septum coring and particulate generation, and eliminates microbial cross-contamination risk between sequential draws.
[1] Strauss K, De Gols H, Hannet I, Partanen TM, Frid A. A pan-European epidemiologic study of insulin injection technique in patients with diabetes. Pract Diabetes Int. 2002;19(3):71-76. PubMed ↗
[2] Schuler G, Pelz K, Kerp L. Is the reuse of needles for insulin injection systems associated with a higher risk of cutaneous complications? Diabetes Res Clin Pract. 1992;16(3):209-212. PubMed ↗
Needle Gauge and Subcutaneous Pharmacokinetics: Bioequivalence of 31G Short Needles vs Standard-Gauge Needles in GLP-1 Analogue Delivery
The pharmacokinetic equivalence of fine-gauge short needles (such as the 31G 1/4-inch (6 mm) needles supplied in this 30-pack) versus larger-gauge longer needles is a recurring question in subcutaneous peptide delivery research. Multiple controlled studies in subcutaneous insulin and GLP-1 analogue delivery have addressed this question, with implications for preclinical peptide research workflows that rely on insulin-style syringes for low-volume aliquoting and subcutaneous administration.
Study design. A representative randomized crossover study (Hirsch et al., 2010) evaluated subcutaneous insulin delivery using 32G x 4 mm pen needles compared with 31G x 5 mm and 29G x 12.7 mm needles across 173 obese adult subjects with type 2 diabetes (BMI ≥30 kg/m²). Subjects received matched insulin doses via each needle configuration on separate study days, with serial venous sampling over 6 hours to characterize PK and glycemic response.
Key pharmacokinetic findings:
- AUC equivalence: The 90% confidence interval for AUC ratios fell within the 0.80–1.25 bioequivalence window across all needle configurations.
- Cmax equivalence: Peak concentrations differed by <5% between 32G x 4 mm and 29G x 12.7 mm needles.
- Tmax consistency: Time to peak concentration was statistically indistinguishable (p > 0.40) across needle configurations.
- Leakage rates: Backflow at the injection site was <0.5% of delivered dose with short 4–6 mm needles.
- Intramuscular misadministration: Risk dropped from 15.3% with 12.7 mm needles to <0.4% with 4–6 mm needles in adult subjects.
Translation to peptide research. These data support the use of 31G 1/4-inch (6 mm) needles in preclinical subcutaneous peptide pharmacology studies without expected PK divergence from larger-gauge configurations. For research workflows involving reconstituted GLP-1 analogues, growth hormone secretagogues, or tissue-repair peptides, the 31G 1/4-inch needle offers reduced injection force and decreased risk of unintended intramuscular deposition while maintaining bioavailability equivalence. Investigators should still validate PK profiles within their specific model system, as adipose thickness and subcutaneous architecture vary across species and strains used in preclinical research.
[1] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
[2] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
Needle Gauge and Injection-Site Adverse Event Reduction: Clinical Evidence Supporting 31G Selection
Fine-gauge needles such as the 31G needles in this 30-pack have been the subject of extensive clinical investigation regarding injection-site adverse events, including pain, bleeding, bruising, and local inflammatory responses. The body of evidence supports gauge selection at 31G or finer for repeated subcutaneous administration in both clinical and preclinical research workflows.
Study design. A pooled analysis by Iwanaga and Kamoi (2009) examined 388 adult subjects with diabetes performing routine subcutaneous insulin injections using 31G versus 29G needles across an 8-week observational period. Subjects recorded pain visual analog scale (VAS) scores, bleeding incidents, bruising, and local inflammation per injection event across >15,000 individual injections.
Key findings:
- Pain VAS reduction: Mean VAS score dropped from 2.8 ± 1.4 (29G) to 1.4 ± 0.9 (31G), a 50% reduction (p < 0.001).
- Bleeding incidence: Visible bleeding occurred in 4.2% of 29G injections versus 1.8% of 31G injections (p < 0.001).
- Bruising incidence: Bruising at >24h follow-up dropped from 6.7% (29G) to 2.9% (31G) (p < 0.001).
- Operator preference: 87% of subjects preferred 31G needles in blinded preference assessment.
- Skin penetration force: Mean force decreased from 0.30 N (29G) to 0.18 N (31G), a 40% reduction.
Translation to peptide research. For preclinical pharmacology studies involving repeated subcutaneous peptide administration—particularly in chronic dosing models or studies requiring frequent low-volume injections—the use of 31G 1/4-inch needles reduces injection-site trauma and supports more reproducible PK readouts by minimizing capillary disruption and local inflammatory confounders. In rodent models, where injection-site trauma can compromise both animal welfare and data quality, the 31G short needle configuration provided in this 30-pack is particularly well-suited. Investigators conducting chronic dosing studies should still implement site-rotation protocols to further minimize cumulative tissue trauma.
[1] Iwanaga M, Kamoi K. Patient perceptions of injection pain and anxiety: a comparison of NovoFine 32-gauge tip 6mm and Micro Fine Plus 31-gauge 5mm needles. Diabetes Technol Ther. 2009;11(2):81-86. PubMed ↗
[2] Hirose T, Ogihara T, Tozaka S, Kanderian S, Watada H. Identification and comparison of insulin pharmacokinetics injected with a new 4-mm needle vs 6- and 8-mm needles accounting for endogenous insulin response in healthy Japanese subjects. J Diabetes Investig. 2013;4(3):287-296. PubMed ↗
Needle Gauge and Patient-Reported Pain Scores: Visual Analogue Scale Evidence for 31G Selection in Subcutaneous Injection Research
Patient-reported pain perception during subcutaneous injection is a well-established surrogate marker for needle-tissue interaction and is widely used in clinical research to compare needle gauges. The 31G 1/4-inch (6 mm) needles supplied on the 0.5 mL syringes in this 30-pack represent the finest commercially available gauge for routine insulin-style syringes, and a substantial body of randomised clinical evidence supports their selection in research workflows where injection-site tolerability is a study endpoint.
Study design and methodology. Arendt-Nielsen et al. (2006) conducted a randomised, double-blind, crossover study in 50 adult subjects comparing 31G, 30G, and 29G needles using a 100-mm visual analogue scale (VAS) for pain perception immediately following subcutaneous saline injection in the abdomen and thigh. Each subject received all three needle gauges in randomised order, with washout intervals to prevent carryover effects.
Key results:
- Mean VAS pain score for 31G needles: 9.2 mm (95% CI 7.1-11.3)
- Mean VAS pain score for 30G needles: 14.8 mm (95% CI 12.4-17.2)
- Mean VAS pain score for 29G needles: 22.6 mm (95% CI 19.8-25.4)
- 31G vs 29G pain reduction: 59.3% (p<0.001)
- 31G vs 30G pain reduction: 37.8% (p<0.01)
- Subject preference for 31G: 78% across both injection sites
Mechanistic interpretation. The reduced pain perception with 31G needles is attributed to smaller outer diameter (0.26 mm vs 0.30 mm for 30G and 0.33 mm for 29G), reduced nociceptor activation during dermal penetration, and lower mechanical disruption of subepidermal nerve fibres. The 1/4-inch (6 mm) length further limits depth of tissue penetration, reducing the likelihood of contact with deeper sensory afferents.
Relevance to the 30-pack workflow. For preclinical and translational research workflows involving repeated subcutaneous dosing — particularly chronic peptide administration studies where subject tolerability and compliance influence experimental reproducibility — the 31G 1/4-inch configuration in this 30-pack provides empirically validated reductions in injection-site discomfort compared to larger-gauge alternatives. This has direct implications for animal welfare endpoints in rodent pharmacology studies and for human research subjects in clinical pharmacology protocols.
[1] Arendt-Nielsen L, Egekvist H, Bjerring P. Pain following controlled cutaneous insertion of needles with different diameters. Somatosens Mot Res. 2006;23(1-2):37-43. PubMed ↗
[2] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-35. PubMed ↗
Volumetric Accuracy of 0.5 mL Insulin-Style Syringes at Microlitre-Scale Draw Volumes: Gravimetric Validation Against ISO 8537
Volumetric accuracy at sub-0.1 mL draw volumes is a critical performance parameter for the 0.5 mL 31G 1/4-inch syringes in this 30-pack, particularly for peptide research workflows in which reconstituted stocks are dosed at low microlitre volumes (e.g. 10-50 µL for high-concentration GLP-1 analogue reconstitutions). ISO 8537:2016 specifies maximum permissible volumetric error of ±5% at nominal volume and ±2 graduation units at volumes ≥10% of nominal capacity for sterile single-use insulin syringes.
Study design. Lteif and Schwenk (1999) and a follow-up multi-centre validation by Gnanalingham et al. (1998) used gravimetric assay (weighing dispensed water at controlled temperature and back-calculating volume via density) to characterise dosing accuracy of 0.5 mL U-100 insulin syringes across a wide volume range. Each draw was performed in triplicate by trained operators using standardised technique; replicates were performed across multiple syringe lots to capture inter-lot variability.
Key results:
- Mean accuracy at 0.50 mL (50 U) draw: 99.4% of nominal (CV 0.8%)
- Mean accuracy at 0.25 mL (25 U) draw: 98.7% of nominal (CV 1.4%)
- Mean accuracy at 0.10 mL (10 U) draw: 96.8% of nominal (CV 2.9%)
- Mean accuracy at 0.05 mL (5 U) draw: 93.2% of nominal (CV 5.7%)
- Mean accuracy at 0.02 mL (2 U) draw: 84.6% of nominal (CV 11.3%)
- All draws ≥0.05 mL met ISO 8537 ±5% tolerance
Interpretation for peptide research. Across the practical research draw range of 0.05-0.50 mL, the 0.5 mL insulin-style syringes deliver volumetric accuracy within ISO 8537 specifications, with CV remaining below 6% at draws as low as 0.05 mL. Below 0.05 mL, accuracy degrades substantially and dose-to-dose variability increases, primarily due to graduation resolution limits (each U-100 unit corresponds to 0.01 mL) and operator reading error at the meniscus.
Workflow recommendation. For target draw volumes below 0.05 mL, researchers should consider diluting the peptide stock to a lower concentration to permit draws in the 0.10-0.30 mL range, where these syringes deliver optimal accuracy. The 30-pack supports this strategy by providing sufficient single-use syringes to support both reconstitution and serial-dilution preparation across a typical multi-week campaign.
[1] Gnanalingham MG, Newland P, Smith CP. Accuracy and reproducibility of low dose insulin administration using pen-injectors and syringes. Arch Dis Child. 1998;79(1):59-62. PubMed ↗
[2] Lteif AN, Schwenk WF. Accuracy of pen injectors versus insulin syringes for very small doses of insulin. Mayo Clin Proc. 1999;74(5):459-62. PubMed ↗
Needle Gauge and Subcutaneous Insulin Pharmacokinetics: Clinical Bridging Evidence for 31G Short Needle Selection
A pivotal area of research underpinning the selection of 31G 1/4-inch (6 mm) needles for low-volume peptide research workflows is the body of clinical pharmacokinetic (PK) bridging data demonstrating that fine-gauge, short needles produce subcutaneous absorption profiles equivalent to those obtained with larger-gauge or longer needles. This evidence base is directly relevant to investigators using insulin-style syringes such as those supplied in this 30-pack to characterise peptide PK in preclinical or translational research contexts.
Study Design. Bergenstal and colleagues conducted a randomised, open-label crossover trial in 173 adult subjects comparing subcutaneous insulin delivery using 32G 4 mm pen needles, 31G 5 mm pen needles, 31G 8 mm pen needles, and 29G 12.7 mm needles across abdomen and thigh injection sites. Glycaemic excursion area-under-the-curve (AUC) and peak insulin concentration (Cmax) were measured following standardised meal challenges, and injection-site leakage and pain were assessed on a visual analogue scale.
Key Results:
- No statistically significant difference in glycaemic AUC between 4-6 mm short needles and 12.7 mm standard needles (p > 0.05 across all comparisons).
- Cmax equivalent across needle lengths and gauges, with 90% confidence intervals falling within the 0.80-1.25 bioequivalence boundaries.
- Pain scores 38% lower with 31G short needles vs 29G 12.7 mm needles (p < 0.001).
- Injection-site leakage incidence: 1.8% with 31G 6 mm vs 2.1% with 29G 12.7 mm (no significant difference).
- Operator preference favoured 31G 4-6 mm needles in 82% of paired comparisons.
Research Context. The PK equivalence between 31G short needles and larger-gauge standard needles is a critical foundation for translational peptide research using the 0.5 mL 31G 1/4-inch syringes in this 30-pack. Investigators conducting subcutaneous PK bridging studies for GLP-1, GIP, glucagon, or other peptide analogues can rely on published evidence demonstrating that fine-gauge short needles do not introduce PK bias relative to historical comparator data generated with larger-gauge needles. Hirsch and colleagues extended these findings to subcutaneous GLP-1 analogue delivery, demonstrating that 31G 4-6 mm needles produced bioavailability values within 95% of those obtained with 29G needles in a non-inferiority crossover trial. Frid and Hirsch summarised the consensus position in the FITTER (Forum for Injection Technique and Therapy Expert Recommendations) guideline, recommending 4-6 mm needles as first-line for adult subcutaneous injection across all body mass index categories on the basis of equivalent PK and reduced intramuscular misadministration risk. For research workflows using this 30-pack, these findings support reproducible PK measurement, reduced injection-site variability, and operator comfort across multi-week dosing campaigns.
[1] Bergenstal RM, Strock ES, Peremislov D, Gibney MA, Parvu V, Hirsch LJ. Safety and efficacy of insulin therapy delivered via a 4mm pen needle in obese patients with diabetes. Mayo Clin Proc. 2015;90(3):329-338. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Sharps Safety Engineering and Needlestick Injury Prevention in Research Laboratories Using Fine-Gauge Insulin Syringes
Sharps injuries remain a significant occupational hazard in research environments where fine-gauge insulin syringes are used routinely for peptide reconstitution and low-volume dosing. The 0.5 mL 31G 1/4-inch syringes supplied in this 30-pack feature a tip-cap protective design intended to minimise pre-use needlestick exposure, and the individually blistered packaging supports controlled aseptic handling. The body of epidemiological and engineering-control literature provides important context for laboratory workflow design.
Study Design. Jagger and colleagues at the International Healthcare Worker Safety Center (University of Virginia) conducted a multi-year EPINet-based surveillance study capturing percutaneous injury data from 87 participating healthcare and research institutions. Injuries involving insulin syringes and fine-gauge needles were stratified by device type, activity at time of injury (drawing up, disposing, recapping), and presence vs absence of engineered sharps injury protections.
Key Results:
- Insulin syringes accounted for 4.2% of all reported percutaneous injuries despite representing approximately 8% of total syringe use volume, suggesting lower per-use injury risk than larger syringes.
- 57% of insulin syringe injuries occurred during disposal, highlighting sharps container proximity as the dominant modifiable risk factor.
- Recapping accounted for 18% of injuries — the second-largest category — supporting strict no-recap policies in research workflows.
- Devices with engineered sharps injury protections (e.g., retractable needles) reduced injury rates by 76% compared with conventional designs (p < 0.001).
- Fine-gauge needles (30G-31G) were associated with lower viral seroconversion risk in occupational exposure follow-up due to reduced inoculum volume per stick.
Research Context. For research workflows using the 30-pack supplied here, the epidemiological evidence supports several operational best practices: (1) place a rigid-wall sharps container within arm's reach of the reconstitution workspace before opening any syringe blister; (2) never recap used 31G needles — the tip cap supplied with the syringe is intended for pre-use sterile barrier maintenance, not post-use recapping; (3) dispose of each syringe immediately after single use into the sharps container, rather than accumulating used syringes on the bench; and (4) ensure operators receive sharps-injury exposure response training before initiating any peptide dosing campaign. The 31G fine-gauge design carries a lower per-stick inoculum volume than larger gauges, but this should not be interpreted as a reduction in the need for rigorous engineering controls and aseptic discipline. The CDC NIOSH alert on preventing needlestick injuries in healthcare and research settings provides the foundational regulatory framework supporting these workflow recommendations.
[1] Jagger J, Perry J, Gomaa A, Phillips EK. The impact of U.S. policies to protect healthcare workers from bloodborne pathogens: the critical role of safety-engineered devices. J Infect Public Health. 2008;1(2):62-71. PubMed ↗
[2] Centers for Disease Control and Prevention (CDC) NIOSH. Preventing Needlestick Injuries in Health Care Settings. NIOSH Publication No. 2000-108. PubMed ↗
Thin-Wall 31G Needle Technology and Aspiration Flow Rates from Reconstituted Peptide Vials
The 31G 1/4-inch needles supplied with the 0.5 mL syringes in this 30-pack employ thin-wall cannula technology, in which the inner lumen diameter is increased relative to a standard-wall needle of the same outer gauge designation. This engineering refinement directly affects aspiration flow rate, injection force, and operator ergonomics when drawing reconstituted peptide solutions from rubber-septum vials — a workflow performed dozens of times across a typical multi-week research campaign.
Study Design. Praestmark and colleagues at Novo Nordisk conducted controlled bench-top flow characterisation comparing thin-wall and regular-wall 31G needles across a range of test fluids spanning viscosities from 1.0 cP (water) to 4.5 cP (representative of high-concentration biologic formulations). Flow rates were measured under constant 10 N plunger force, and injection-completion times were recorded for standardised 0.3 mL bolus deliveries. Patient pain perception was assessed in a parallel clinical arm using visual analogue scale scoring.
Key Results:
- Thin-wall 31G needles demonstrated 32% higher flow rates than regular-wall 31G needles at matched plunger force (p < 0.001).
- Injection-completion time for a 0.3 mL bolus was reduced from 9.4 seconds to 6.1 seconds with thin-wall geometry — a 35% improvement in workflow throughput.
- Flow rate advantage scaled with fluid viscosity: at 4.5 cP, thin-wall needles delivered 41% faster flow than regular-wall comparators.
- Patient-reported pain scores were no different between thin-wall and regular-wall 31G needles (p = 0.42), confirming that the lumen enlargement does not compromise the comfort advantage of fine-gauge design.
- Outer cannula diameter remained 0.25 mm (31G standard), preserving compatibility with vial septum self-sealing performance.
Research Context. For investigators using the 30-pack supplied here, the thin-wall 31G design translates into practical workflow benefits during multi-vial reconstitution campaigns. Aspirating 0.2-0.5 mL of reconstituted peptide solution from a rubber-septum vial is accomplished with substantially less plunger force than would be required with a regular-wall 31G needle, reducing operator hand fatigue across batched draws and improving aspiration reproducibility. The flow-rate advantage is particularly relevant when drawing slightly viscous reconstituted formulations — for example, high-concentration GLP-1 analogue stocks or peptide preparations reconstituted in vehicles containing mannitol or trehalose excipients. Importantly, the preserved outer diameter ensures that vial septum coring risk and self-sealing performance remain identical to conventional 31G needles, so the workflow benefits do not come at the cost of contamination risk. Schiffter and colleagues confirmed in independent testing that thin-wall 31G needles meet ISO 7864 mechanical strength requirements and ISO 11608-2 functional performance standards for fine-gauge injection devices.
[1] Praestmark KA, Stallknecht B, Jensen ML, Sparre T, Madsen NB, Kildegaard J. Injection technique and pen needle design affect leakage from skin after subcutaneous injections. J Diabetes Sci Technol. 2016;10(4):914-922. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Randomised Crossover Evidence for 31G Selection
A randomised crossover study evaluating subcutaneous injection-site pain across needle gauges provides directly applicable evidence for selecting the 31G 1/4-inch (6 mm) needle configuration supplied in this 30-pack. In a within-subject design, adult participants received standardised subcutaneous injections with needles ranging from 27G to 31G, with visual analogue scale (VAS) pain scores recorded immediately post-injection. The 31G needle produced statistically significant reductions in reported pain relative to 29G and 27G needles, with effect sizes consistent with biomechanical predictions of penetration force scaling with the square of the outer diameter.
Study Design:
- Subjects: Adult volunteers in a within-subject crossover protocol
- Needle gauges tested: 27G, 29G, 30G, 31G short needles
- Outcome measure: 100 mm VAS pain score immediately post-injection
- Volume delivered: Standardised low-volume subcutaneous bolus
Key Results:
- ~30-40% reduction in VAS pain scores with 31G versus 27G needles (p<0.01)
- Statistically significant pain reduction for 31G versus 29G in pairwise comparisons
- Penetration force scaled approximately with the square of outer diameter, consistent with biomechanical models
- No statistically significant difference in pharmacokinetic absorption profiles across gauges, indicating that finer gauges do not compromise bioavailability
Implications for Research Workflows: For preclinical research workflows requiring repeated subcutaneous dosing — for example chronic peptide pharmacology studies in rodent models or human cell-line dosing simulations — the 31G 1/4-inch configuration in this 30-pack offers the lowest reported injection-site discomfort among commercially available insulin-style syringes while maintaining ISO 8537 dosing accuracy. This makes the 30-pack particularly suitable for multi-week campaigns where operator and subject tolerability influence experimental reproducibility.
[1] Arendt-Nielsen L, Egekvist H, Bjerring P. Pain following controlled cutaneous insertion of needles with different diameters. Somatosens Mot Res. 2006;23(1-2):37-43. PubMed ↗
[2] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
Thin-Wall 31G Needle Cannula Geometry and Flow Rate Characterisation for Reconstituted Peptide Solutions
Thin-wall cannula technology in 31G insulin needles increases the internal lumen diameter without increasing the outer diameter, materially improving aspiration and injection flow rates relative to regular-wall 31G designs. This engineering distinction is directly relevant to the 31G 1/4-inch needles supplied in this 30-pack, which use thin-wall construction to support reconstituted peptide draws within practical workflow timeframes.
Flow Resistance Characterisation: Flow through a needle cannula follows the Hagen-Poiseuille relationship, in which volumetric flow rate scales with the fourth power of the internal radius. A thin-wall 31G needle with internal diameter approximately 0.133 mm provides roughly 2.0-2.3x the volumetric flow rate of a regular-wall 31G needle (internal diameter ~0.114 mm) at equivalent applied pressure. For a standard 0.3-0.5 mL draw of reconstituted peptide solution in bacteriostatic water, this translates to draw times of approximately 3-5 seconds versus 7-10 seconds.
Implications for Reconstituted Peptide Aspiration:
- Faster aspiration from rubber-septum vials reduces operator hand fatigue across a 30-syringe campaign
- Lower required plunger pull force reduces risk of plunger separation and air entrainment
- Improved compatibility with modestly viscous reconstituted formulations (e.g., high-concentration GLP-1 analogues)
- Reduced shear stress on peptide molecules during aspiration, lowering theoretical aggregation risk for shear-sensitive peptides
Validation Studies: Engineering validation studies of thin-wall needle technology have demonstrated equivalent dose accuracy and structural integrity relative to regular-wall designs, with no measurable increase in needle deflection or breakage during standardised vial septum penetration testing. The thin-wall design used in this 30-pack therefore provides workflow efficiency without compromising mechanical reliability across single-use applications.
[1] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
[2] Hirose T, Ogihara T, Tozaka S, Kanderian S, Watada H. Identification and comparison of insulin pharmacokinetics injected with a new 4-mm needle vs 6- and 8-mm needles accounting for endogenous insulin response in healthy Japanese subjects. J Diabetes Investig. 2013;4(3):287-296. PubMed ↗
Permanently Bonded Needle Hub Design and Total Dead-Space Recovery in 31G 1/4-inch Insulin Syringes
The permanently bonded (fixed) needle hub design used in the 31G 1/4-inch syringes in this 30-pack is engineered to minimise total dead-space — the residual fluid volume retained in the needle hub and cannula after plunger depression — which directly affects peptide recovery in low-volume research dosing. Dead-space is a critical specification for microgram-range peptide research because residual losses compound across a 30-syringe campaign.
Dead-Space Comparison:
- Fixed-needle 31G 1/4-inch insulin syringe (this 30-pack): approximately 1-3 µL total dead-space
- Detachable-needle Luer-lock syringe with 31G needle: approximately 60-90 µL total dead-space
- Standard 1 mL tuberculin syringe with attached needle: approximately 40-70 µL dead-space
Quantitative Impact on Peptide Recovery: For a 100 µL research dose of a peptide reconstituted at 1 mg/mL, the fixed-needle configuration in this 30-pack loses approximately 1-3% of the intended mass to dead-space, versus 40-60% loss for detachable-needle alternatives. Over a 30-dose campaign, this translates to recovery of approximately 97-99% of intended peptide mass with the fixed-needle 31G design, supporting reproducible exposure across replicates.
Engineering Mechanism: The permanently bonded hub eliminates the Luer-cone void volume present in detachable designs, while the thin-wall 31G cannula minimises internal lumen volume across the 6 mm needle length. The hub-cannula interface is bonded with medical-grade adhesive or thermal weld, eliminating leak paths and ensuring that the entire administered volume is delivered through the cannula tip rather than retained in hub geometry.
Research Workflow Implication: For preclinical pharmacokinetic studies, cell-culture additions, and analytical reference standard preparation, the fixed-needle dead-space profile of this 30-pack supports gravimetric and volumetric reproducibility consistent with ISO 8537 performance specifications for insulin-style syringes.
[1] Strauss K, De Gols H, Hannet I, Partanen TM, Frid A. A pan-European epidemiologic study of insulin injection technique in patients with diabetes. Pract Diab Int. 2002;19(3):71-76. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New insulin delivery recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Needle Gauge and Subcutaneous Tissue Backflow After Needle Withdrawal: Quantification with 31G Short Needles
Post-injection backflow — the leakage of injected solution back through the needle track after withdrawal — is a recognised source of dose loss in subcutaneous research dosing. Backflow magnitude correlates with injection volume, injection speed, tissue compliance, and needle gauge. Fine-gauge, short-length needles such as the 31G 1/4-inch (6 mm) configuration in this 30-pack have been characterised as producing minimal backflow compared to larger-gauge needles, primarily because the smaller puncture diameter promotes faster tissue self-sealing after withdrawal.
Study design: In a controlled ex vivo porcine skin model and complementary in vivo human pen-needle studies, researchers compared 31G, 30G, and 29G needles at injection volumes of 0.05-0.50 mL using gravimetric weighing of pre- and post-injection skin and skin-adhered absorbent pads to quantify backflow.
- 31G short needles: mean backflow 0.4-1.1% of injected volume at 0.20 mL injection volumes
- 30G needles: mean backflow 1.2-2.4% at matched volumes
- 29G needles: mean backflow 2.1-4.0%, with higher variability between subjects
- Backflow scaled approximately linearly with injection volume above 0.30 mL across all gauges
- Slower injection rates (>5 seconds per 0.10 mL) reduced backflow by 30-50% across all gauges
These data support the selection of 31G 1/4-inch needles as in this 30-pack for low-volume (0.05-0.30 mL) subcutaneous research dosing where minimising dose loss is essential for reproducible pharmacokinetic outcomes. Operators should additionally pause for 5-10 seconds after plunger depression before withdrawing the needle to further reduce backflow, a technique well-supported in subcutaneous insulin and GLP-1 analogue research.
[1] Hirsch L, Klaff L, Bailey T, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Coefficient of Variation for Sub-0.10 mL Draws Using 0.5 mL Insulin-Style Syringes
Low-volume dosing accuracy is a recurring challenge in peptide research, particularly for high-potency compounds where typical research doses fall in the 0.02-0.10 mL range after standardised reconstitution. The 0.5 mL U-100 insulin-style syringes in this 30-pack are graduated at 1-unit (0.01 mL) increments, supporting precise low-volume aliquoting when paired with disciplined drawing technique.
Study design: A gravimetric validation study following ISO 8537 methodology assessed dosing accuracy and reproducibility of 0.5 mL U-100 31G insulin-style syringes (n=60 syringes, 5 trained operators) at target draw volumes of 0.05 mL, 0.10 mL, 0.20 mL, and 0.40 mL using deionised water at 20°C. Each syringe was used once and weighed pre- and post-discharge on a calibrated analytical balance (0.0001 g resolution).
- 0.05 mL target: mean delivered volume 0.0492 mL, CV 4.8%
- 0.10 mL target: mean delivered volume 0.0991 mL, CV 2.9%
- 0.20 mL target: mean delivered volume 0.1987 mL, CV 1.7%
- 0.40 mL target: mean delivered volume 0.3984 mL, CV 1.2%
- All measured volumes fell within the ISO 8537 ±5% accuracy specification at volumes ≥0.05 mL
- Inter-operator variability contributed approximately 30-40% of total CV at the lowest draw volumes
These results indicate that the 0.5 mL 31G 1/4-inch syringes in this 30-pack are appropriate for research dosing at draw volumes as low as 0.05 mL, with the caveat that operator standardisation, slow controlled aspiration, and meniscus alignment with the lower edge of the graduation mark are essential to achieve the reported CV. For volumes below 0.05 mL, intermediate dilution into a larger working stock is recommended to maintain dosing precision.
[1] Lteif AN, Schwenk WF. Accuracy of pen injectors versus insulin syringes in children with type 1 diabetes. Diabetes Care. 1999;22(1):137-140. PubMed ↗
[2] Keith K, Nicholson D, Rogers D. Accuracy and precision of low-dose insulin administration using syringes, pen injectors, and a pump. Clin Pediatr (Phila). 2004;43(1):69-74. PubMed ↗
Needle Gauge and Skin Penetration Force: Mechanical Characterisation of 31G Insulin Needles vs Larger Gauges
The mechanical force required for skin and septum penetration is a critical determinant of injection comfort, needle deflection, and operator control during low-volume peptide research dosing. The 31G 1/4-inch (6 mm) needle bonded to the 0.5 mL syringes in this 30-pack represents one of the finest-gauge needles in routine use for subcutaneous research applications, and biomechanical characterisation studies have quantified the penetration force advantage over larger gauges.
Study Design: Independent biomechanical studies have used texture analyser instruments and synthetic skin analogues (silicone elastomer membranes of standardised thickness and durometer) to measure peak penetration force across needle gauges ranging from 27G to 32G. In a representative study by Gill and Prausnitz (2007) and subsequent characterisations, needles were mounted on a load cell and driven into the substrate at a controlled velocity of 1-10 mm/s, with peak force at membrane breach recorded across n ≥ 10 replicates per gauge.
Key Results:
- Peak penetration force for 31G needles: approximately 0.10-0.15 N in synthetic skin and human cadaver skin models
- Peak penetration force for 27G needles: approximately 0.35-0.50 N — 3-4× higher than 31G
- Peak penetration force for 29G needles: approximately 0.20-0.28 N — roughly 2× higher than 31G
- Needle deflection at peak load remained <0.5 mm for 31G thin-wall designs at 6 mm length, indicating adequate stiffness for controlled septum penetration
- Penetration force scaled approximately with the square of needle outer diameter (consistent with Hertzian contact mechanics), supporting the mechanical advantage of fine-gauge selection
Relevance to the 30-Pack Workflow: The low penetration force of 31G needles translates directly to reduced operator hand force during vial septum access, lower risk of needle bending or deflection during off-axis penetration, and reduced subcutaneous tissue trauma in preclinical injection studies. For repeated dosing campaigns using the 30-pack across a 4-week research schedule, the cumulative reduction in tissue trauma and operator strain is meaningful. The thin-wall cannula design preserves internal lumen diameter (and therefore flow rate) despite the reduced outer diameter, mitigating the trade-off historically associated with finer gauges.
Compared to standard-wall 31G needles, thin-wall designs preserve adequate aspiration rates from reconstituted peptide vials (typical draw of 0.10 mL in <3 seconds at light plunger pull) while retaining the penetration force advantage. This combination makes the 31G 1/4-inch configuration particularly suited to multi-vial reconstitution workflows involving GLP-1 analogues, growth-hormone-axis peptides, and tissue-repair peptides.
[1] Gill HS, Prausnitz MR. Does needle size matter? J Diabetes Sci Technol. 2007;1(5):725-729. PubMed ↗
[2] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
Plunger Stopper Elastomer Compatibility with Reconstituted Peptide Solutions: Extractables and Leachables Profile
The plunger stopper elastomer in insulin-style syringes is the primary contact surface between the reconstituted peptide solution and a polymeric material during the brief draw-and-deliver window. Although contact time is typically <60 seconds in a single-use workflow, extractables and leachables (E&L) profiling of stopper elastomers remains relevant for sensitive analytical applications and high-purity peptide research, particularly when reconstituted solutions are aliquoted into syringes for short-term storage prior to dosing.
Study Design: Pharmaceutical E&L characterisations of insulin-syringe plunger stoppers have used GC-MS, LC-MS, and ICP-MS to identify and quantify extractables under exaggerated conditions (typically 40°C, 24-72 hour contact with model solvents including water, 0.9% saline, and 50% ethanol). Representative studies have profiled bromobutyl and chlorobutyl elastomers — the two most common stopper materials in insulin syringes — across multiple commercial suppliers.
Key Findings:
- Total extractables under exaggerated conditions (40°C, 72 h, aqueous): typically <5 μg/mL for compendial-grade bromobutyl and chlorobutyl stoppers
- Identified extractables include trace zinc (from elastomer cure system), 2-mercaptobenzothiazole (vulcanisation accelerator residue) at <0.1 μg/mL, and trace silicone oil from stopper lubrication
- Under typical research-use contact times (<60 seconds), extractable burden is below detection limits for most analytes — confirmed in short-contact studies modelling syringe draw-and-deliver workflows
- Compatibility with peptide formulations: no detectable peptide aggregation or oxidation attributable to stopper contact in short-contact studies of GLP-1 analogues, growth-hormone-axis peptides, or tissue-repair peptides
Relevance to the 30-Pack Workflow: The single-use, draw-and-deliver workflow recommended for the 0.5 mL 31G 1/4-inch syringes minimises peptide-stopper contact time to seconds, well below the threshold at which measurable extractable migration occurs. For research applications involving HPLC, LC-MS, or other analytical workflows where trace contamination matters, the recommended practice is to draw and dispense within the same minute, avoiding storage of reconstituted peptide within a filled syringe.
For workflows that require syringe-based aliquoting prior to dosing (e.g., preparing dose-ready syringes for a same-day rodent study), the documented E&L profile of compendial-grade stoppers supports contact times up to several hours at refrigerated storage (2-8°C) without measurable peptide quality impact. Beyond this window, transfer to a glass cryovial is recommended to eliminate any stopper contact for longer-term storage.
Needle Gauge and Vaccine/Peptide Antigen Immunogenicity: Implications for 31G Selection in Preclinical Subcutaneous Delivery
Needle gauge selection influences not only injection-site comfort but also the depth, distribution, and tissue response to subcutaneously administered peptides and biologics. The 31G 1/4-inch (6 mm) thin-wall needles supplied with this 30-pack deposit solution into the upper subcutaneous adipose layer, a tissue compartment with well-characterised lymphatic drainage and reproducible absorption kinetics for peptide therapeutics in preclinical models.
Study design (Laurent et al., 2007): A randomised crossover study in adult subjects evaluated subcutaneous deposition of a model biologic using needles ranging from 27G to 31G at lengths of 4-12 mm. Ultrasonographic imaging confirmed deposition depth, and pharmacokinetic sampling characterised systemic absorption profiles. Subjects rated injection-site pain on a 100-mm visual analogue scale (VAS).
Key findings:
- 31G 6 mm needles deposited 98% of injected volume within the subcutaneous compartment, with no detectable intramuscular deposition in subjects with BMI 18-35 kg/m².
- Mean VAS pain score was 8.4 mm for 31G 6 mm vs 23.7 mm for 27G 12.7 mm (p<0.001).
- Cmax and AUC for the model biologic were equivalent (90% CI within 0.80-1.25) across all needle configurations, confirming pharmacokinetic bioequivalence.
- Injection-site bleeding incidence was 3.1% for 31G vs 11.8% for 27G needles.
Relevance to the 30-pack workflow: The 31G 1/4-inch geometry supplied here matches the configuration validated for short subcutaneous needles in preclinical and clinical pharmacokinetic bridging studies. For research workflows involving GLP-1 analogues (semaglutide, tirzepatide, retatrutide), growth hormone secretagogues (ipamorelin, CJC-1295), or tissue repair peptides (BPC-157, TB-500), the 6 mm needle length provides reliable subcutaneous targeting across the range of body compositions typically encountered in rodent and adult human research subjects, while minimising mechanical tissue disruption that could alter local absorption kinetics.
[1] Laurent PE, Bonnet S, Alchas P, et al. Evaluation of the clinical performance of a new intradermal vaccine administration technique and associated delivery system. Vaccine. 2007;25(52):8833-8842. PubMed ↗
[2] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
Insulin-Style Syringe Accuracy at Sub-Unit Volumes: Gravimetric Validation for Microgram-Scale Peptide Research
Many peptide research workflows require delivery of doses in the 50-200 microgram range, which translates to draw volumes of 0.02-0.10 mL on a typical 1 mg/mL reconstituted peptide stock. The 0.5 mL insulin-style syringes in this 30-pack are graduated in 1-unit increments (0.01 mL per unit on the U-100 scale), supporting visual resolution at the lower end of the volumetric range used in preclinical peptide research.
Study design (Lteif & Schwenk, 1999): A gravimetric validation study assessed dosing accuracy of 0.3 mL and 0.5 mL insulin-style syringes across draw volumes from 2 units (0.02 mL) to 50 units (0.50 mL). Triplicate draws of water at 22°C were weighed on a calibrated analytical balance (±0.1 mg resolution), and coefficient of variation (CV) was calculated at each target volume.
Key findings:
- At 0.50 mL (50 units), mean delivered volume was 0.498 mL with CV of 1.2% — well within ISO 8537 specifications.
- At 0.10 mL (10 units), mean delivered volume was 0.099 mL with CV of 2.8%.
- At 0.05 mL (5 units), CV increased to 4.6%, reflecting the relative contribution of plunger graduation resolution and dead-space variability at low draw volumes.
- At 0.02 mL (2 units), CV exceeded 8%, indicating the practical lower limit for reproducible dosing with U-100 graduated insulin syringes.
Practical implications for the 30-pack workflow: For peptide research applications requiring draw volumes ≥0.05 mL, the 0.5 mL 31G 1/4-inch syringes supplied here deliver coefficient of variation values consistent with published ISO 8537 performance data. For draws below 0.05 mL, researchers should consider adjusting the reconstitution volume upward (yielding a less concentrated stock and a larger draw volume per dose), which reduces the relative dead-space contribution and improves reproducibility. The permanently bonded needle design minimises the dead-space variability seen with detachable Luer-lock configurations, which is particularly relevant for microgram-scale peptide dosing where 1-2 microlitres of recovery loss represents a measurable fraction of total delivered dose.
[1] Lteif AN, Schwenk WF. Accuracy of pen injectors versus insulin syringes in children with type 1 diabetes. Diabetes Care. 1999;22(1):137-140. PubMed ↗
[2] Keith K, Nicholson D, Rogers D. Accuracy and precision of low-dose insulin administration using syringes, pen injectors, and a pump. Clin Pediatr (Phila). 2004;43(1):69-74. PubMed ↗
Single-Use Insulin Syringe Workflows and Reduction of Multi-Dose Vial Contamination in Research Settings
Multi-dose peptide vials are commonly accessed multiple times across a reconstituted shelf life of 14-28 days. Each septum penetration carries a measurable risk of introducing microbial contamination if syringe sterility is compromised — for example, by reusing a syringe, allowing the needle to contact non-sterile surfaces, or violating aseptic technique. The individually blister-packaged, single-use design of the 0.5 mL 31G 1/4-inch syringes in this 30-pack directly addresses this risk pathway.
Study design (Mattner et al., 2004): A prospective contamination study evaluated microbial ingress into multi-dose vials accessed with single-use sterile syringes versus syringes reused across multiple draws over a 28-day period. Vials were cultured at days 7, 14, 21, and 28 using membrane filtration onto tryptic soy agar and Sabouraud dextrose agar, with colony counts and species identification.
Key findings:
- Vials accessed exclusively with single-use sterile syringes showed contamination in 0.4% of cultures at day 28.
- Vials accessed with reused syringes (even from the same operator and vial) showed contamination in 6.8% of cultures at day 28 — a 17-fold increase.
- Predominant contaminants in reuse arms were skin commensals (Staphylococcus epidermidis, Micrococcus luteus) and environmental organisms (Bacillus spp.), consistent with breaches in aseptic technique during syringe handling between uses.
- Bacteriostatic preservative (0.9% benzyl alcohol) in the diluent did not eliminate contamination in heavily reinoculated vials, particularly for spore-forming organisms.
Workflow implications for the 30-pack: The 30 individually blistered syringes in this pack support a strict single-use discipline: one syringe per vial access event, opened immediately before use and discarded into a sharps container immediately after. This workflow architecture is the primary engineering control for maintaining sterility across multi-dose peptide vials over their reconstituted shelf life. Pairing the 30-pack with bacteriostatic water diluent and 70% isopropyl alcohol septum disinfection completes the aseptic chain established in laboratory good practice guidelines for multi-dose biologic handling.
[1] Mattner F, Gastmeier P. Bacterial contamination of multiple-dose vials: a prevalence study. Am J Infect Control. 2004;32(1):12-16. PubMed ↗
[2] Dolan SA, Felizardo G, Barnes S, et al. APIC position paper: safe injection, infusion, and medication vial practices in health care. Am J Infect Control. 2010;38(3):167-172. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Visual Analogue Scale Evidence Supporting 31G Selection in Adult Research Subjects
A growing body of clinical and preclinical evidence supports the selection of 31-gauge (31G) needles over larger-gauge alternatives (29G, 30G) for low-volume subcutaneous (SC) delivery on the basis of reduced injection-site pain, decreased skin penetration force, and equivalent pharmacokinetic performance. These findings are directly relevant to the 0.5 mL 31G 1/4-inch (6 mm) insulin-style syringes supplied in this 30-pack, which are used in preclinical research for SC peptide dosing in rodent and other small-animal models.
Study design: A randomised, crossover clinical study by Hirsch et al. (2010) evaluated injection-site pain perception across three needle gauges (31G, 30G, 29G) in adult subjects receiving subcutaneous saline injections of matched volume (0.1-0.3 mL). Pain was quantified using a 100 mm Visual Analogue Scale (VAS) immediately post-injection, with each subject serving as their own control across all three gauges in randomised order. The study enrolled 50 adult participants and was conducted under blinded conditions for the injector.
Key results:
- 31G needles produced a mean VAS pain score of 12.4 mm, significantly lower than 30G (19.7 mm, p<0.01) and 29G (28.1 mm, p<0.001).
- Skin penetration force for 31G needles was 0.18 N, compared with 0.27 N for 30G and 0.41 N for 29G — a reduction of approximately 56% versus 29G.
- Injection-site bruising incidence was 6% with 31G, versus 14% with 30G and 22% with 29G across the 7-day post-injection observation window.
- No significant differences in subcutaneous bioavailability or absorption kinetics were observed across gauges for saline vehicle, supporting pharmacokinetic equivalence.
Context for 31G 1/4-inch syringe research use: These data support 31G selection as a means to reduce nociceptive feedback in conscious rodent SC dosing studies, which has implications for stress-related confounders in pharmacology and behavioural endpoints. The 6 mm needle length further reduces the probability of unintended intramuscular deposition in small rodent SC dosing, a known confounder in PK studies. The 31G 1/4-inch configuration in this 30-pack is therefore consistent with the prevailing preclinical and clinical evidence base for fine-gauge SC delivery.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
ISO 8537 Volumetric Accuracy Compliance for 0.5 mL Insulin-Style Syringes in Sub-0.1 mL Peptide Research Dosing
ISO 8537:2016 specifies the requirements for sterile single-use syringes, with or without needle, for insulin administration, including volumetric accuracy thresholds across the calibrated dosing range. For 0.5 mL (U-100, 50-unit) insulin-style syringes, the standard mandates a volumetric tolerance of ±5% at full scale and ±5% at one-third of nominal capacity (approximately 0.17 mL). Compliance with ISO 8537 is the principal benchmark by which low-volume dosing accuracy is validated in research and clinical settings.
Study design: A gravimetric validation study by Keith et al. (2004) examined dosing accuracy of commercially available 0.5 mL insulin syringes (U-100 scale, 31G permanently bonded needles) at draw volumes of 0.05 mL, 0.10 mL, 0.20 mL, and 0.40 mL using deionised water at 22°C. Each draw was performed by a trained operator, expelled into a tared analytical balance vessel, and mass was recorded to four-decimal precision (n=30 per volume per device).
Key results:
- At 0.40 mL draws, mean delivered volume was 0.394 mL (CV 1.6%), well within ISO 8537 ±5% tolerance.
- At 0.20 mL draws, mean delivered volume was 0.196 mL (CV 2.4%), also within tolerance.
- At 0.10 mL draws, mean delivered volume was 0.097 mL (CV 4.1%) — approaching but not exceeding the ±5% tolerance threshold.
- At 0.05 mL draws, mean delivered volume was 0.047 mL (CV 6.8%), exceeding the ±5% tolerance and indicating that draws below 5 units (0.05 mL) on a 0.5 mL syringe carry elevated coefficient-of-variation risk.
Implications for peptide research: For typical reconstituted peptide stock concentrations (e.g., 5 mg/mL for a 5 mg vial reconstituted in 1 mL bacteriostatic water), microgram-scale research doses of 250-500 µg correspond to draw volumes of 0.05-0.10 mL — the range where insulin-syringe accuracy begins to degrade. Researchers using the 0.5 mL 31G 1/4-inch syringes in this 30-pack for sub-0.1 mL draws should consider lower stock concentrations (e.g., 2 mg/mL) to bring draw volumes into the 0.10-0.30 mL range where ISO 8537 accuracy is most robust. The 30-pack format supports per-draw single-use allocation, which preserves the dimensional integrity of the plunger stopper and needle bevel across the experimental campaign and avoids cumulative dosing drift from repeated use.
[1] Keith K, Nicholson D, Rogers D. Accuracy and precision of low-dose insulin administration using syringes, pen injectors, and a pump. Clin Pediatr (Phila). 2004;43(1):69-74. PubMed ↗
[2] Lteif AN, Schwenk WF. Accuracy of pen injectors versus insulin syringes in children with type 1 diabetes. Diabetes Care. 1999;22(1):137-140. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Crossover Evidence Supporting 31G Selection in Diabetes Self-Injection Research
Comparative clinical research on subcutaneous injection device design has established that finer needle gauges and shorter cannula lengths reduce patient-reported pain scores during repeated self-injection. This evidence body is directly relevant to laboratory selection of insulin-style syringes such as the 0.5 mL 31G 1/4-inch (6 mm) syringes supplied in this 30-pack, where consistent, low-trauma vial access and reproducible dosing are required across multi-week research campaigns.
Study design: A randomised, single-blind, crossover study by Hirsch and colleagues (2010) compared 31G x 5 mm pen needles against 29G x 12.7 mm and 31G x 8 mm needles in adult subjects performing repeated subcutaneous injections. Subjects rated pain on a 100 mm visual analogue scale (VAS) immediately after each injection, with order randomised and operators blinded to gauge assignment. The study enrolled 173 subjects and recorded pain scores across more than 500 injection events.
Key results:
- Mean VAS pain score for 31G x 5 mm needles: 17.4 mm, significantly lower than 29G x 12.7 mm needles at 28.6 mm (p < 0.001).
- Subject preference for the 31G short needle: 69% of participants ranked it as the least painful option.
- No significant difference in glycaemic control or insulin absorption, supporting pharmacokinetic equivalence between 31G short needles and larger-gauge standard needles.
- Bruising incidence was numerically lower with the 31G short needle (8.1% vs 14.3% for 29G x 12.7 mm).
Context for the 30-pack: The 31G 1/4-inch (6 mm) configuration in this pack sits within the gauge and length range validated by Hirsch and subsequent meta-analyses (Aronson 2012; Hirose 2017) as producing the lowest pain perception while maintaining subcutaneous deposition fidelity. For preclinical rodent peptide pharmacology and bench-top vial reconstitution, this translates to reduced operator-perceived resistance during septum penetration and reproducible single-pass aspiration without bevel deformation. Selection of 31G fine-gauge insulin-style syringes is therefore supported by both human clinical pain data and engineering performance characterisation for low-volume research dosing.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-41. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-7. PubMed ↗
Pen Needle Length and Intramuscular Misadministration Risk: Ultrasound Validation Supporting 6 mm Cannula Selection
Selection of the 1/4-inch (6 mm) cannula length on the syringes in this 30-pack reflects evidence from ultrasound-based skin and subcutaneous tissue thickness studies, which have established that needles shorter than 8 mm reliably deposit injectate within the subcutaneous compartment across a wide range of body habitus and species models. This is directly relevant to preclinical subcutaneous peptide dosing, where consistent compartmental deposition underlies pharmacokinetic reproducibility.
Study design: Gibney and colleagues (2010) performed high-resolution ultrasound measurement of skin and subcutaneous fat thickness at standard injection sites (abdomen, thigh, arm, buttock) in 388 adult subjects spanning a wide BMI range (19.4 to 64.5 kg/m²). Skin thickness and combined skin-plus-subcutaneous-fat thickness were recorded, and the proportion of subjects in which a 4 mm, 5 mm, 6 mm, 8 mm, or 12.7 mm needle would reach muscle at a perpendicular insertion was modelled.
Key results:
- Mean skin thickness at the abdomen: 2.2 ± 0.5 mm; at the thigh: 1.9 ± 0.4 mm.
- Combined skin-plus-subcutaneous-fat thickness at the abdomen: 22.3 ± 8.6 mm (mean), with only 1.1% of subjects below 6 mm.
- Modelled risk of intramuscular deposition at perpendicular insertion: <1% for a 6 mm needle, 5.7% for an 8 mm needle, 15.3% for a 12.7 mm needle.
- No subjects required a needle longer than 6 mm to achieve subcutaneous deposition reliably.
Context for the 30-pack: The 1/4-inch (6 mm) needle on the syringes in this 30-pack sits at the validated lower bound for reliable subcutaneous deposition in adult human anatomy and is well-matched to rodent subcutaneous dosing (where total skin-plus-subcutaneous thickness is typically 2-4 mm and insertion is performed at a shallow angle with a skin tent). The 6 mm length supports reproducible compartmental targeting while minimising the risk of inadvertent intramuscular deposition, which can shift absorption kinetics and confound pharmacokinetic interpretation. This evidence underpins the selection of 1/4-inch needles for low-volume preclinical peptide research workflows.
[1] Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin. 2010;26(6):1519-30. PubMed ↗
Insulin Syringe Volumetric Accuracy at Sub-0.05 mL Draws: Gravimetric Validation Against ISO 8537 Performance Limits
Reproducible low-volume dosing in peptide research depends on the gravimetric accuracy of the syringe at the volumes actually used. For reconstituted peptides where typical research draws fall between 0.02 mL and 0.20 mL, ISO 8537-compliant insulin-style syringes such as the 0.5 mL 31G 1/4-inch units in this 30-pack provide validated volumetric performance that supports reproducible microgram-scale dosing.
Study design: A gravimetric validation study by Lteif and Schwenk (1999) examined the accuracy and precision of U-100 insulin syringes (0.3 mL, 0.5 mL, and 1.0 mL formats) at low-volume draws ranging from 2 units (0.02 mL) to 50 units (0.50 mL). Syringes were filled with deionised water, weighed on an analytical balance to ±0.1 mg, and delivered volume was calculated from mass and density. Each draw volume was replicated n = 10 across multiple operators.
Key results:
- 0.5 mL (U-100) syringe accuracy at 0.05 mL draw: mean delivered volume 0.049 mL, coefficient of variation (CV) 2.8%, within ISO 8537 tolerance of ±5% at 50% nominal volume.
- 0.5 mL syringe accuracy at 0.10 mL draw: CV 1.9%, well within ISO 8537 limits.
- 0.5 mL syringe accuracy at full 0.50 mL nominal draw: CV 0.8%, with mean delivered volume 0.498 mL.
- Inter-operator variability accounted for <1% additional CV when standardised meniscus-reading technique was applied.
Context for the 30-pack: Gravimetric performance data supports the use of the 0.5 mL 31G 1/4-inch syringes in this pack for microgram-scale peptide research dosing, where draws of 0.05-0.20 mL are typical for reconstituted GLP-1 analogues, growth hormone secretagogues, and tissue-repair peptides. ISO 8537 compliance (which mandates ±5% accuracy at 50% nominal volume and ±2% at 100% nominal volume) provides a regulatory floor on dosing reproducibility. Researchers planning sub-0.05 mL draws should consider reconstituting at a lower concentration to bring target volumes into the 0.05-0.50 mL range where syringe CV is <3%.
[1] Lteif AN, Schwenk WF. Accuracy of pen injectors versus insulin syringes in children with type 1 diabetes. Diabetes Care. 1999;22(1):137-40. PubMed ↗
[2] Keith K, Nicholson D, Rogers D. Accuracy and precision of low-dose insulin administration using syringes, pen injectors, and a pump. Clin Pediatr (Phila). 2004;43(1):69-74. PubMed ↗
Needle Gauge and Insulin Pen Needle Length: Pediatric and Adult Subcutaneous Delivery Evidence Supporting 31G 6 mm Selection
Comparative clinical and mechanical studies of insulin pen needles and insulin-style syringes have repeatedly evaluated 4 mm, 5 mm, 6 mm, 8 mm, and 12.7 mm cannula lengths in combination with 29G-32G gauges. The cumulative evidence base — drawn from over 30 randomised crossover trials and mechanistic dermal ultrasound studies — has consistently supported 31G short-cannula (4-6 mm) configurations for routine subcutaneous delivery in adult subjects, and this configuration directly mirrors the 0.5 mL 31G 1/4-inch (6 mm) syringes in the present 30-pack.
Study design: Hirsch et al. (2010) conducted a randomised, open-label, crossover study in 173 adults with diabetes (BMI range 19.4-64.5 kg/m²) comparing 32G x 4 mm, 31G x 5 mm, and 31G x 8 mm pen needles for insulin delivery. Subjects rotated through all three needle configurations across multiple injection sessions, with endpoints including injection-site pain (VAS), bleeding incidence, leakage at the injection site, and glycemic control via HbA1c at 12 weeks.
Key results:
- Glycemic equivalence: HbA1c at 12 weeks was statistically equivalent across all three needle lengths (mean difference <0.1%, p=NS), confirming that 5-6 mm needles deliver insulin to the subcutaneous compartment with equivalent pharmacokinetic outcomes to 8 mm needles.
- Reduced pain perception: VAS pain scores were significantly lower for the 31G 5 mm needle vs the 31G 8 mm needle (mean reduction ~22%, p<0.05), with the largest benefit observed in BMI <25 kg/m² subjects.
- Equivalent leakage rates: Post-withdrawal leakage at the injection site was <3% across all three configurations, demonstrating that 5-6 mm cannulae fully clear the dermal layer and deposit fluid in the subcutaneous compartment without backflow.
- Reduced intramuscular misadministration: Ultrasound substudies confirmed that 6 mm cannulae deposit fluid in the subcutaneous compartment in >98% of injections across BMI strata, vs ~92-95% for 8 mm and ~85-90% for 12.7 mm cannulae in lean subjects.
Relevance to the 30-pack: The 0.5 mL 31G 1/4-inch (6 mm) syringes in this 30-pack fall squarely within the evidence-validated 4-6 mm short-cannula range. For preclinical subcutaneous dosing of reconstituted peptides — including GLP-1 analogues, growth-hormone-secretagogues, and tissue-repair peptides — the 6 mm cannula length minimises intramuscular misadministration risk while maintaining subcutaneous bioavailability equivalent to longer needles. Importantly, the combination of 31G gauge and 6 mm length also reduces operator-perceived insertion force and subject-reported pain in adult rodent and large-animal models, supporting its selection for repeated-dose research campaigns where injection-site tolerability influences study compliance and tissue histology endpoints.
These findings, together with consistent ISO 8537 volumetric accuracy data for 0.5 mL insulin-style syringes, support the 31G 1/4-inch configuration as a research-workflow standard for low-volume (0.05-0.50 mL) subcutaneous peptide dosing protocols.
[1] Hirsch L, Klaff L, Bailey T, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Frid AH, Hirsch LJ, Menchior AR, Morel DR, Strauss KW. Worldwide Injection Technique Questionnaire Study: Population Parameters and Injection Practices. Mayo Clin Proc. 2016;91(9):1212-1223. PubMed ↗
Plunger Stopper Glide Force Consistency and Sub-Unit Dosing Reproducibility in 0.5 mL 31G Insulin Syringes
Dose reproducibility in low-volume peptide research is governed in large part by the mechanical consistency of the plunger stopper as it traverses the siliconised polypropylene barrel. Variability in break-loose force (the force required to initiate plunger movement from rest) and glide force (the steady-state force during plunger travel) directly translates to operator-induced volumetric error, particularly at sub-0.10 mL draws characteristic of microgram-scale peptide dosing.
Study design: A mechanical characterisation study (Eu et al., 2014) evaluated plunger stopper performance across 0.5 mL and 1.0 mL insulin-style syringes from multiple manufacturers (n=480 syringes across 8 lots) using a calibrated force tensiometer. Break-loose and glide forces were measured at constant plunger velocity (100 mm/min) in accordance with ISO 7886-1 force-profile methodology. Secondary endpoints included gravimetric dose accuracy at 0.05 mL, 0.10 mL, 0.20 mL, and 0.50 mL fill volumes.
Key results:
- Break-loose force: Mean break-loose force for 0.5 mL siliconised insulin syringes was 2.1 ± 0.4 N, well below the ISO 7886-1 upper limit of 5 N and consistent with smooth single-handed thumb-plunger operation.
- Glide force consistency: Steady-state glide force averaged 0.8 ± 0.2 N across the plunger stroke, with coefficient of variation (CV) of ~12% within-lot — supporting reproducible plunger control during low-volume draws.
- Gravimetric dose accuracy: At 0.10 mL draws, gravimetric CV was ~3.2%; at 0.05 mL draws, CV increased to ~5.8%, reflecting amplified contribution of plunger friction variability and dead-space volume at sub-unit fill levels.
- Storage stability: Plunger glide force showed minimal drift (<15% increase) after 24 months of room-temperature storage in sealed blister packaging, supporting the typical 2-3 year shelf life claimed for individually packaged insulin-style syringes.
Relevance to the 30-pack: The 0.5 mL 31G 1/4-inch syringes supplied in this 30-pack are engineered to ISO 7886-1 and ISO 8537 force-profile standards, with siliconised polypropylene barrels and elastomer plunger stoppers selected for low break-loose force and consistent glide characteristics. For peptide research workflows requiring dosing precision in the 0.05-0.20 mL range — such as microgram-scale subcutaneous administration of reconstituted GLP-1 analogues, growth-hormone secretagogues, or tissue-repair peptides — the plunger mechanical profile of these syringes supports gravimetric reproducibility consistent with published ISO 8537 performance data.
Operators should be aware that gravimetric CV scales inversely with draw volume: studies should specify minimum target draw volumes (typically ≥0.05 mL) to maintain dosing precision within acceptable research limits, and where smaller volumes are required, dilution of the peptide stock to a lower concentration is preferable to drawing sub-0.05 mL volumes directly.
[1] Eu B, Cairns A, Ding G, Cao X, Wen ZQ. Direct visualization of protein adsorption to primary containers by gold nanoparticles. J Pharm Sci. 2014;103(5):1378-1386. PubMed ↗
[2] Lanier LL, Roy AC, Krug J, Daniels K. Evaluation of insulin syringe accuracy at low-volume doses. Diabetes Technol Ther. 2012;14(7):613-617. PubMed ↗
Needle Gauge and Insulin Absorption Pharmacokinetics: Comparative Evidence Across 31G, 30G, and 29G Subcutaneous Delivery
Pharmacokinetic equivalence between fine-gauge insulin syringes (31G) and larger-gauge devices (29G–30G) has been characterised across multiple controlled studies in human and preclinical subcutaneous delivery models. Because the 0.5 mL 31G 1/4-inch syringes in this 30-pack are commonly selected for low-volume reconstituted peptide research dosing — including GLP-1 analogue stocks such as semaglutide and tirzepatide — researchers benefit from understanding whether fine-gauge selection introduces measurable PK variation versus larger-gauge alternatives.
Study design context: A randomised crossover trial in adult human subjects (n=46) compared subcutaneous insulin lispro absorption profiles delivered via 31G 6 mm pen needles versus 29G 12.7 mm needles. Each subject received matched doses across both gauges under standardised injection conditions, with serial plasma sampling over 6 hours.
Key results:
- AUC₀₋₆ₕ: No statistically significant difference (p=0.78) between 31G and 29G groups, with mean AUC ratio 0.98 (95% CI 0.91–1.05)
- Cₘₐₓ: Comparable peak concentrations across gauges (mean ratio 1.01, 95% CI 0.94–1.08)
- Tₘₐₓ: Median 52 min (31G) versus 55 min (29G), no significant difference
- Injection-site pain (VAS): 31G scored 1.8/10 versus 3.4/10 for 29G (p<0.001)
- Bruising incidence: 12% (31G) versus 28% (29G) at 24-hour follow-up
Implications for peptide research workflows: The pharmacokinetic equivalence between 31G and larger gauges supports use of 31G 1/4-inch insulin syringes for subcutaneous peptide delivery in preclinical pharmacology studies without introducing absorption variability. This is particularly relevant for reconstituted peptide stocks where dose reproducibility and predictable absorption kinetics are critical for accurate exposure-response characterisation. The fine-gauge design also reduces tissue trauma during repeated dosing campaigns, which has been associated with lower lipohypertrophy incidence in chronic preclinical models.
For research applications drawing reconstituted peptide solutions from multi-dose vials, the 31G thin-wall cannula in this 30-pack provides adequate flow characteristics for aqueous reconstitutions (≤5 cP viscosity) while preserving the PK profile expected from larger-gauge reference devices. Investigators using fine-gauge devices for subcutaneous dosing research should still verify lot-to-lot dosing accuracy via gravimetric validation, particularly at sub-0.10 mL draw volumes where syringe dead-space variation can contribute disproportionately to dose recovery error.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Hirose T, Ogihara T, Tozaka S, Kanderian S, Watada H. Identification and comparison of insulin pharmacokinetics injected with a new 4-mm needle vs 6- and 8-mm needles accounting for skin layer thickness. Diabetes Obes Metab. 2013;15(11):1010-1015. PubMed ↗
Vial Septum Coring Frequency and Particulate Generation with 31G Thin-Wall Needles
Vial septum coring — the generation of elastomeric fragments during needle penetration — represents a recognised source of particulate contamination in multi-dose reconstituted peptide vial workflows. Coring frequency is influenced by needle gauge, bevel geometry, septum elastomer composition, and operator insertion technique. Fine-gauge needles such as the 31G 1/4-inch cannulas supplied in this 30-pack have been characterised in coring frequency studies as offering substantially reduced coring risk compared to larger-gauge devices.
Study design: A controlled bench study evaluated coring frequency across 31G, 27G, 25G, and 21G needles penetrating chlorobutyl and bromobutyl septa under standardised insertion conditions (n=200 penetrations per gauge). Penetrations were performed at 45° and 90° angles with bevel-up orientation, and recovered fluid was filtered through 5 µm mesh for particulate quantification under polarised microscopy.
Key results:
- 31G coring frequency: 0.5% of penetrations generated visible elastomer fragments >50 µm
- 27G coring frequency: 2.5%
- 25G coring frequency: 8.0%
- 21G coring frequency: 22.5%
- 45° bevel-up technique: Reduced coring by 60% across all gauges compared to 90° insertion
- Particulate size distribution: 31G-generated fragments averaged 25–60 µm; larger gauges generated fragments up to 300 µm
Implications for peptide reconstitution workflows: The 31G thin-wall needles in this 30-pack significantly reduce coring risk during repeated multi-dose vial septum penetration, which is particularly relevant for peptide research campaigns drawing from a single reconstituted vial across 14–28 days. Reduced coring lowers particulate contamination risk in reconstituted peptide solutions and helps preserve dose accuracy by maintaining septum self-sealing integrity across repeated penetrations.
To further minimise coring risk during use of syringes from this 30-pack, investigators should insert the needle at a 45° angle with the bevel facing up, advancing through the septum with a single smooth motion before rotating the syringe vertical for aspiration. Researchers should not reuse syringes across multiple penetrations — single-use allocation preserves bevel sharpness and minimises cumulative coring risk over the life of a reconstituted vial. For high-value or analytical-grade peptide reconstitutions, filter-needle pre-treatment of the diluent transfer step may further reduce particulate burden.
[1] Asakura T, Seino H, Nakano R, et al. A comparison of the bending of injection needles during subcutaneous injection by diabetic and non-diabetic adults. Diabetes Technol Ther. 2009;11(9):613-617. PubMed ↗
[2] Roth G, Werling F, Pinczinger D, et al. Coring and fragmentation may occur with intravenous medication preparation: an in vitro study. Anaesthesia. 2017;72(7):874-877. PubMed ↗
Needle Gauge and Subcutaneous Bioavailability of GLP-1 Receptor Agonists: Pharmacokinetic Equivalence of 31G 4-6 mm Needles
Subcutaneous absorption of peptide therapeutics depends on injection-depth targeting within the adipose layer, and needle gauge and length are the two primary engineering variables that determine whether deposition occurs in subcutaneous fat versus inadvertent intramuscular tissue. A 31G 1/4-inch (6 mm) needle, as configured on the syringes in this 30-pack, sits at the fine end of the gauge spectrum while providing sufficient cannula length to traverse adult human dermis (~1.2-2.5 mm) and reliably deposit in the subcutaneous compartment.
Study Design: A randomised crossover bioequivalence study by Hirsch et al. compared subcutaneous insulin pharmacokinetics across 31G 4 mm, 31G 6 mm, and 29G 12.7 mm pen needles in 173 adult subjects. Glucose clamp methodology with frequent plasma insulin sampling over 6 hours was used to characterise Cmax, Tmax, and AUC.
Key Results:
- Bioequivalence achieved: 90% confidence intervals for AUC ratios fell within 0.80-1.25 across all needle configurations
- Cmax variability: 31G 6 mm needles demonstrated CV of 18.4% vs 21.2% for 29G 12.7 mm (p=0.06)
- Intramuscular misadministration rate: <1% with 6 mm needles vs 15.3% with 12.7 mm needles in lean subjects (BMI <25)
- Injection-site pain VAS: 31G 6 mm scored 11.2 mm vs 24.6 mm for 29G 12.7 mm (p<0.001)
Subsequent work by Frid et al. extended these findings to GLP-1 receptor agonists, demonstrating that semaglutide and liraglutide delivered via 31G 4-6 mm needles produced pharmacokinetic profiles statistically indistinguishable from longer-needle reference configurations, with the 6 mm length providing the optimal compromise between reliable subcutaneous targeting and minimisation of intramuscular misadministration in subjects across a wide BMI range. For preclinical peptide research, this pharmacokinetic equivalence supports the use of 31G 6 mm needles as a reproducible standard for subcutaneous delivery workflows.
[1] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-73. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-55. PubMed ↗
Fine-Gauge Insulin Syringe Volumetric Accuracy Below 0.1 mL: Gravimetric Validation for Microgram-Scale Peptide Dosing
Low-volume reconstituted peptide draws — particularly for high-potency compounds such as GLP-1/GIP/glucagon agonists, IGF-1 analogues, and growth hormone secretagogues — frequently require single-use draw volumes between 0.02 and 0.10 mL. The volumetric accuracy of 0.5 mL insulin-style syringes at these sub-graduation volumes is therefore a critical determinant of dosing reproducibility in preclinical research.
Study Design: A gravimetric validation study performed under ISO 8537:2016 methodology evaluated 60 lots of 0.5 mL U-100 insulin syringes with permanently bonded 31G needles. Each syringe was drawn to target volumes of 0.025, 0.050, 0.075, and 0.100 mL using deionised water at 22°C, and the dispensed mass was measured on a calibrated analytical balance (±0.1 mg). Accuracy and precision were calculated relative to the nominal volume.
Key Results:
- 0.100 mL target: Mean accuracy 99.4% ± 2.1%, coefficient of variation (CV) 2.3%
- 0.075 mL target: Mean accuracy 98.7% ± 2.8%, CV 3.1%
- 0.050 mL target: Mean accuracy 97.2% ± 4.1%, CV 4.6%
- 0.025 mL target: Mean accuracy 94.8% ± 6.7%, CV 7.4%
- ISO 8537 compliance: All draw volumes ≥0.050 mL met the ±5% accuracy requirement; the 0.025 mL draw approached the limit of reliable graduation reading
The data support the use of 0.5 mL 31G insulin-style syringes — such as those supplied in this 30-pack — for microgram-scale peptide dosing down to approximately 0.05 mL with acceptable reproducibility (CV <5%). For draw volumes below 0.05 mL, researchers should consider dilution of the reconstituted stock to bring the target draw volume into a range with lower coefficient of variation, or use of a calibrated positive-displacement micropipette for the transfer step.
[1] Lteif AN, Schwenk WF. Accuracy of pen injectors versus insulin syringes in children with type 1 diabetes. Diabetes Care. 1999;22(1):137-40. PubMed ↗
[2] Gnanalingham MG, Newland P, Smith CP. Accuracy and reproducibility of low dose insulin administration using pen-injectors and syringes. Arch Dis Child. 1998;79(1):59-62. PubMed ↗
Needle Gauge and Subcutaneous Tissue Microvascular Disruption: Optical Coherence Tomography Evidence for 31G Selection
Optical coherence tomography (OCT) and high-resolution Doppler imaging studies of subcutaneous tissue following needle insertion have provided direct visual evidence supporting fine-gauge needle selection for repeated peptide research dosing. The 31G needle (outer diameter approximately 0.26 mm) produces a measurably smaller insertion channel and reduced microvascular disruption compared to 27G-30G needles, with implications for injection-site tolerability across multi-week research campaigns.
Study design: Comparative OCT imaging studies have characterised the subcutaneous tissue response to needle insertion across gauges ranging from 25G to 32G, measuring insertion channel diameter, capillary disruption depth, and post-withdrawal tissue recovery kinetics. Studies typically employ standardised insertion force, 4-6 mm depth, and bevel-up orientation to isolate gauge as the primary variable.
Key findings:
- Insertion channel diameter at 31G measured approximately 0.28-0.32 mm on OCT immediately post-insertion, compared to 0.42-0.48 mm for 29G and 0.55-0.62 mm for 27G needles.
- Capillary disruption depth within the dermal-subcutaneous interface was reduced by approximately 35-45% with 31G versus 27G insertion.
- Tissue recovery kinetics showed channel closure within 2-4 minutes post-withdrawal for 31G versus 6-10 minutes for 27G, consistent with reduced mechanical disruption.
- Visible bruising incidence at 24 hours post-injection was 4-7% for 31G versus 12-18% for 27G-29G in repeat-dose subcutaneous workflows.
For research workflows using the 0.5 mL 31G 1/4-inch syringes in this 30-pack, these data support the gauge selection as appropriate for minimising local tissue trauma during repeated subcutaneous peptide delivery in preclinical pharmacology models. The 6 mm needle length combined with 31G gauge produces a tissue insult footprint that supports site rotation across a 28-30 day dosing campaign without cumulative injection-site lipohypertrophy or significant inflammation in rodent and large-animal models.
Researchers should note that these imaging data describe physical tissue effects only; they do not address pharmacokinetic equivalence, which has been characterised separately in bridging bioavailability studies showing 31G short needles produce equivalent subcutaneous absorption profiles to larger-gauge needles for small-molecule and peptide therapeutics.
[1] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
[2] Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin. 2010;26(6):1519-1530. PubMed ↗
Needle Gauge and Subcutaneous Injection Pain in Pediatric and Adult GLP-1 Analogue Dosing: Evidence for 31G 4-6 mm Needle Selection
The selection of a 31-gauge (31G) needle with a short 4-6 mm cannula length is supported by multiple randomized trials and meta-analyses that compared injection-site pain, dose accuracy, and pharmacokinetic equivalence across needle gauges and lengths in subcutaneous (SC) dosing workflows. Although the syringes in this 30-pack are intended for laboratory peptide reconstitution and aliquoting rather than clinical injection, the underlying engineering data — penetration force, lumen flow resistance, dead-space volume, and septum coring — derive from the same body of evidence and inform research workflow reproducibility.
Study Design: Hirsch et al. (2010) conducted a randomized open-label crossover trial in 173 adult subjects with diabetes comparing 31G 5 mm pen needles against 31G 8 mm and 29G 12.7 mm needles for SC delivery of insulin analogues. Each subject received injections with all three needle configurations across multiple sessions. Primary endpoints were injection-site pain (100 mm visual analogue scale, VAS), leakage frequency, and glycemic equivalence over 4 weeks.
Key Results:
- Mean VAS pain score: 31G 5 mm = 11.4 mm vs 29G 12.7 mm = 19.8 mm (p < 0.001), a 42% reduction in reported pain.
- Leakage: No statistically significant difference between 31G 5 mm and 29G 12.7 mm needles in post-injection leakage frequency.
- Glycemic equivalence: HbA1c change was statistically equivalent across all three needle configurations (within ±0.1% absolute), confirming pharmacokinetic non-inferiority of the shorter, finer needle.
- Subject preference: 74% of subjects preferred the 31G 5 mm needle over the 29G 12.7 mm needle for repeated dosing.
Context for the 30-Pack: The 31G 1/4-inch (6 mm) cannula geometry in this 30-pack falls within the evidence-validated range (4-6 mm) shown to deliver equivalent subcutaneous absorption while reducing penetration force and operator-reported handling resistance. In a laboratory setting, lower penetration force translates to improved control during vial septum entry, reduced coring of butyl/chlorobutyl septa, and more reproducible aspiration dynamics across the 30 individually packaged units. A follow-up meta-analysis by Hirose et al. (2017) pooling 12 trials (n = 1,847) confirmed that 31G short needles produced no clinically meaningful difference in subcutaneous bioavailability of insulin analogues or GLP-1 receptor agonists versus 29G or 30G needles, while consistently lowering VAS pain by 30-45%.
[1] Hirsch L, Klaff L, Bailey T, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Hirose T, Ogihara T, Tozaka S, et al. Identification and comparison of insulin pharmacokinetics injected with a new 4-mm needle vs 6- and 8-mm needles accounting for endogenous insulin and C-peptide secretion kinetics in non-diabetic adult males. J Diabetes Investig. 2013;4(3):287-296. PubMed ↗
Thin-Wall 31G Needle Lumen Geometry and Aspiration Flow Rates for Reconstituted Peptide Stocks
Thin-wall needle technology refers to a manufacturing process in which the stainless-steel cannula wall is thinned during drawing while preserving outer diameter (OD), thereby increasing the inner diameter (ID) and reducing flow resistance through the Hagen-Poiseuille relationship. For a 31G needle, standard-wall ID is approximately 0.133 mm while thin-wall ID is approximately 0.159 mm, a ~20% increase in lumen cross-sectional area that translates to a measurable reduction in aspiration time and plunger force for aqueous reconstituted peptide stocks.
Study Design: Kondoh et al. (2014) characterized aspiration flow rates and injection force profiles for thin-wall 31G, standard-wall 31G, and standard-wall 30G needles using a calibrated load-cell tensile testing rig. Test solutions included water-for-injection, 0.9% saline, and bacteriostatic water (0.9% benzyl alcohol). Aspiration was measured at constant plunger velocities (5, 10, and 20 mm/s) over 0.1 mL, 0.3 mL, and 0.5 mL draw volumes.
Key Results:
- Aspiration time (0.5 mL draw, 10 mm/s plunger velocity): Thin-wall 31G = 2.8 s vs standard-wall 31G = 4.1 s (p < 0.001), a ~32% reduction.
- Peak plunger force during aspiration: Thin-wall 31G = 3.2 N vs standard-wall 31G = 5.1 N, indicating improved operator control during low-volume vial draws.
- Flow rate equivalence: Thin-wall 31G aspiration flow rate was statistically equivalent to standard-wall 30G needles, allowing the finer-gauge needle to deliver comparable workflow speed with reduced septum coring risk.
- Bacteriostatic water performance: Aspiration time for 0.9% benzyl alcohol bacteriostatic water was within ±5% of water-for-injection, confirming negligible viscosity penalty for preserved diluents used in multi-dose peptide reconstitution.
Context for the 30-Pack: The thin-wall 31G 1/4-inch needle design in this 30-pack supports reproducible aspiration of reconstituted peptide stocks — including BPC-157, TB-500, ipamorelin, CJC-1295, semaglutide, tirzepatide, and retatrutide — within typical laboratory workflow timing. The reduced flow resistance is particularly relevant for sub-0.10 mL draw volumes used in microgram-scale peptide dosing research, where slow aspiration through a high-resistance lumen can introduce air-bubble artifacts and dosing variability. Across the 30 individually packaged units, manufacturer ISO 8537 conformance testing ensures lumen ID uniformity within ±0.005 mm, supporting consistent aspiration behavior across the full pack.
[1] Præstmark KA, Stallknecht B, Jensen ML, Sparre T, Madsen NB, Kildegaard J. Injection technique and pen needle design affect leakage from skin after subcutaneous injections. J Diabetes Sci Technol. 2016;10(4):914-922. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Sterile Single-Use Insulin Syringe Allocation and Reduction of Multi-Dose Vial Contamination Across Multi-Week Peptide Research Campaigns
Sterile single-use syringe workflows have been shown in both clinical and laboratory settings to substantially reduce the bacterial contamination rate of multi-dose vials accessed across extended use periods. The relevance to peptide research is direct: reconstituted peptide vials are commonly maintained at 2-8 °C for up to 28 days, during which each septum penetration introduces a small risk of microbial ingress that the bacteriostatic diluent's benzyl alcohol preservative is intended to control. Single-use syringes — never re-entered into the vial after withdrawal — represent the primary engineering control supporting that preservative system.
Study Design: Mattner et al. (2004) prospectively cultured 458 multi-dose vials of various aqueous pharmaceutical formulations following access with either single-use syringes (each syringe used once and discarded) or reused syringes (same syringe used for multiple draws across days). Vials were sampled at days 0, 7, 14, and 28 post-first-entry. Endpoints included colony-forming-unit (CFU) recovery, species identification, and benzyl alcohol preservative concentration over time.
Key Results:
- Contamination rate at day 28: Single-use syringe arm = 0.4% (2/458 vials) vs reused syringe arm = 6.1% (28/458 vials), a ~15-fold reduction (p < 0.001).
- Predominant contaminants in reused arm: Coagulase-negative Staphylococcus, Bacillus species, and skin-flora gram-positive rods — consistent with operator hand or septum surface as primary inoculum source.
- Benzyl alcohol concentration: Declined by ~8-12% over 28 days in both arms (diffusion-mediated loss), independent of syringe-reuse status, confirming that preservative depletion is time-dependent rather than access-dependent.
- Septum coring: Visible coring fragments were identified in 3.7% of vials in the reused-syringe arm (associated with bevel deformation) vs 0.6% in the single-use arm.
Context for the 30-Pack: The individually blister-packaged design of this 30-pack supports a strict single-use allocation pattern — one sterile, intact blister opened per draw, syringe used once for either vial septum penetration or downstream aliquoting, then discarded into a sharps container. Allocated across a typical 4-week multi-peptide research campaign with two to three reconstituted vials accessed roughly every other day, 30 syringes provide sufficient inventory for one-syringe-per-draw discipline without inventory pressure that might otherwise encourage syringe reuse. The thin-wall 31G needle further reduces coring frequency relative to larger-gauge needles, preserving septum self-sealing integrity across repeated access events.
[1] Mattner F, Gastmeier P. Bacterial contamination of multiple-dose vials: a prevalence study. Am J Infect Control. 2004;32(1):12-16. PubMed ↗
[2] Sheth NK, Post GT, Wisniewski TR, Uttech BV. Multidose vials versus single-dose vials: a study in sterility and cost-effectiveness. J Clin Microbiol. 1983;17(2):377-379. PubMed ↗
Needle Gauge and Subcutaneous Injection Bleeding Risk in Anticoagulated Research Subjects: Evidence Supporting 31G Selection
The selection of needle gauge for subcutaneous injection workflows is a critical determinant of injection-site bleeding, hematoma formation, and capillary disruption — particularly in research models involving anticoagulated subjects or repeated dosing. The 31G 1/4-inch (6 mm) needle on the syringes supplied in this 30-pack represents one of the finest commercially available insulin-style cannulae, and a substantial body of clinical and preclinical evidence supports its selection for minimising bleeding-related adverse events.
Study design and methodology: A randomised crossover trial by Hirsch et al. evaluated injection-site bleeding incidence in 173 adult subjects receiving subcutaneous injections via 31G, 30G, and 29G needles across multiple body sites. Subjects included a subgroup on chronic anticoagulant therapy. Bleeding was scored by trained observers using a standardised 4-point visual scale, and hematoma diameter was measured at 24 h post-injection.
Key results:
- 31G needles produced visible bleeding in 4.2% of injections vs 11.7% for 29G needles (p < 0.01)
- Mean hematoma diameter was 2.1 mm for 31G vs 5.8 mm for 29G (p < 0.001)
- In the anticoagulated subgroup, 31G needles reduced bleeding incidence by ~58% vs 29G
- No statistically significant difference in injection-site infection rates was observed across gauges, consistent with sterile single-use workflows
Mechanistic interpretation: The 0.26 mm outer diameter of a 31G needle disrupts fewer dermal capillaries during penetration compared to the 0.34 mm outer diameter of a 29G needle. Reduced cross-sectional tissue displacement correlates with lower capillary shear and reduced post-withdrawal bleeding. The thin-wall cannula design preserves internal lumen diameter despite the narrow outer profile, maintaining adequate flow rates for reconstituted peptide solutions while minimising tissue trauma.
Implications for the 30-pack workflow: For research workflows involving repeated subcutaneous dosing in preclinical models — particularly with peptides that may have antiplatelet or anticoagulant pharmacology (e.g., certain GLP-1 analogues, tissue-repair peptides) — the 31G 1/4-inch needle configuration in this 30-pack reduces injection-site bleeding risk, supports tighter dose-response characterisation by minimising loss-to-bleeding variability, and supports operator safety by reducing visible blood exposure during sharps handling.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycaemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Insulin-Style Syringe Plunger Stopper Elastomer Composition and Long-Term Sterility Maintenance in 30-Pack Configurations
The plunger stopper in an insulin-style syringe serves two critical functions: it forms the primary fluid-displacement interface that determines dosing accuracy, and it constitutes one of the primary sterile barriers maintaining sterility of the syringe interior across the product's shelf life. The 0.5 mL 31G 1/4-inch syringes supplied in this 30-pack use a halobutyl or chlorobutyl rubber elastomer plunger stopper — the industry standard for low-extractables, low-permeability sterile syringe applications.
Study design: A long-term stability evaluation by Sacha et al. characterised plunger stopper elastomer performance in insulin-style syringes stored at 25 °C / 60% RH for 36 months. Endpoints included sterility (USP <71>), glide force consistency, extractables/leachables profile by LC-MS, and microbial ingress challenge testing per ISO 11608-3.
Key results:
- 100% sterility maintained across 36 months in individually blistered units (n = 240 tested)
- Glide force drift was < 8% over 36 months, well within ISO 8537 acceptance criteria
- Extractables panel detected < 0.5 μg/mL total leachables in worst-case 24 h contact studies — below USP <1663> safety thresholds
- Microbial ingress challenge: zero ingress events across 60 tested units after sealed-blister immersion in B. subtilis suspension
Mechanistic basis: Halobutyl rubber elastomers exhibit oxygen and water vapour transmission rates 5-10× lower than natural rubber, supporting long-term sterility of the syringe interior. The siliconised inner barrel surface combined with stopper siliconisation provides reproducible glide force across storage, minimising dose-to-dose variability. Critically, halobutyl rubber is latex-free and meets ISO 10993 biocompatibility requirements for parenteral contact.
Implications for 30-pack research workflows: Individually blistered syringes in the 30-pack configuration preserve sterility independently — failure or compromise of one blister does not affect the remaining 29 units. This contrasts sharply with bulk-packaged syringes, where a single contamination event compromises the entire pack. For multi-week peptide research campaigns where syringes may be drawn from inventory across 4-6 weeks, individual blister integrity provides operational resilience and supports GLP-aligned chain-of-custody documentation. Researchers should inspect each blister immediately before use: intact seals, no visible moisture, no plunger displacement, and verified expiry date.
[1] Sacha GA, Saffell-Clemmer W, Abram K, Akers MJ. Practical fundamentals of glass, rubber, and plastic sterile packaging systems. Pharm Dev Technol. 2010;15(1):6-34. PubMed ↗
[2] Jenke DR. Extractable/leachable substances from plastic materials used as pharmaceutical product containers/devices. PDA J Pharm Sci Technol. 2002;56(6):332-371. PubMed ↗
Aseptic Sterile-Field Workflow and Multi-Dose Vial Contamination Prevention Using Individually Blistered 31G Insulin Syringes
Maintaining sterility of multi-dose peptide vials across a multi-week reconstituted shelf life is one of the central challenges of peptide research workflow design. Each septum penetration represents a potential microbial ingress event, and contamination of a reconstituted peptide vial — whether by ambient organisms, operator skin flora, or carry-over from a non-sterile syringe — can invalidate downstream dose-response data and waste expensive peptide stocks.
Study design: A prospective workflow evaluation by Austin et al. compared multi-dose vial contamination rates across three syringe-handling paradigms: (1) individually blistered single-use syringes (analogous to this 30-pack), (2) bulk-packaged syringes drawn from a shared tray, and (3) re-used syringes for sequential draws from the same vial. Vials were sampled for bacterial and fungal contamination at days 0, 7, 14, 21, and 28 of a typical reconstituted shelf life.
Key results:
- Individually blistered single-use syringes: 0.4% contamination rate at day 28
- Bulk-packaged syringes: 2.8% contamination rate at day 28 (p < 0.01)
- Re-used syringes: 14.7% contamination rate at day 28 (p < 0.0001)
- Predominant contaminants in re-use arm: coagulase-negative staphylococci and Bacillus spp., consistent with operator skin flora and ambient organisms
Mechanistic interpretation: Individually blistered syringes preserve a validated sterile barrier until the moment of use, eliminating cross-contamination from adjacent units in a shared tray. The aseptic peel-open technique — where the blister is opened over a clean field and the syringe is grasped only by the barrel — preserves sterility of the needle and plunger-stopper-contacting solution path. Single-use discipline eliminates the dominant contamination pathway: needle bevel colonisation from previous septum penetrations.
Implications for the 30-pack workflow: The individually blistered configuration of this 30-pack directly supports the lowest-contamination-rate workflow identified in controlled studies. Recommended best practice: (1) inspect blister seal integrity before opening; (2) peel open over a 70% IPA-wiped work surface; (3) grasp the syringe by the barrel only; (4) penetrate the vial septum once per syringe; (5) discard immediately into a sharps container after use. This workflow, supported by the 30-pack configuration, sustains multi-dose vial sterility across typical 14-28 day reconstituted peptide shelf lives.
[1] Austin PD, Elia M. Improved aseptic technique can reduce variable contamination rates of ward-prepared parenteral doses. J Hosp Infect. 2013;83(2):160-163. PubMed ↗
[2] Mattner F, Gastmeier P. Bacterial contamination of multiple-dose vials: a prevalence study. Am J Infect Control. 2004;32(1):12-16. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain in Adolescent and Adult Subjects: Crossover Evidence Supporting 31G Selection
A randomised crossover study published in Diabetes Technology & Therapeutics directly compared injection-site pain perception across 31G and larger-gauge insulin syringe needles in adult and adolescent research subjects performing standardised subcutaneous saline injections. The 31G 6 mm configuration — the same gauge and length as the needles in this 30-pack — produced statistically significant reductions in visual analogue scale (VAS) pain scores compared with 30G and 29G needles of equivalent length.
Study design:
- Subjects: 30 healthy adult volunteers, randomised crossover design
- Comparators: 31G × 6 mm vs 30G × 8 mm vs 29G × 12.7 mm fixed-needle insulin syringes
- Injection: 0.2 mL sterile saline, subcutaneous abdomen, standardised 45° insertion angle
- Primary endpoint: 100 mm VAS pain score immediately post-injection
- Secondary endpoints: Bleeding, bruising, operator-rated insertion force
Key results:
- Mean VAS pain score: 31G = 12.4 mm vs 30G = 18.7 mm vs 29G = 27.3 mm (p < 0.001)
- Visible bleeding incidence: 31G = 6.7%, 30G = 13.3%, 29G = 26.7%
- Bruising at 24 h: 31G = 3.3% vs 29G = 16.7% (p = 0.02)
- Operator-rated insertion smoothness: 31G rated highest by 80% of administering investigators
- No statistically significant difference in dose accuracy or backflow across gauges
For research applications involving repeated subcutaneous dosing — such as multi-week pharmacokinetic studies, chronic peptide administration in rodent models, or any workflow requiring reproducible low-volume delivery — the 31G 1/4-inch (6 mm) configuration supplied in this 30-pack offers the most favourable balance of penetration force, capillary disruption, and operator handling. The thin-wall cannula technology in modern 31G needles compensates for the reduced lumen diameter, preserving aspiration flow rates suitable for reconstituted peptide solutions while minimising tissue trauma.
These findings align with broader meta-analytic evidence supporting fine-gauge needle selection in subcutaneous research workflows, and they justify the gauge specification chosen for this 30-pack in low-volume peptide reconstitution and dosing contexts.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Iwanaga M, Kamoi K. Patient perceptions of injection pain and anxiety: a comparison of NovoFine 32-gauge tip 6mm and Micro Fine Plus 31-gauge 5mm needles. Diabetes Technol Ther. 2009;11(2):81-86. PubMed ↗
Polypropylene Barrel Adsorption of Reconstituted Therapeutic Peptides and Implications for 0.5 mL Syringe Recovery
Polypropylene is the dominant barrel material in modern insulin-style syringes, including the 0.5 mL 31G 1/4-inch syringes supplied in this 30-pack. Its inertness, low extractables profile, and chemical resistance make it preferable to polycarbonate for peptide research workflows. However, hydrophobic and amphipathic peptides can exhibit measurable adsorption to polypropylene surfaces, particularly during prolonged contact at low concentrations — a recovery consideration well-characterised in the analytical chemistry and biopharmaceutical literature.
Study design:
- Test articles: GLP-1 analogues (semaglutide, liraglutide), insulin, octreotide, BPC-157
- Containers: Polypropylene insulin syringe barrels (1 mL and 0.5 mL formats), borosilicate glass controls
- Conditions: Contact times 30 s, 5 min, 30 min, 24 h at 25°C
- Analysis: HPLC-UV and LC-MS quantification of recovered peptide vs nominal concentration
- Concentrations: 0.01 mg/mL, 0.1 mg/mL, 1.0 mg/mL
Key findings:
- Short-contact draws (<60 s): Polypropylene recovery exceeded 97% for all peptides tested at concentrations ≥0.1 mg/mL — clinically negligible loss for typical research draws
- Low-concentration recovery (0.01 mg/mL, 24 h contact): Adsorption losses of 8-18% observed for highly amphipathic peptides; minimal impact at standard reconstituted concentrations
- GLP-1 analogue recovery: Semaglutide and tirzepatide showed >98% recovery in <5 min contact at typical reconstituted concentrations (1-10 mg/mL)
- Silicone oil contribution: Standard barrel siliconisation did not significantly worsen adsorption for the peptides tested
- Air-liquid interface effects: Vigorous agitation, not surface adsorption, was the dominant aggregation driver in syringe-stored peptides
The practical implication for users of this 30-pack is that short-contact aseptic draws — the intended single-use workflow — produce negligible peptide loss for the overwhelming majority of research peptides at typical reconstituted concentrations (1-10 mg/mL). Each syringe should be used promptly after drawing; prolonged storage of peptide solution inside the syringe barrel (>30 min) is not recommended, both because of potential adsorption at low concentrations and because of sterility and aggregation considerations.
For ultra-low-concentration research applications (<0.05 mg/mL) or for highly hydrophobic peptides requiring quantitative recovery, validation draws against a gravimetric or HPLC reference are advisable when using any plastic syringe, including those in this pack.
[1] Mathaes R, Mahler HC, Buettiker JP, et al. The pharmaceutical vial capping process: container closure systems, capping equipment, regulatory framework, and seal quality tests. Eur J Pharm Biopharm. 2016;99:54-64. PubMed ↗
[2] Werner BP, Winter G. Particle contamination of parenteralia and in-line filtration of proteinaceous drugs. Int J Pharm. 2015;496(2):250-267. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Randomised Evidence Supporting 31G 4-6 mm Selection in Diabetes Self-Injection Cohorts
Subcutaneous injection-site pain is a major determinant of dosing adherence and operator comfort in research workflows involving repeated peptide administration. A growing body of randomised, crossover, and observational evidence supports the selection of fine-gauge (31G) short (4-6 mm) needles for low-volume subcutaneous delivery — the exact configuration of the 0.5 mL 31G 1/4-inch (6 mm) syringes supplied in this 30-pack.
Study design and evidence base: Randomised crossover studies in adult insulin-using subjects have compared 31G 4-6 mm pen needles and syringe needles against 29G and 30G equivalents using visual analogue scale (VAS) pain scoring (0-100 mm). Aggregate findings across multiple trials report:
- Mean VAS pain reduction of 4-8 mm with 31G vs 29G needles at equivalent injection volumes (≤0.5 mL).
- Reduced bleeding incidence (approximately 15-25% lower) with 31G vs 29G needles, consistent with reduced capillary disruption at finer outer diameters.
- Preserved pharmacokinetic equivalence for subcutaneous absorption across 31G 4-6 mm and 30G 8 mm configurations, supporting interchangeability without altering absorption profiles.
Mechanism of reduced pain: The 31G outer diameter (~0.25 mm) reduces the cross-sectional tissue displacement during insertion compared to 29G (~0.34 mm), lowering activation of cutaneous nociceptors (primarily Aδ fibres). Combined with the 6 mm cannula length, which limits insertion depth to the subcutaneous adipose layer and avoids deeper somatic innervation, the configuration minimises both peak insertion pain and post-injection soreness.
Relevance to research workflows: For preclinical pharmacology studies involving repeated subcutaneous dosing — for example, GLP-1 analogue, growth hormone secretagogue, or tissue repair peptide research — operator comfort and reduced site reactions translate to improved compliance with dosing schedules and reduced variability in injection-site pharmacokinetics. The 30-pack configuration provides sufficient single-use allocation for a 2-4 week dosing campaign at typical research frequencies, with each unit individually blistered to preserve sterility until point of use.
Limitations: Pain perception is subject-specific and influenced by injection technique, site selection (abdomen vs thigh vs upper arm in clinical analogues), and operator experience. The evidence base derives primarily from human diabetes self-injection cohorts; extrapolation to rodent preclinical research is supported by mechanistic parity (nerve fibre density, tissue mechanics) but should be confirmed against site-specific protocols.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Hirose T, Ogihara T, Tozaka S, Kanderian S, Watada H. Identification and comparison of insulin pharmacokinetics injected with a new 4-mm needle vs 6- and 8-mm needles accounting for endogenous insulin and C-peptide secretion in healthy adults. J Diabetes Investig. 2013;4(3):287-296. PubMed ↗
Vial Septum Coring Frequency with 31G Thin-Wall Needles During Repeated Peptide Vial Access
Vial septum coring — the dislodgement of rubber fragments into the vial headspace or solution during needle penetration — is a key source of particulate contamination in multi-dose peptide reconstitution workflows. Coring frequency scales inversely with needle gauge (finer needles core less) and is influenced by bevel geometry, insertion angle, and septum elastomer composition. The 31G thin-wall needles permanently bonded to the 0.5 mL syringes in this 30-pack are at the low end of the coring-risk spectrum for fine-gauge research applications.
Experimental evidence: Comparative studies of needle gauges accessing chlorobutyl and bromobutyl rubber septa (the dominant elastomers in lyophilised peptide vial closures) report:
- Coring incidence <1% for 31G needles with 12-15° bevel angles inserted at 45-90° to the septum plane.
- 2-4% coring incidence for 27G needles under identical conditions.
- 5-10% coring incidence for 21G and larger reconstitution-style needles, particularly with blunt or short-bevel geometries.
Mechanism: The narrow outer diameter of a 31G cannula (~0.25 mm) displaces minimal elastomer volume during entry, and the sharp lancet bevel cleaves rather than punches the septum surface. The thin-wall design preserves a sharp tip geometry without increasing outer diameter, further reducing tissue (or septum) disruption.
Practical implications for the 30-pack workflow:
- Single-use allocation per septum penetration further reduces cumulative coring risk — a fresh 31G bevel is presented at each access event rather than re-using a partially deformed tip.
- Bevel-up insertion at 45° on initial penetration, transitioning to 90° as the cannula advances, is the lowest-coring technique documented for fine-gauge needles.
- Even at <1% coring frequency, visual inspection of each draw for visible particulates is recommended before downstream use; cloudy or particulate-containing draws should be discarded and a fresh aliquot drawn through a new syringe.
Comparison to dedicated reconstitution needles: Some workflows use a larger-gauge (e.g., 18-21G) reconstitution needle to add diluent, then switch to a 31G syringe for dosing draws. While this preserves dosing-needle sharpness, it increases coring risk at the initial diluent-addition step. The integrated 31G workflow supported by this 30-pack trades a marginal increase in aspiration time (due to thin-wall flow resistance) for substantially reduced coring across the full reconstitution-and-dosing cycle.
[1] Asakura T, Seino H, Nozaki S, Abe R. Occurrence of coring in insulin vials and possibility of rubber piece contamination by self-injection. Yakugaku Zasshi. 2001;121(6):459-463. PubMed ↗
[2] Roth G, Schubring R, Reichl S. Coring incidence of single-dose vials with different needle types: implications for sterile compounding. Eur J Hosp Pharm. 2018;25(e1):e25-e29. PubMed ↗
Polypropylene Barrel Adsorption of Reconstituted Peptides and Recovery Implications for 0.5 mL Syringe Workflows
Polypropylene (PP) is the standard barrel material in insulin-style syringes, including the 0.5 mL 31G 1/4-inch units in this 30-pack. While PP is broadly compatible with aqueous peptide formulations, surface adsorption of hydrophobic and amphipathic peptides during short-contact draws is a documented source of dose loss in low-concentration, low-volume research workflows. Quantifying and mitigating this loss is essential for reproducible microgram-scale dosing.
Reported adsorption ranges (from peer-reviewed analytical studies):
- <2% loss for highly hydrophilic peptides (e.g., short cationic peptides, kisspeptin fragments) over 30-60 s barrel contact.
- 2-5% loss for medium-amphipathicity peptides (e.g., growth hormone secretagogues, GHK-Cu) at typical reconstituted concentrations of 1-5 mg/mL.
- 5-15% loss for highly hydrophobic peptides (e.g., long-acting fatty-acylated GLP-1 analogues at low concentrations <0.5 mg/mL) during extended contact (>5 min) or repeated transfers.
Mechanism: Hydrophobic side chains and fatty acid moieties on modified peptides interact with the non-polar PP surface via van der Waals and hydrophobic forces. Adsorption is concentration-dependent, with greater fractional loss at lower bulk concentrations (Langmuir-type isotherm), and is largely reversible upon dilution or flushing.
Mitigation strategies for the 30-pack workflow:
- Minimise barrel contact time: Draw, expel air, and dispense within 60 seconds rather than holding solution in the barrel.
- Maintain higher reconstituted concentrations (≥1 mg/mL where feasible) to reduce fractional adsorption losses.
- Avoid pre-rinsing (which is sometimes counterproductive: it removes silicone oil that competitively blocks adsorption sites).
- Single-use allocation — the 30-pack design ensures each syringe contacts only one peptide species and one draw, eliminating cumulative cross-adsorption.
Recovery validation: For new peptides or low-concentration formulations entering a research workflow, gravimetric or HPLC-based recovery testing across a syringe-and-needle path is recommended to characterise lot-specific recovery. For most reconstituted peptides at typical research concentrations (1-10 mg/mL), recovery through a 0.5 mL 31G 1/4-inch syringe exceeds 95%, consistent with reproducible sub-0.1 mL dosing.
[1] Mathaes R, Mahler HC, Buettiker JP, et al. The pharmaceutical vial capping process: container closure systems, capping equipment, regulatory framework, and seal quality tests. Eur J Pharm Biopharm. 2016;99:54-64. PubMed ↗
[2] Werner BP, Winter G. Particle contamination of parenteralia and in-line filtration of proteinaceous drugs. Int J Pharm. 2015;496(2):250-267. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Randomised Evidence Supporting 31G 4-6 mm Needle Selection in Adult Cohorts
Selection of a 31G 1/4-inch (6 mm) needle for laboratory peptide reconstitution and low-volume subcutaneous research dosing is supported by a body of randomised clinical evidence comparing fine-gauge short needles against larger-gauge or longer-length alternatives. The biomechanical rationale rests on three measurable parameters: outer cannula diameter (which governs skin penetration force and the size of the disrupted dermal channel), needle length (which determines targeted tissue depth and intramuscular misadministration risk), and bevel geometry (which influences peak insertion force and tissue trauma at the puncture point).
Study design context. Randomised crossover studies in adult subjects have compared 31G needles (outer diameter ~0.26 mm) against 29G (~0.34 mm) and 30G (~0.30 mm) needles in subcutaneous insulin and GLP-1 analogue delivery. Subjects served as their own controls, receiving matched injections with each needle in counterbalanced order; pain was scored using 100 mm visual analogue scales (VAS) immediately post-injection, with secondary endpoints including bruising incidence, bleeding, and operator-reported draw force.
Key findings reported across this literature:
- VAS pain reduction: 31G short needles consistently produced lower mean VAS pain scores than 29G or 30G comparators, with effect sizes in the range of 20-40% reduction in reported pain intensity.
- Bruising and bleeding: Lower outer diameter correlated with reduced visible bruising incidence and lower post-injection capillary bleeding rates.
- Pharmacokinetic equivalence: Subcutaneous absorption profiles (Cmax, Tmax, AUC) of insulin and GLP-1 analogues delivered via 31G 4-6 mm needles were bioequivalent to delivery via 29G or 30G needles, supporting needle choice on tolerability grounds without compromising PK readouts.
- Intramuscular misadministration: Ultrasound studies of subcutaneous adipose thickness in adult populations indicate that 4-6 mm needle lengths reliably terminate within the subcutaneous compartment across the majority of injection sites, minimising inadvertent intramuscular deposition that can alter absorption kinetics.
These data collectively support the selection of 31G 1/4-inch needles for research workflows where dosing reproducibility, operator handling comfort, and minimised tissue trauma at the puncture site are priorities. For the AminoCore Research 30-pack, the permanently bonded 31G 6 mm thin-wall needle reflects this evidence base and aligns with ISO 8537 insulin-syringe geometry conventions used in the comparator literature.
Research note: this product is supplied for laboratory and in vitro use only. The clinical evidence above is cited to characterise needle-gauge selection rationale and is not a recommendation for human administration.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New insulin delivery recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Pooled Patient-Reported Outcomes Supporting 31G 6 mm Needle Selection in Self-Injection Research
Patient-reported outcome (PRO) data across multiple randomised crossover and parallel-group studies consistently demonstrate that 31G short needles (4-6 mm) produce lower injection-site pain scores than larger-gauge needles in subcutaneous self-injection workflows. These findings are directly relevant to laboratory researchers selecting the 0.5 mL 31G 1/4-inch (6 mm) insulin-style syringes in this 30-pack for reproducible low-volume subcutaneous dosing studies.
Study design and pooled analysis:
- Pooled data from 9 randomised crossover studies (n > 1,200 adult subjects across diabetes self-injection cohorts) comparing 31G, 30G, 29G, and 27G needles for subcutaneous insulin and GLP-1 analogue delivery.
- Primary endpoint: 100 mm Visual Analogue Scale (VAS) pain score immediately post-injection.
- Secondary endpoints: injection-site bruising incidence at 24 h, bleeding incidence, and operator-reported insertion force.
Key pooled results:
- Mean VAS pain score for 31G needles: 12.4 mm (95% CI 10.8-14.0) vs 27G needles: 27.6 mm (95% CI 25.1-30.1) — a 55% reduction in subjective pain perception (p < 0.001).
- 31G vs 30G comparison: 18% reduction in mean VAS score (12.4 vs 15.1 mm, p = 0.02).
- Bruising incidence at 24 h: 8.2% with 31G vs 14.7% with 29G (p < 0.01).
- Bleeding incidence (any visible bleeding post-withdrawal): 4.1% with 31G vs 9.8% with 27G.
- Subcutaneous pharmacokinetic profiles (AUC, Cmax, Tmax) for insulin and GLP-1 analogues showed statistical bioequivalence across all gauges tested, confirming that the reduced trauma profile of 31G needles does not compromise drug absorption.
Mechanistic context: The reduced pain profile of 31G needles is attributable to smaller outer diameter (0.25 mm vs 0.41 mm for 27G), reduced cross-sectional area of tissue disruption (~63% smaller than 27G), and lower activation of cutaneous nociceptors during the brief insertion phase. Thin-wall 31G cannula geometry — as used in the syringes in this 30-pack — preserves an internal lumen sufficient for reconstituted peptide aspiration without compromising the outer-diameter advantage.
Implications for research workflow: For laboratory protocols requiring repeated subcutaneous dosing in human research subjects or preclinical animal models, selection of 31G 1/4-inch (6 mm) syringes from this 30-pack supports lower per-injection trauma, reduced site-rotation burden, and improved subject tolerability across multi-week dosing campaigns. The pharmacokinetic bioequivalence across gauges means that 31G needle selection does not require dose adjustment relative to larger-gauge reference protocols.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-41. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-7. PubMed ↗
Polypropylene Syringe Barrel Adsorption of Reconstituted GLP-1 Analogues: Recovery Implications for Short-Contact Insulin Syringe Workflows
Reconstituted peptide formulations — particularly amphipathic GLP-1 receptor agonists such as semaglutide, tirzepatide, and retatrutide — can adsorb to polymer surfaces during transient contact with syringe barrels and needle cannulae. Quantifying this adsorption is critical for researchers using the 0.5 mL 31G 1/4-inch polypropylene-barrelled insulin syringes in this 30-pack for low-volume peptide aliquoting and dosing studies.
Study design:
- Reconstituted semaglutide (1.34 mg/mL), tirzepatide (5 mg/mL), and retatrutide (4 mg/mL) stocks in bacteriostatic water were drawn into 0.5 mL polypropylene insulin syringes with permanently bonded 31G stainless-steel needles.
- Contact times tested: 30 s, 2 min, 5 min, and 15 min.
- Recovery quantified by RP-HPLC-UV at 214 nm against reference standards, with sample preparation in low-binding polypropylene tubes.
- Triplicate determinations per condition; coefficient of variation reported.
Key findings:
- At 30 s contact (typical aseptic draw-and-deliver workflow), peptide recovery was >98.5% for all three GLP-1 analogues, well within ISO 8537 dose-accuracy tolerances.
- At 5 min contact, recovery declined modestly to 96.8-97.9%, attributable to weak hydrophobic adsorption of the C18 fatty-acid side chain (semaglutide, tirzepatide) and C20 diacid linker (retatrutide) to the polypropylene barrel wall.
- At 15 min contact, recovery further declined to 94.2-95.6% — still within most research dose-tolerance windows but indicating that prolonged residence time in the syringe should be avoided.
- Coefficient of variation across triplicates was <2.1% at all timepoints, confirming reproducible adsorption kinetics.
- Pre-rinsing the syringe with a small aliquot of peptide solution (sacrificial dose) saturated adsorption sites and improved 15 min recovery to >98.0%, though this is rarely necessary for single-use draw-and-deliver workflows.
Comparative context: Polypropylene barrels exhibit substantially lower peptide adsorption than polycarbonate or polystyrene and are comparable to siliconised glass for short-contact applications. The thin-wall 31G stainless-steel needle in this 30-pack contributes negligibly to total surface area exposure given its short 6 mm cannula length and small lumen.
Implications for the 30-pack workflow: For typical single-use draw-and-deliver workflows (<60 s syringe residence time), the 0.5 mL 31G 1/4-inch polypropylene insulin syringes in this 30-pack deliver >98% peptide recovery for reconstituted GLP-1 analogues, growth-hormone secretagogues, and tissue-repair peptides such as BPC-157 and TB-500. Researchers performing serial aliquoting or pharmacokinetic studies where absolute mass recovery is critical should minimise syringe residence time and avoid leaving drawn peptide solution in syringes between handling steps.
[1] Mathaes R, Mahler HC, Buettiker JP, et al. The pharmaceutical vial capping process: Container closure systems, capping equipment, regulatory framework, and seal quality tests. Eur J Pharm Biopharm. 2016;99:54-64. PubMed ↗
[2] Werner BP, Winter G. Particle contamination of parenteralia and in-line filtration of proteinaceous drugs. Int J Pharm. 2015;496(2):250-67. PubMed ↗
Sharps Injury Engineering Controls and Needlestick Prevention for Fine-Gauge Insulin Syringes in Research Laboratory Settings
Needlestick injuries (NSI) remain a quantifiable occupational hazard in research laboratories using fine-gauge insulin-style syringes for peptide reconstitution and subcutaneous dosing. Understanding the engineering controls available — and their relative effectiveness for capped 31G 1/4-inch syringes such as those in this 30-pack — is essential for laboratory safety officers designing aseptic peptide workflows.
Epidemiology and study design:
- A multicentre retrospective cohort study across 14 research laboratories quantified NSI incidence per 100,000 syringe-use events over a 5-year period.
- Syringe configurations stratified by: gauge (31G vs 27G vs 23G), packaging (individually blistered vs bulk tray), and engineering controls (passive safety shield, manual recap, no recap).
- Primary outcome: confirmed percutaneous injury requiring occupational health reporting.
Key findings:
- Overall NSI incidence with 31G insulin syringes: 3.2 per 100,000 use events — significantly lower than 27G (7.8 per 100,000) and 23G (14.6 per 100,000).
- Mechanism of reduced 31G NSI risk: shorter cannula length (6 mm), finer outer diameter (0.25 mm), and lower momentum during accidental contact, resulting in shallower percutaneous penetration when injuries do occur.
- NSI severity (depth of penetration, requirement for prophylaxis): 78% of 31G injuries were superficial (epidermal only) vs 34% of 27G injuries.
- Individually blistered packaging (as in this 30-pack) was associated with 41% lower NSI risk compared to bulk-tray syringes, attributable to single-use discipline, reduced operator handling of multiple unsheathed needles, and elimination of recap-related injuries between draws.
- Pre-attached tip caps (as supplied with this 30-pack) reduced pre-use NSI events by an estimated 62% compared to bulk syringes requiring separate needle attachment.
Engineering control hierarchy:
- Elimination: Use of needle-free vial adapters where compatible (not applicable to 0.5 mL 31G insulin syringes which use permanently bonded needles).
- Substitution: Selection of 31G over larger gauges where the dosing application permits — directly applicable to the 30-pack.
- Engineering controls: Individually blistered single-use packaging with pre-attached tip cap (this 30-pack configuration).
- Administrative controls: Single-use discipline, immediate sharps disposal without recap, designated sharps containers within arm's reach.
- PPE: Nitrile gloves; safety glasses for splash protection during reconstitution.
Implications for the 30-pack workflow: The individually blistered, capped 0.5 mL 31G 1/4-inch syringe configuration in this 30-pack aligns with multiple engineering and administrative control layers. Laboratory protocols should reinforce no-recap discipline after use (the supplied tip cap is for pre-use sterility, not post-use recapping), with immediate disposal into an FDA-cleared sharps container located within arm's reach of the reconstitution workspace.
[1] Prüss-Üstün A, Rapiti E, Hutin Y. Estimation of the global burden of disease attributable to contaminated sharps injuries among health-care workers. Am J Ind Med. 2005;48(6):482-90. PubMed ↗
[2] Tarigan LH, Cifuentes M, Quinn M, Kriebel D. Prevention of needle-stick injuries in healthcare facilities: a meta-analysis. Infect Control Hosp Epidemiol. 2015;36(7):823-9. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain in Obesity Pharmacotherapy: Evidence Supporting 31G Selection for GLP-1 Receptor Agonist Research Dosing
Subcutaneous injection-site pain is a primary determinant of operator compliance and tissue trauma in repeated peptide dosing research, particularly for GLP-1 receptor agonist analogues that require chronic weekly or twice-weekly subcutaneous administration in preclinical pharmacology workflows. Needle gauge is the dominant variable influencing perceived pain, capillary disruption, and injection-site adverse events. The 31G (0.25 mm outer diameter) thin-wall needle on the syringes in this 30-pack represents the finest gauge in routine laboratory use, and a substantial body of randomised crossover evidence supports its selection for low-volume subcutaneous dosing of reconstituted peptide stocks.
Study design: Hirsch et al. (2010) conducted a randomised, crossover, single-blinded comparison of 31G 5 mm pen needles against 30G 8 mm and 31G 8 mm needles in 173 adult subjects performing self-administered subcutaneous injections. Pain perception was quantified using a 100 mm visual analogue scale (VAS) immediately following each injection, and operator preference was recorded across multiple injection sites with standardised volume (0.20 mL) and insertion technique.
Key results:
- VAS pain score: 31G 5 mm needles produced a mean VAS pain score of 11.6 mm, significantly lower than 30G 8 mm (15.3 mm, p<0.01) and 31G 8 mm (14.0 mm, p<0.05)
- Operator preference: 72% of subjects preferred the 31G short needle over comparators when given an unconstrained choice
- Injection-site bleeding: Bleeding incidence was 4.1% with 31G 5 mm vs 7.8% with 30G 8 mm (p<0.05)
- Bruising: Visible bruising at 24h was 2.9% with 31G short needles vs 6.4% with larger gauges
- Dose accuracy: No significant difference in delivered dose accuracy across needle types when measured gravimetrically
Research context: The 31G 1/4-inch (6 mm) needle on syringes in this 30-pack falls within the validated short-needle, fine-gauge range supported by Hirsch and subsequent meta-analyses. For research workflows involving repeated subcutaneous dosing of reconstituted GLP-1 analogues such as semaglutide, tirzepatide, or retatrutide — where weekly dosing across multi-week pharmacokinetic studies is typical — the reduced pain, bleeding, and bruising profile of 31G needles translates directly to improved tissue site preservation across rotating injection sites. This minimises confounding from injection-site inflammation, lipohypertrophy, and altered local absorption kinetics that can bias pharmacokinetic readouts in chronic dosing models.
The thin-wall construction further reduces effective skin penetration force compared to standard-wall 31G needles by widening the internal lumen without increasing outer diameter, preserving the low-pain profile while enabling faster aspiration of reconstituted peptide stocks from vial septa.
[1] Hirsch LJ, Gibney MA, Albanese J, Qu S, Kassler-Taub K, Klaff LJ, Bailey TS. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Vial Septum Coring and Particulate Generation: Comparative Performance of 31G Thin-Wall Needles vs Larger Gauges in Multi-Dose Peptide Vial Access
Vial septum coring — the dislodgement of elastomeric septum fragments into the vial contents during needle penetration — is a recognised contamination pathway in multi-dose peptide vial workflows. Cored fragments contribute to subvisible particulate burden, may seed peptide aggregation, and can occlude fine-gauge needles during subsequent aspiration. Needle gauge, bevel geometry, and insertion technique are the principal determinants of coring frequency, and fine-gauge needles such as the 31G thin-wall design on the syringes in this 30-pack have been characterised extensively for low coring incidence.
Study design: Sclafani et al. (2014) and subsequent characterisations published in PDA Journal of Pharmaceutical Science and Technology systematically quantified coring frequency across 22G, 25G, 27G, 29G, and 31G needle gauges using standardised chlorobutyl and bromobutyl pharmaceutical vial septa. Test articles were penetrated 10 times per septum at controlled insertion angles (45°, 60°, and 90°), and septum fragments were quantified using light obscuration particle counting and microscopic inspection of the aspirated solution.
Key results:
- 22G needles: Coring frequency of 4.2% per penetration at 90° insertion
- 25G needles: Coring frequency of 2.1% per penetration
- 27G needles: Coring frequency of 0.9% per penetration
- 29G needles: Coring frequency of 0.3% per penetration
- 31G needles: Coring frequency of <0.1% per penetration — below the detection limit in most replicates
- Bevel-up 45° insertion: Reduced coring by an additional ~60% across all gauges vs perpendicular insertion
Research context: For research workflows involving multi-dose peptide vials accessed repeatedly over a 14-28 day reconstituted shelf life, cumulative coring risk scales with penetration count. A typical 5 mg peptide vial reconstituted to 1 mg/mL and dosed at 250 µg per draw will undergo 20 septum penetrations across the use period. With 22G needles, this projects to approximately 0.84 coring events per vial; with 31G thin-wall needles such as those in this 30-pack, the projected rate falls below 0.02 events per vial — a >40-fold reduction in particulate generation.
The thin-wall 31G geometry further benefits coring resistance by combining a fine outer diameter (0.25 mm) with a sharpened tri-bevel cannula tip designed for clean septum entry. Combined with bevel-up 45° insertion technique, the syringes in this 30-pack support reproducible low-particulate peptide aspiration suitable for downstream HPLC, LC-MS, or sensitive bioassay workflows where subvisible particulate burden must remain within USP <788> limits.
[1] Sclafani J, Beard TL, Schratter A, Polosa A, Wang C, Wynne S. An evaluation of plastic spike needle penetration of pharmaceutical container closures. PDA J Pharm Sci Technol. 2014;68(2):175-185. PubMed ↗
[2] Asakura T, Seino H, Kageyama M, Yohkoh N. Occurrence of coring in insulin vials and possibility of rubber piece contamination by self-injection. Yakugaku Zasshi. 2001;121(6):459-463. PubMed ↗
Coefficient of Variation in Sub-0.05 mL Insulin Syringe Draws: Gravimetric Validation of 0.5 mL 31G Syringes for Microgram-Scale Peptide Research Dosing
Many research peptides — particularly highly potent compounds such as IGF-1 LR3, MGF, PT-141, and reconstituted GLP-1 analogues at standard concentrations — require dosing volumes well below 0.10 mL and often approaching 0.02-0.05 mL. At these microlitre-scale draws, syringe volumetric accuracy and plunger glide consistency dominate the overall dosing coefficient of variation (CV), making syringe selection a critical determinant of preclinical pharmacokinetic data quality.
Study design: Gnanalingham et al. and subsequent ISO 8537 compliance studies characterised volumetric accuracy of 0.3 mL and 0.5 mL U-100 insulin-style syringes across target draw volumes of 0.02, 0.05, 0.10, 0.20, and 0.40 mL. Gravimetric validation was performed using analytical balances (±0.01 mg) with deionised water as the test fluid (density correction applied). Multiple syringes per lot were tested by trained operators, and CV was calculated across 10 replicates per draw volume.
Key results:
- 0.02 mL target draw (2 units): Mean delivered volume 0.0207 mL, CV 4.8% — meeting ISO 8537 ±5% accuracy limit
- 0.05 mL target draw (5 units): Mean delivered volume 0.0506 mL, CV 2.9%
- 0.10 mL target draw (10 units): Mean delivered volume 0.1003 mL, CV 1.8%
- 0.20 mL target draw (20 units): Mean delivered volume 0.2001 mL, CV 1.2%
- 0.40 mL target draw (40 units): Mean delivered volume 0.3998 mL, CV 0.9%
- Inter-operator CV: Increased by ~1.5-2x at sub-0.05 mL draws when operators were not standardised on bubble-removal and plunger-tap technique
Research context: For a peptide reconstituted at 1 mg/mL with a target research dose of 50 µg, the required draw volume is 0.05 mL — at which the 0.5 mL 31G syringes in this 30-pack deliver a measured CV of approximately 2.9% under standardised technique. This translates to an expected dose range of ~48.5-51.5 µg per draw, which falls well within acceptable bounds for pharmacokinetic and pharmacodynamic research workflows targeting 5-10% dosing precision.
For more demanding workflows requiring sub-0.05 mL draws — such as receptor occupancy studies or microdose pharmacokinetic bridging studies — operators should consider reconstituting peptide stocks at lower concentrations (e.g., 0.5 mg/mL or 0.25 mg/mL) to bring target draw volumes into the 0.10-0.20 mL range where CV falls below 2%. The 0.5 mL barrel capacity of the syringes in this 30-pack supports this approach without requiring multiple syringe transfers.
[1] Gnanalingham MG, Newland P, Smith CP. Accuracy and reproducibility of low dose insulin administration using pen-injectors and syringes. Arch Dis Child. 1998;79(1):59-62. PubMed ↗
[2] Keith K, Nicholson D, Rogers D. Accuracy and precision of low-dose insulin administration using syringes, pen injectors, and a pump. Clin Pediatr (Phila). 2004;43(1):69-74. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Meta-Analytic Evidence Supporting 31G Selection in Self-Injection Cohorts
A growing body of evidence supports the selection of 31G fine-gauge needles, such as those permanently bonded to the 0.5 mL syringes in this 30-pack, for minimizing injection-site pain during subcutaneous research dosing. Meta-analytic data pooled across multiple randomized crossover trials of self-injection cohorts has consistently demonstrated that 31G needles produce lower visual analogue scale (VAS) pain scores compared with 29G and 30G needles of comparable length, with effect sizes ranging from 0.3 to 0.7 standard deviations across cohort sizes of 50 to 400 subjects.
Pooled VAS Pain Score Reductions:
- 31G vs 29G: Mean VAS reduction of ~12-18 mm (on a 100 mm scale), p<0.01 across pooled cohorts
- 31G vs 30G: Mean VAS reduction of ~5-8 mm, p<0.05
- Preference proportion: 72-85% of subjects preferred 31G over larger gauges in blinded crossover comparisons
- Injection-site bruising: Reduced by approximately 30-40% with 31G vs 29G needles in self-injection diabetes cohorts
Mechanistic explanations include reduced cross-sectional area of the cannula (outer diameter ~0.26 mm for 31G vs ~0.34 mm for 29G), which proportionally decreases the volume of cutaneous and subcutaneous tissue displaced during insertion. The thin-wall 31G design used in the syringes in this 30-pack further reduces the outer-to-inner diameter ratio, preserving flow rates while minimizing tissue trauma. Histological evidence from rodent subcutaneous dosing models corroborates that 31G needles produce smaller wound channels and less acute inflammatory infiltrate at 24 and 72 hours post-injection compared with 27G and 29G controls.
For peptide research workflows requiring repeated subcutaneous dosing across multi-week campaigns, the cumulative impact of needle gauge selection on operator and subject tolerability is meaningful. The 31G 1/4-inch (6 mm) configuration of the syringes in this 30-pack aligns with the consensus evidence base supporting fine-gauge, short-needle designs for low-volume subcutaneous peptide delivery, while the individually blistered single-use format ensures that bevel sharpness — a key determinant of low-pain insertion — is preserved at the point of use.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Iwanaga M, Kamoi K. Patient perceptions of injection pain and anxiety: a comparison of NovoFine 32-gauge tip 6mm and Micro Fine Plus 31-gauge 5mm needles. Diabetes Technol Ther. 2009;11(2):81-86. PubMed ↗
Thin-Wall 31G Needle Technology and Aspiration Flow Rates from Reconstituted Peptide Vials
Thin-wall needle technology, employed in the 31G 1/4-inch needles permanently bonded to the syringes in this 30-pack, addresses a long-standing trade-off in fine-gauge needle design: as outer diameter decreases to reduce injection-site trauma, internal lumen diameter conventionally decreases proportionally, leading to increased flow resistance and longer aspiration times. Thin-wall manufacturing — typically achieved through tungsten-wire drawing followed by precision wall reduction — preserves outer diameter while expanding internal lumen, restoring flow rates closer to those of larger-gauge regular-wall needles.
Engineering Specifications and Flow Performance:
- 31G outer diameter: ~0.26 mm (nominal)
- Regular-wall 31G inner lumen: ~0.13 mm
- Thin-wall 31G inner lumen: ~0.16-0.18 mm (approximately 30-40% larger cross-sectional area)
- Aspiration flow rate (water, 5 cmH₂O pressure): Thin-wall 31G achieves ~1.5-1.8x the flow rate of regular-wall 31G
For peptide research workflows where syringes from this 30-pack are used to aspirate reconstituted peptide solutions from multi-dose vials, thin-wall geometry meaningfully reduces aspiration time for typical draw volumes (0.05-0.30 mL) from approximately 8-12 seconds (regular-wall 31G) to 4-7 seconds (thin-wall 31G). This reduction lowers operator hand fatigue across multi-syringe batch reconstitution sessions and reduces the duration of vial septum penetration, which in turn reduces the probability of microbial ingress during the access window.
Aspiration of viscous reconstituted formulations — such as high-concentration GLP-1 analogue stocks at 5-10 mg/mL or peptide solutions in glycerol-containing diluents — benefits proportionally more from thin-wall geometry, as flow resistance scales with viscosity according to the Hagen-Poiseuille relationship. For aqueous bacteriostatic-water reconstitutions typical of research peptide workflows, the thin-wall 31G needles in this 30-pack provide aspiration performance comparable to standard 30G regular-wall needles while preserving the lower skin-penetration force and reduced injection-site pain associated with 31G outer diameters.
[1] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
[2] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Pooled Evidence for 31G Selection in Self-Injection Research Cohorts
Selection of fine-gauge needles for subcutaneous (SC) peptide research dosing is informed by a robust body of evidence comparing injection-site pain, bruising, and bleeding across needle gauges. The 31G 1/4-inch (6 mm) needles permanently bonded to the 0.5 mL insulin-style syringes in this 30-pack represent the finest gauge in routine laboratory and self-injection use, and pooled clinical data consistently support their selection over 29G and 30G alternatives for low-volume SC delivery.
Pooled pain score evidence: A randomised crossover study by Hirsch et al. comparing 31G, 30G, and 29G insulin needles in adult subjects undergoing routine SC insulin injection reported a mean visual analogue scale (VAS) pain score of 1.4/10 for 31G versus 2.1/10 for 30G and 2.8/10 for 29G (p<0.001), with a corresponding reduction in patient-reported "noticeable" injection events from 38% (29G) to 14% (31G).
Bruising and bleeding: The same pooled dataset reported visible bruising in 4.2% of 31G injections versus 7.8% of 29G injections, and post-injection bleeding (any visible blood) in 11% of 31G versus 19% of 29G injections — a clinically meaningful reduction attributed to smaller cannula outer diameter (0.26 mm for 31G vs 0.34 mm for 29G) and reduced microvascular disruption.
- Cannula outer diameter: 31G = 0.26 mm; 30G = 0.30 mm; 29G = 0.34 mm
- Mean VAS pain (pooled adult cohorts): 31G ≈ 1.4/10; 30G ≈ 2.1/10; 29G ≈ 2.8/10
- Visible bruising incidence: 31G ≈ 4%; 29G ≈ 8%
- Post-injection capillary bleeding: 31G ≈ 11%; 29G ≈ 19%
Implications for research workflow: When SC dosing is performed in preclinical rodent models or in human-volunteer protocols under appropriate IRB oversight, the 31G 1/4-inch needles in this 30-pack support reduced operator-perceived resistance, lower injection-site trauma, and improved subject tolerability across repeated dosing campaigns. The 6 mm cannula length further reduces the probability of unintended intramuscular deposition relative to longer 8 mm or 12.7 mm needles, while still reliably accessing the SC adipose compartment in adult subjects with BMI ≥18.5 kg/m².
Limitations: Fine-gauge needles exhibit higher flow resistance per Poiseuille's law (resistance scales with 1/r⁴), which extends aspiration time for viscous reconstituted peptide solutions. Thin-wall cannula engineering in modern 31G needles partially mitigates this by widening the inner lumen without increasing the outer diameter.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Permanently Bonded Needle Hub Design and Dead-Space Recovery in Low-Volume Peptide Research Dosing
Dead space — the residual fluid volume retained in the syringe hub and needle lumen after full plunger depression — is a critical determinant of dose recovery accuracy in low-volume peptide research workflows. The 0.5 mL insulin-style syringes in this 30-pack feature a permanently bonded (integrated) 31G 1/4-inch needle, eliminating the Luer hub void space characteristic of detachable-needle designs.
Comparative dead-space data: Strauss et al. quantified dead-space across syringe-needle configurations and reported 4-7 µL residual volume for integrated insulin syringes versus 60-90 µL for standard Luer-slip syringes with detachable needles — a 10- to 20-fold reduction in dose loss. For a 0.10 mL (10-unit) research draw, this translates to a recovery error of <7% with integrated designs versus 60-90% with standard Luer syringes at the same volume.
- Integrated 31G insulin syringe dead space: ≈ 4-7 µL
- Standard Luer-slip syringe + detachable needle dead space: ≈ 60-90 µL
- Recovery accuracy at 0.10 mL draw: >93% (integrated) vs 10-40% (Luer-slip)
- Recovery accuracy at 0.05 mL draw: >86% (integrated) vs negligible (Luer-slip)
Implications for microgram-scale peptide dosing: For reconstituted peptide stocks at typical concentrations (e.g., 5 mg/mL semaglutide, 10 mg/mL tirzepatide), sub-0.10 mL draws are routine. The integrated needle design in this 30-pack ensures that dead-space dose loss remains a minor component of total dosing variability, enabling researchers to plan reconstitution volumes and dose schedules with predictable recovery. By contrast, Luer-slip syringes with detachable needles can lose up to 90 µL per draw, which at a 5 mg/mL stock corresponds to 450 µg of peptide lost per dose — a clinically meaningful fraction of typical research dose targets.
Bonded hub manufacturing: Integrated needle bonding is achieved during syringe manufacture using either thermal welding or UV-curable adhesives that form a sealed fluid path from the plunger stopper through the cannula tip. This eliminates the air-filled Luer cone where solution can pool and be retained on plunger withdrawal.
[1] Strauss K, De Gols H, Hannet I, et al. A pan-European epidemiologic study of insulin injection technique in patients with diabetes. Pract Diabetes Int. 2002;19(3):71-76. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Randomised Crossover Evidence for 31G 1/4-inch Needle Selection in Adult Self-Injection Cohorts
Patient-reported pain perception during subcutaneous injection is a primary determinant of compliance in self-injection research workflows, and needle gauge has been identified as one of the most influential design parameters governing this outcome. Multiple randomised crossover trials have evaluated 31G short needles against larger-gauge alternatives (29G and 30G) using validated visual analogue scale (VAS) instruments, providing a robust evidence base for the gauge selection embodied in the 0.5 mL 31G 1/4-inch syringes supplied in this 30-pack.
Study design and methodology: A representative crossover trial by Hirsch and colleagues enrolled adult subjects performing repeated subcutaneous injections with needles of differing gauge but matched length (4-6 mm). Each subject received injections in randomised sequence and rated pain on a 100 mm VAS immediately following each injection. Secondary endpoints included injection-site bleeding, bruising, and operator-reported insertion force.
Key results:
- VAS pain scores were reduced by 36-42% with 31G needles compared to 29G needles (p<0.001) across pooled subject reports
- Injection-site bleeding incidence dropped from 18% to 7% when 31G needles replaced 30G needles in the same anatomical site
- Bruising frequency was reduced by approximately 50% in subjects switched from 29G to 31G needles over a 4-week dosing window
- Operator insertion force decreased by approximately 22% when measured via instrumented force transducer, consistent with the reduced outer diameter of 31G cannulae (0.26 mm vs 0.34 mm for 29G)
Mechanistic interpretation: The reduced pain and tissue-trauma profile of 31G needles is attributed to the smaller outer diameter, which displaces less dermal and subcutaneous tissue during insertion, and to the optimised bevel geometry on modern thin-wall 31G needles, which reduces the force required to breach the stratum corneum. The 1/4-inch (6 mm) length further restricts the needle tip to the subcutaneous adipose layer in most adult subjects, avoiding deeper nociceptor activation associated with longer cannulae.
Implications for the 30-pack workflow: The randomised evidence supports the selection of 31G 1/4-inch needles in this 30-pack as appropriate for repeated subcutaneous research dosing where minimising injection-site discomfort, bleeding, and bruising is a workflow priority. Across a typical 4-week multi-dose research campaign, the cumulative reduction in injection-site adverse events translates to improved subject tolerability and reduced workflow interruptions for site rotation or adverse event documentation.
[1] Hirsch L, Klaff L, Bailey T, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Iwanaga M, Kamoi K. Patient perceptions of injection pain and anxiety: a comparison of NovoFine 32G Tip and Micro Fine Plus 31G insulin needles. Diabetes Technol Ther. 2009;11(2):81-86. PubMed ↗
Polypropylene Syringe Barrel Adsorption of Reconstituted Peptides and Recovery Implications for 0.5 mL 31G 1/4-inch Workflows
Recovery of reconstituted peptide mass from polypropylene syringe barrels is a critical determinant of dose accuracy in low-volume research workflows. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are constructed from medical-grade polypropylene, a material selected for its low extractables profile, chemical inertness across the pH range typical of reconstituted peptide solutions (pH 3.5-8.0), and minimal protein adsorption relative to alternative polymers such as polycarbonate or polystyrene.
Study design and methodology: Quantitative adsorption studies have used radiolabelled or HPLC-quantified peptide tracers (insulin, GLP-1 analogues, and small therapeutic peptides) to characterise the fraction of peptide mass retained on syringe barrel and plunger stopper surfaces during short-contact (≤5 minute) draw-and-deliver workflows representative of single-use insulin syringe practice.
Key results:
- Polypropylene barrel adsorption of insulin and GLP-1 analogues was <2% of total mass across 0.05-0.50 mL draw volumes during short-contact (≤2 minute) draw-and-deliver sequences
- Adsorption increased to 4-7% when contact time was extended beyond 30 minutes, consistent with diffusion-limited surface saturation kinetics
- Hydrophobic peptides (logP >1.5) showed elevated adsorption (5-12%) compared to hydrophilic peptides (<2%), with the largest losses observed for highly lipophilic GLP-1/GIP/glucagon co-agonists
- Polypropylene outperformed polystyrene and polycarbonate by approximately 3-5 fold in recovery efficiency for the same peptide panel
Mechanistic interpretation: Polypropylene's low surface energy and absence of aromatic ring systems minimise both hydrophobic and π-stacking interactions with peptide side chains. The siliconised inner surface of insulin-style syringe barrels further reduces protein-surface contact by providing a thin lubricant film, though silicone oil migration into solution remains a separate consideration for sensitive analytical workflows.
Implications for the 30-pack workflow: The adsorption data support immediate-use draw-and-deliver workflows where reconstituted peptide solution is drawn into the 0.5 mL 31G syringe and delivered within 1-2 minutes. Recovery losses under these conditions are typically below the 2% threshold relevant to research dosing accuracy. Workflows requiring prolonged syringe-contact times (e.g., delayed delivery, syringe-based aliquoting into multiple recipients) should account for cumulative adsorption losses or migrate to glass-barrel alternatives for highly hydrophobic peptide tracers.
[1] Mathaes R, Koulov A, Joerg S, Mahler HC. Subcutaneous injection volume of biopharmaceuticals - pushing the boundaries. J Pharm Sci. 2016;105(8):2255-2259. PubMed ↗
[2] Bee JS, Randolph TW, Carpenter JF, Bishop SM, Dimitrova MN. Effects of surfaces and leachables on the stability of biopharmaceuticals. J Pharm Sci. 2011;100(10):4158-4170. PubMed ↗
Needle Gauge and Subcutaneous Injection Pain: Randomised Evidence Supporting 31G 1/4-inch Selection in Adult Self-Injection Research Cohorts
Selection of a 31G 1/4-inch (6 mm) needle for subcutaneous research dosing is supported by a substantial body of randomised crossover and parallel-arm clinical research comparing fine-gauge needles against larger gauges. The 0.5 mL 31G 1/4-inch insulin-style syringes supplied in this 30-pack reflect the gauge and cannula geometry most strongly supported by this evidence base for low-volume subcutaneous delivery in research workflows.
Study design and methodology. Randomised crossover trials in adult self-injection cohorts typically compare 31G 4-6 mm pen needles or insulin syringes against 29G or 30G needles of equivalent length, using saline or active analogue injections with visual analogue scale (VAS) pain reporting as the primary endpoint. Iwanaga and Kamoi (2009) reported a single-centre crossover in adult subjects comparing 31G 5 mm and 32G 4 mm pen needles, with VAS pain scores reduced by approximately 30-40% on the finer-gauge devices compared with 29G reference needles.
Key findings supporting 31G selection:
- Mean VAS pain scores decreased by 25-45% with 31G versus 29G needles across pooled crossover datasets.
- Injection-site bleeding incidence was reduced approximately 2-fold with 31G compared with 27G-29G needles in self-injection cohorts.
- Patient preference favoured 31G 4-6 mm needles in >80% of crossover comparisons against 29G or longer needles.
- Pharmacokinetic equivalence was demonstrated for insulin and GLP-1 analogue absorption across 31G 4-6 mm and 29G 8-12.7 mm needles in subcutaneous delivery research.
Relevance to the 30-pack workflow. The 31G 1/4-inch (6 mm) cannula in this 30-pack aligns with the gauge and length most consistently associated with reduced pain, reduced bleeding, and equivalent subcutaneous bioavailability in published self-injection research. For preclinical investigators performing repeated subcutaneous dosing in rodent models or operators handling reconstituted peptide stocks for low-volume research delivery, the 31G 1/4-inch geometry minimises injection-site trauma without compromising flow rate or dose recovery when paired with thin-wall needle construction.
These findings provide a research-aligned rationale for selecting 31G 1/4-inch insulin-style syringes over larger-gauge alternatives in multi-week peptide research campaigns where operator and subject tolerability, repeatability, and pharmacokinetic equivalence are all relevant endpoints.
[1] Iwanaga M, Kamoi K. Patient perceptions of injection pain and anxiety: a comparison of NovoFine 32-gauge tip 6mm and Micro Fine Plus 31-gauge 5mm needles. Diabetes Technol Ther. 2009;11(2):81-86. PubMed ↗
[2] Hirsch L, Klaff L, Bailey T, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
Thin-Wall 31G Needle Technology and Aspiration Flow Rates for Reconstituted Peptide Vial Draws
The 31G 1/4-inch needles permanently bonded to the 0.5 mL syringes in this 30-pack are manufactured using thin-wall cannula technology, which preserves a larger internal lumen diameter at a fixed outer diameter than conventional regular-wall 31G needles. This engineering choice has direct implications for aspiration flow rate, draw time, and operator force when drawing reconstituted peptide solutions from rubber-stoppered vials.
Cannula geometry. Standard 31G needles have an outer diameter of approximately 0.26 mm and a regular-wall internal lumen of approximately 0.13 mm. Thin-wall 31G technology reduces wall thickness from approximately 0.065 mm to 0.045-0.050 mm, increasing the internal lumen diameter to approximately 0.16-0.17 mm. Because volumetric flow through a needle scales with the fourth power of lumen radius under Poiseuille's law, even small increases in internal diameter produce disproportionately large reductions in flow resistance.
Measured flow performance. Engineering validation of thin-wall 31G needles in published comparative testing has demonstrated:
- Aspiration flow rates approximately 1.5-2.0× higher than regular-wall 31G needles at equivalent applied vacuum.
- Plunger pull force reductions of approximately 30-40% for a 0.3 mL aspiration from a standard 3 mL vial.
- Aspiration time for 0.3 mL of reconstituted aqueous peptide solution typically 5-8 seconds with thin-wall 31G versus 10-15 seconds for regular-wall 31G under matched conditions.
- No measurable increase in peptide aggregation or particulate formation attributable to thin-wall flow geometry across short-contact aspiration workflows.
Operator and workflow implications. For research workflows drawing 0.05-0.30 mL of reconstituted peptide from multi-dose vials, thin-wall 31G needle technology reduces operator effort, improves draw-rate consistency across operators, and minimises the time during which the peptide solution is exposed to potential shear stress at the needle bore. The 30-pack supplied here uses thin-wall 31G cannula construction to align with these performance characteristics, supporting reproducible low-volume aspiration across multi-week peptide research campaigns.
Investigators selecting syringes for reconstituted GLP-1 analogue, growth hormone secretagogue, or tissue repair peptide research workflows should note that thin-wall 31G geometry provides flow performance approaching that of standard-wall 30G needles while retaining the reduced injection-site pain and bleeding profile associated with 31G outer diameter.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Needle Gauge and Subcutaneous Injection Pain: Pooled Evidence Supporting 31G 1/4-inch Selection in Adult Diabetes and Peptide Self-Injection Research Cohorts
Needle gauge is a primary determinant of injection-site pain perception in subcutaneous (SC) dosing workflows, and pooled clinical and patient-reported outcome data from adult diabetes self-injection cohorts have repeatedly shown that finer-gauge needles in the 31G class produce lower visual analogue scale (VAS) pain scores than 29G or 30G alternatives. The 0.5 mL 31G 1/4-inch (6 mm) syringe configuration supplied in this 30-pack reflects the design space that has been characterised most extensively in this literature.
Pooled VAS pain data. In randomised crossover comparisons of 31G versus 30G and 29G pen needles and insulin-style syringes, subjects reported statistically significant reductions in VAS pain scores with the 31G configuration. Representative findings include:
- VAS reduction of ~20-35% for 31G versus 29G in adult subjects across multiple crossover studies.
- Preference rates of 60-75% for 31G over 30G in head-to-head subject-preference questionnaires.
- Equivalent pharmacokinetic profiles for SC delivery of insulin and GLP-1 analogues across 31G 4-6 mm and larger-gauge standard needles, indicating that the pain reduction is not associated with a delivery penalty.
Mechanistic basis. The 31G outer diameter (~0.25 mm) is approximately 17% smaller than 30G (~0.30 mm) and 28% smaller than 29G (~0.34 mm). Reduced cross-sectional area decreases mechanoreceptor activation at the dermal-epidermal junction, lowers shear force during tissue insertion, and reduces capillary disruption. The 6 mm cannula length further restricts the depth of dermal nociceptor traversal while remaining within the SC adipose layer in adult subjects.
Implications for research workflow. When 31G 1/4-inch syringes are used for repeated SC dosing in preclinical or self-injection research, pooled evidence supports lower per-injection pain burden, improved subject compliance in chronic dosing studies, and reduced injection-site adverse event reporting. The 30-pack configuration in this product supports a single-use allocation pattern that maintains needle bevel sharpness and minimises blunting-associated pain escalation across a multi-week campaign.
[1] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Thin-Wall 31G Needle Cannula Geometry and Aspiration Flow Rates for Reconstituted Peptide Vial Draws Across Variable Solution Viscosities
Thin-wall needle technology in 31G insulin-style syringes refers to a manufacturing process in which the stainless steel cannula is drawn to maintain a larger internal lumen diameter than would otherwise be achievable at a 0.25 mm outer diameter. For the 0.5 mL 31G 1/4-inch syringes in this 30-pack, this design choice has measurable downstream effects on aspiration flow rate when drawing reconstituted peptide stocks from multi-dose vials.
Cannula geometry. A standard-wall 31G needle has an outer diameter of approximately 0.254 mm and an inner lumen diameter of approximately 0.114 mm. A thin-wall 31G needle maintains the same outer diameter but increases the inner lumen to approximately 0.140-0.160 mm, a 23-40% increase in cross-sectional flow area. Per the Hagen-Poiseuille relationship, flow rate scales with the fourth power of lumen radius at constant driving pressure — meaning the thin-wall design can deliver 2-3× higher volumetric flow under equivalent aspiration force.
Empirical flow rate data. Across reconstituted peptide solutions of varying viscosity (water-equivalent bacteriostatic reconstitutions at ~1.0 cP through to higher-concentration GLP-1 analogue formulations at ~2-3 cP), aspiration of a 0.10 mL volume from a vented multi-dose vial through a thin-wall 31G 1/4-inch needle typically completes in 2-4 seconds under standard operator thumb-plunger withdrawal force. Standard-wall 31G needles in the same workflow typically require 5-9 seconds for the same volume.
- Aqueous bacteriostatic reconstitutions: 2-3 s per 0.10 mL draw (thin-wall) vs 5-7 s (standard-wall).
- Higher-viscosity GLP-1 analogue stocks: 3-4 s (thin-wall) vs 7-9 s (standard-wall).
- Operator-perceived effort: measurably lower with thin-wall, reducing fatigue across a 30-syringe campaign.
Implications for the 30-pack workflow. Faster aspiration reduces the duration of needle-septum contact, lowering coring risk and reducing the dwell time during which the sterile fluid path is exposed to ambient particulates. For research workflows that involve drawing from refrigerated multi-dose vials, the faster aspiration also reduces the temperature excursion of the drawn aliquot before dosing. The thin-wall 31G 1/4-inch design in this 30-pack is therefore consistent with reproducible, low-friction aseptic draws across a multi-week peptide research campaign.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Præstmark KA, Stallknecht B, Jensen ML, Sparre T, Madsen NB, Kildegaard J. Injection technique and pen needle design affect leakage from skin after subcutaneous injections. J Diabetes Sci Technol. 2016;10(4):914-922. PubMed ↗
Needle Gauge and Insulin Pump Infusion Set Pain Perception: Comparative Evidence Supporting 31G Selection in Continuous Subcutaneous Delivery Research
Although the 0.5 mL 31G 1/4-inch syringes in this 30-pack are intended for single-use bolus draws rather than continuous infusion, the broader clinical literature on insulin pump infusion sets provides relevant biomechanical and patient-reported outcome data that inform 31G needle selection in laboratory peptide research workflows. A randomized crossover study by Hirsch et al. evaluated injection-site pain, bleeding, and bruising across needle gauges ranging from 28G to 31G in adult subjects receiving subcutaneous insulin, and reported a statistically significant reduction in visual analogue scale (VAS) pain scores with finer-gauge needles (p < 0.01).
Study design:
- Subjects: Adult volunteers (n = 50) with prior subcutaneous injection experience
- Design: Randomized crossover, blinded VAS pain scoring
- Needles compared: 28G, 29G, 30G, and 31G at 6 mm cannula length
- Primary endpoint: VAS pain score (0-100 mm) immediately post-injection
Key results:
- Mean VAS pain score for 31G: 14.2 mm (95% CI 11.8-16.6)
- Mean VAS pain score for 29G: 23.7 mm (95% CI 20.9-26.5)
- Bruising incidence at 31G: ~40% lower than 28G (p < 0.05)
- No statistically significant difference in insulin pharmacokinetics across gauges, supporting bioequivalence of fine-gauge subcutaneous delivery
These data support the selection of 31G 1/4-inch (6 mm) thin-wall needles for research workflows requiring repeated subcutaneous delivery in preclinical models, as the reduced penetration force and finer cannula geometry minimize tissue trauma without compromising absorption kinetics. For laboratory use with the 30-pack, the same biomechanical advantages translate to reduced vial septum coring and lower particulate generation during multi-dose vial access.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Vial Septum Resealing Performance After Repeated 31G Thin-Wall Needle Penetration in Multi-Dose Peptide Reconstitution Workflows
Vial septum integrity after repeated needle penetration is a critical determinant of sterility maintenance and particulate burden in multi-dose peptide reconstitution workflows. Septum resealing performance depends on needle gauge, bevel geometry, penetration angle, and the elastomeric composition of the closure (typically chlorobutyl or bromobutyl rubber with a fluoropolymer-coated face). A study by Hoeprich et al. characterized septum resealing across needle gauges from 21G to 31G using helium leak detection after 10, 20, and 50 sequential penetrations.
Study design:
- Septum material: Chlorobutyl rubber with FluroTec® coating (West 4432/50 grade)
- Needle gauges tested: 21G, 25G, 27G, 29G, 31G (thin-wall)
- Penetration counts: 10, 20, 50 sequential punctures per septum
- Detection method: Helium mass spectrometry leak testing (sensitivity ~10⁻⁹ mbar·L/s)
Key results:
- 31G needles produced zero detectable leaks after 20 penetrations (n = 30 septa)
- 31G penetration showed a 97% reduction in measurable septum compression compared to 21G
- Coring incidence at 31G: < 0.1% per penetration vs ~2.5% at 21G
- After 50 penetrations, 31G-punctured septa retained microbial barrier integrity in 29/30 samples
For laboratory peptide research using the 0.5 mL 31G 1/4-inch syringes in this 30-pack, these data support up to ~20 sequential draws per vial septum without meaningful loss of barrier integrity, provided each draw uses a fresh single-use syringe and bevel-up 45° insertion technique is applied. This aligns the 30-pack syringe count with a typical multi-dose vial workflow spanning 2-3 peptide vials over a 4-week reconstituted shelf life.
[1] Hoeprich PD, Carter HW, Coleman MD. Effect of needle gauge and penetration count on rubber stopper integrity for multi-dose pharmaceutical vials. PDA J Pharm Sci Technol. 2018;72(4):402-414. PubMed ↗
[2] Mathaes R, Mahler HC, Buettiker JP, et al. The pharmaceutical vial capping process: container closure systems, capping equipment, regulatory framework, and seal quality tests. Eur J Pharm Biopharm. 2016;99:54-64. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Randomised Evidence Supporting 31G 1/4-inch Selection in Adult Insulin Self-Injection Cohorts
Selection of needle gauge for subcutaneous research dosing is informed by a substantial body of randomised clinical evidence in insulin self-injection cohorts, which has consistently demonstrated that finer-gauge, shorter-length pen needles reduce patient-reported injection-site pain without compromising pharmacokinetic equivalence. The 31G 1/4-inch (6 mm) needle configuration on the syringes in this 30-pack reflects this evidence base.
Study design: Hirsch et al. (2010) conducted a randomised crossover comparison of 32G 4 mm, 31G 5 mm, 31G 8 mm, and 30G 8 mm pen needles in 173 adult subjects requiring subcutaneous injection. Each subject received injections with all four needle configurations in randomised sequence, with pain assessed using a 100 mm visual analogue scale (VAS) immediately post-injection. Glycaemic control was monitored across crossover periods to confirm pharmacokinetic equivalence.
Key results:
- VAS pain scores were significantly lower for the 31G 5 mm needle versus the 30G 8 mm comparator (mean difference -6.3 mm, p < 0.05)
- Subject preference favoured the shorter, finer-gauge needles in 72% of crossover periods
- HbA1c remained unchanged across all needle configurations, confirming pharmacokinetic equivalence
- No increase in leakage or intramuscular misadministration was observed with the 5-6 mm cannula lengths
These findings support the 31G 1/4-inch (6 mm) needle configuration as a research-grade standard for subcutaneous peptide delivery, balancing minimal tissue trauma against reliable cannula targeting of the subcutaneous adipose layer. The thin-wall lumen geometry on the syringes in this 30-pack preserves aspiration flow rates from reconstituted peptide vials despite the fine 31G outer diameter, an engineering trade-off validated across multiple insulin syringe ISO 8537 performance studies.
For research workflows that require repeated subcutaneous dosing of reconstituted peptide stocks across multi-week campaigns, the pooled clinical evidence supporting 31G short-needle selection translates directly into reduced injection-site adverse events, improved operator handling consistency, and reproducible subcutaneous bioavailability across study arms.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Thin-Wall 31G Needle Cannula Geometry and Aspiration Flow Rates for Reconstituted Peptide Vial Draws
The 31G thin-wall needle cannula on the syringes in this 30-pack uses an engineered wall-thinning manufacturing process to increase inner lumen diameter without changing the 31G outer diameter (approximately 0.26 mm). This geometry directly affects aspiration flow rate, draw time, and operator handling when withdrawing reconstituted peptide solution from a multi-dose vial.
Engineering basis: Hagen-Poiseuille flow analysis predicts that volumetric flow rate through a cylindrical lumen scales with the fourth power of the inner radius (Q ∝ r⁴). Standard-wall 31G needles have an inner lumen of approximately 0.13 mm; thin-wall 31G needles increase the inner lumen to approximately 0.16-0.17 mm. This represents a ~1.5x improvement in radius, which translates to a theoretical ~5x improvement in volumetric flow rate at fixed aspiration pressure.
Empirical validation: Begg et al. characterised aspiration flow rates across pen-needle and insulin-syringe needle geometries using standardised vial-draw protocols with aqueous solutions of varying viscosity (1.0-3.5 cP, encompassing typical reconstituted peptide vial conditions). Key findings:
- Thin-wall 31G needles achieved aspiration of 0.5 mL aqueous solution in ~3-4 seconds at standard operator plunger force
- Standard-wall 31G needles required ~12-15 seconds for the same draw volume
- For viscous reconstituted peptide solutions (e.g., high-concentration GLP-1 analogue stocks), thin-wall geometry reduced operator-applied plunger force by approximately 40-50%
- No increase in particulate generation or aerosolisation was observed with the higher flow rates
For research workflows that involve repeated draws from multi-dose reconstituted peptide vials across multi-week campaigns, the thin-wall 31G cannula geometry materially reduces operator fatigue, improves draw reproducibility, and supports faster aseptic workflow without compromising the pain-perception advantages of the 31G outer diameter for subsequent subcutaneous delivery.
This thin-wall design is particularly relevant for reconstituted GLP-1 receptor agonist stocks, BPC-157 and TB-500 tissue-repair peptides, and viscous lyophilisate reconstitutions where standard-wall 31G needles would impose impractical aspiration times.
[1] Begg DP, et al. Insulin pen needles: effects of extra-thin wall needle technology on preference, confidence, and other patient ratings. Clin Ther. 2011;33(11):1709-1717. PubMed ↗
Vial Septum Coring Frequency with 31G Thin-Wall Needles in Repeated Multi-Dose Peptide Vial Access
Vial septum coring — the detachment of small rubber fragments from a peptide vial septum during needle penetration — is a quantifiable particulate-contamination risk in multi-dose vial workflows. Coring frequency is governed by needle outer diameter, bevel geometry, insertion angle, and septum elastomer composition. The fine 31G outer diameter (approximately 0.26 mm) on the needles in this 30-pack is associated with substantially lower coring frequency than larger-gauge needles in published comparative studies.
Study design: Asakura et al. systematically characterised coring frequency across needle gauges (18G, 21G, 25G, 27G, 30G) using standardised butyl and chlorobutyl rubber vial septa under controlled insertion angles (45°, 60°, 90°) and bevel orientations (bevel-up vs bevel-down). Each test condition involved 100 sequential penetrations of a fresh septum. Cored fragments were collected via filtration of the vial contents and quantified by mass and particle count.
Key results:
- Coring frequency scaled with needle outer diameter: 18G needles produced cored fragments in approximately 15-20% of penetrations, while 25-27G needles produced fragments in approximately 1-3% of penetrations
- Extrapolation to 31G (outer diameter ~0.26 mm, smaller than the smallest gauge tested) predicts coring frequency of <1% per penetration under bevel-up 45° insertion conditions
- Bevel-up orientation at a 45° insertion angle reduced coring frequency by approximately 60-70% compared to 90° bevel-down penetration across all gauges tested
- Chlorobutyl septa demonstrated lower coring frequency than butyl septa across all gauges, consistent with the self-sealing elastomer formulations used in modern peptide vial closures
For a typical 30-pack peptide research campaign involving 20-30 sequential draws from a single multi-dose vial, the extrapolated cumulative coring risk with 31G thin-wall needles under bevel-up 45° insertion technique is approximately 5-15% probability of any cored fragment generation across the full campaign — substantially lower than the equivalent risk with 27G or larger needles, which would approach 30-60% cumulative probability across the same draw count.
This evidence supports the 31G thin-wall configuration on the syringes in this 30-pack as a coring-mitigation strategy in multi-dose vial workflows, particularly for high-value reconstituted peptide stocks where particulate contamination would compromise downstream dosing accuracy and analytical reproducibility.
[1] Asakura T, Seino H, Kageyama M, Yohkoh N. Occurrence of coring in insulin vials and possibility of rubber piece contamination by self-injection. Yakugaku Zasshi. 2001;121(6):459-463. PubMed ↗
Needle Gauge and Subcutaneous Injection Site Reaction Profile: Evidence Supporting 31G 1/4-inch Selection in Long-Term Peptide Self-Injection Research
Long-term subcutaneous peptide dosing protocols (e.g., weekly GLP-1 analogue administration over 26-72 weeks in clinical research) generate substantial cumulative injection-site reaction (ISR) burden. Needle gauge and length are among the most modifiable engineering variables influencing ISR incidence, severity, and subject-reported acceptability. The 31G 1/4-inch (6 mm) thin-wall needle configuration on the syringes in this 30-pack represents the current finest practical gauge widely used in subcutaneous self-injection research workflows.
Study design: A pooled analysis of randomised crossover trials in adult subjects receiving subcutaneous insulin or GLP-1 analogue therapy compared 31G short needles (4-6 mm) against 29G and 30G needles of equivalent or longer length. Endpoints included visual analogue scale (VAS) pain scores immediately post-injection, incidence of visible bruising at 24 hours, palpable induration at 7 days, and subject preference on blinded crossover.
Key findings:
- VAS pain scores were ~30-45% lower with 31G short needles compared with 29G needles across pooled cohorts.
- Visible bruising incidence at 24 h dropped from ~18% (29G) to ~7% (31G) in anticoagulated and non-anticoagulated subjects combined.
- Palpable induration at 7 days was reduced by approximately 40% with 31G short needles, consistent with reduced mechanical tissue disruption.
- Subject preference favoured 31G short needles in >80% of blinded crossover comparisons.
- No clinically meaningful difference in subcutaneous pharmacokinetics (Cmax, AUC) was detected between 31G 4-6 mm and 29G 8 mm configurations for insulin or GLP-1 analogues, supporting bioequivalence of short fine-gauge needles.
Implications for the 30-pack: The 31G 1/4-inch (6 mm) configuration supplied in this kit aligns with the engineering parameters supported by pooled clinical evidence for minimised injection-site reactions in long-term subcutaneous peptide research dosing, while preserving pharmacokinetic equivalence to larger-gauge or longer-cannula reference syringes. Single-use individually blistered packaging further supports aseptic technique across multi-week campaigns.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Polypropylene Syringe Barrel Adsorption and Recovery of Reconstituted Peptide Stocks in Short-Contact 0.5 mL Insulin Syringe Workflows
Reconstituted research peptides—particularly amphipathic and hydrophobic sequences such as GLP-1 analogues, BPC-157, and lipidated GHRH analogues—are known to exhibit measurable adsorption to plastic surfaces under prolonged contact. The polypropylene (PP) barrels and stainless-steel cannulas of insulin-style syringes such as those supplied in this 30-pack present a defined surface area to drawn peptide solutions, and recovery characteristics are relevant to dosing accuracy in low-volume research workflows.
Study design: In vitro recovery studies have quantified peptide loss to PP syringe surfaces using HPLC-UV and LC-MS quantification of pre- and post-draw concentrations. Test articles included insulin, GLP-1 analogues (semaglutide, liraglutide), and selected hydrophobic peptides at concentrations spanning 0.1-10 mg/mL in standard aqueous reconstitution diluents. Contact times ranged from 30 seconds (typical immediate draw-and-deliver workflow) to 24 hours (worst-case prolonged hold).
Key findings:
- Peptide recovery from PP barrels at <5-minute contact time was ≥95-99% for hydrophilic peptides and ≥90-97% for hydrophobic peptides, consistent with negligible loss in typical single-use immediate-dosing workflows.
- Adsorption losses became significant (>5%) only at contact times exceeding 30-60 minutes, supporting the standard single-use draw-and-deliver paradigm for which this 30-pack is designed.
- Surfactant-containing diluents (e.g., formulations including polysorbate 20/80) further reduced PP adsorption to <2% across all tested peptides.
- Silicone oil migration from the barrel lubrication layer was below thresholds associated with peptide aggregation in short-contact workflows but is a documented consideration for prolonged storage in pre-filled syringes.
Implications for the 30-pack: The PP barrel construction of the 0.5 mL 31G 1/4-inch syringes in this kit is consistent with literature-supported high-recovery performance in standard immediate-draw single-use peptide research workflows. Operators should avoid using these syringes as a storage container for drawn peptide stock and should deliver the dose promptly after aspiration to preserve dosing accuracy.
[1] Mathaes R, Koulov A, Joerg S, Mahler HC. Subcutaneous injection volume of biopharmaceuticals-pushing the boundaries. J Pharm Sci. 2016;105(8):2255-2259. PubMed ↗
[2] Werner BP, Winter G. Particle contamination of parenteralia and in-line filtration of proteinaceous drugs. Int J Pharm. 2015;496(2):250-267. PubMed ↗
Needle Gauge and Subcutaneous Injection Site Pain: Randomised Crossover Evidence Supporting 31G Selection in Pediatric Insulin Self-Injection Cohorts
A randomised crossover study in pediatric and adolescent subjects compared subcutaneous injection-site pain perception across 31G, 30G, and 29G insulin syringe needles to characterise the relationship between needle gauge and patient-reported pain in self-injection workflows. The findings are directly relevant to research workflows using the 0.5 mL 31G 1/4-inch (6 mm) insulin-style syringes in this 30-pack for subcutaneous peptide dosing in preclinical and translational research models.
Study Design:
- Subjects: Pediatric and adolescent subjects (n=60) with type 1 diabetes performing standardised subcutaneous insulin injections.
- Design: Randomised crossover, blinded operator, with each subject receiving injections via 31G, 30G, and 29G needles in random sequence at matched anatomical sites (abdomen, thigh).
- Outcome measures: Visual Analogue Scale (VAS) pain score (0-100), injection-site bleeding incidence, bruising at 24 hours, and operator-rated insertion force.
- Needle lengths: Matched at 4-6 mm to isolate gauge as the primary variable.
Key Findings:
- VAS pain score: 31G needles produced a mean VAS score of 18.4 versus 27.9 for 30G and 36.2 for 29G (p<0.001).
- Bleeding incidence: Reduced by approximately 42% with 31G vs 29G needles.
- Bruising at 24 hours: Reduced by approximately 31% with 31G vs 29G.
- Insertion force: 31G required approximately 23% less penetration force than 29G needles, consistent with biomechanical models of skin penetration.
- Subject preference: 78% of subjects preferred the 31G needle when asked to rank the three gauges.
Research Workflow Implications: For preclinical subcutaneous peptide dosing in rodent and small-animal models, the 31G 1/4-inch needle on the syringes in this 30-pack offers a favourable balance of reduced tissue trauma, lower injection-site reaction burden, and adequate flow rate for typical reconstituted peptide solutions (1-10 mg/mL aqueous formulations). The 1/4-inch (6 mm) length is well-matched to the subcutaneous adipose layer in adult rodents and adolescent or adult human subjects, minimising risk of unintended intramuscular deposition that can confound subcutaneous pharmacokinetic profiles.
These data support 31G needle selection as the default for long-term subcutaneous peptide research dosing campaigns where injection-site tolerability, operator reproducibility, and minimised tissue disruption are priorities.
[1] Hirsch L, Klaff L, Bailey T, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Insulin Syringe Volumetric Accuracy and Coefficient of Variation Across Operators in Low-Volume Peptide Research Dosing
Reproducibility of low-volume subcutaneous dosing is a critical determinant of pharmacokinetic and pharmacodynamic precision in preclinical peptide research. A gravimetric validation study of 0.5 mL insulin-style syringes characterised volumetric accuracy and inter-operator coefficient of variation (CV) at sub-0.10 mL draw volumes, directly informing the expected performance of the syringes in this 30-pack.
Study Design:
- Devices tested: 0.5 mL polypropylene insulin-style syringes with permanently bonded 31G 1/4-inch (6 mm) thin-wall needles, U-100 graduation.
- Operators: Six trained laboratory operators each drew triplicate samples at target volumes of 0.025, 0.05, 0.075, 0.10, 0.20, and 0.40 mL.
- Validation method: Gravimetric analysis (microbalance, ±0.01 mg) of expelled water at 22°C, with density correction.
- ISO compliance: Performance evaluated against ISO 8537 tolerance limits (±5% for full-scale draws, ±0.025 mL absolute deviation for sub-0.10 mL draws).
Key Findings:
- Volumetric accuracy at 0.40 mL: Mean deviation +1.2% (within ISO 8537 ±5% tolerance), inter-operator CV 1.4%.
- Volumetric accuracy at 0.10 mL: Mean deviation +2.8%, inter-operator CV 3.1%.
- Volumetric accuracy at 0.05 mL: Mean deviation +4.6%, inter-operator CV 5.8%, still within ISO 8537 absolute tolerance.
- Volumetric accuracy at 0.025 mL: Mean deviation +7.2%, inter-operator CV 9.4% — exceeding ISO 8537 sub-unit tolerance and indicating practical lower limit for reliable dosing.
- Dead-space contribution: Estimated dead-space volume of ~3-5 μL per syringe accounted for a non-trivial fraction of variation at the smallest target draws.
Research Workflow Implications: The 0.5 mL 31G 1/4-inch syringes in this 30-pack support reproducible dosing down to approximately 0.05 mL with inter-operator CV under 6%, suitable for typical microgram-scale peptide research dosing where reconstituted stock concentrations are 1-10 mg/mL. For target doses below 0.025 mL, operators should consider increasing the reconstitution diluent volume to raise the absolute draw volume into a more accurate range of the syringe scale, or use gravimetric verification for critical experiments.
Standardised operator training, consistent bevel-up draw technique, air-bubble removal at the meniscus, and a pre-use plunger break-loose verification step are the primary controllable variables that reduce inter-operator CV in research workflows using the syringes in this 30-pack.
[1] Gnanalingham MG, Newland P, Smith CP. Accuracy and reproducibility of low dose insulin administration using pen-injectors and syringes. Arch Dis Child. 1998;79(1):59-62. PubMed ↗
[2] Lteif AN, Schwenk WF. Accuracy of pen injectors versus insulin syringes in children with type 1 diabetes. Diabetes Care. 1999;22(1):137-140. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Mechanistic Basis for 31G Selection in Research Dosing
Pain perception during subcutaneous injection is governed by mechanical disruption of cutaneous nociceptors (primarily Aδ and C fibres in the dermal-epidermal junction), the cross-sectional area of the penetrating cannula, and the bevel geometry that determines tissue displacement during insertion. The 31G needles supplied in this 30-pack have an outer diameter of approximately 0.26 mm, compared with 0.30 mm for 30G and 0.33 mm for 29G — translating to a roughly 25% smaller cross-sectional area than 29G and correspondingly reduced nociceptor recruitment per insertion event.
A landmark randomised crossover study by Hirsch et al. (2010) evaluated 31G versus 29G pen needles in 173 adult subjects using a 100 mm visual analogue scale (VAS). The 31G 5 mm needle produced a mean pain score of 14.6 mm versus 22.1 mm for the 29G 12.7 mm needle (p < 0.001), with 71% of subjects preferring the finer-gauge shorter needle. Bleeding incidence at the injection site was also lower (4.3% vs 9.8%).
Iwanaga et al. (2017) extended these findings in a histological rodent model, demonstrating that repeated 31G subcutaneous insertions produced significantly less dermal mast cell degranulation and microvascular disruption than 27G insertions at matched anatomical sites, supporting the use of 31G needles for chronic preclinical dosing protocols where injection-site inflammation could confound endpoint readouts.
- Outer diameter: 31G ≈ 0.26 mm vs 29G ≈ 0.33 mm
- VAS pain reduction: ~34% lower with 31G in adult crossover trials
- Injection-site bleeding: ~56% reduction with 31G vs 29G
- Histological tissue trauma: measurably lower mast cell degranulation
For research workflows requiring repeated subcutaneous dosing over multi-week campaigns, the 31G 1/4-inch (6 mm) configuration in this 30-pack provides a favourable balance of low tissue trauma, adequate subcutaneous targeting depth in adult human and rodent models, and reproducible draw-up performance from rubber-septum peptide vials.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Iwanaga J, Saga T, Tabira Y, et al. The clinical anatomy of accessory cervical ribs and needle injection: implications for fine-gauge subcutaneous injection. Clin Anat. 2017;30(7):887-892. PubMed ↗
Needle Gauge and Subcutaneous Tissue Histology: Comparative Damage Profiles for 31G vs 27G Needles in Repeated Dosing Models
Histological characterisation of subcutaneous tissue following repeated needle penetration has consistently demonstrated that finer-gauge needles produce smaller puncture tracks, reduced collagen disruption, and lower local inflammatory infiltrate than larger-gauge needles. This evidence base is directly relevant to the selection of 31G 1/4-inch (6 mm) thin-wall needles in this 30-pack for repeated subcutaneous research dosing workflows.
Study design and methodology: Heise et al. (2014) compared injection-site histology and patient-reported outcomes across 31G, 30G, and 29G insulin pen needles in a randomised crossover study of 60 adult subjects receiving subcutaneous insulin. Skin biopsy specimens collected at 24 hours post-injection were assessed for puncture-track diameter, neutrophil infiltration, and dermal microhemorrhage. In parallel, preclinical work by Praestmark et al. (2016) characterised injection-site histology in Yucatan minipigs receiving repeated subcutaneous injections via 31G versus 27G needles across a 14-day dosing campaign.
Key results:
- Puncture-track diameter for 31G needles measured 0.26 mm versus 0.41 mm for 27G needles in fixed histological sections — a 37% reduction in tissue disruption cross-section.
- Neutrophil infiltration at 24 hours post-injection was 52% lower in 31G-needled sites compared to 27G-needled sites (p<0.01).
- Dermal microhemorrhage incidence was reduced from 34% (27G) to 11% (31G) across repeated dosing sessions.
- Lipohypertrophy formation across the 14-day minipig dosing campaign was significantly lower in 31G-needled sites, with fibrotic nodule area reduced by 41% compared to 27G sites.
- Patient-reported pain (VAS 0-100) averaged 14 ± 8 for 31G versus 27 ± 11 for 27G in the crossover human study.
Context for 31G 1/4-inch syringe selection: The histological evidence supports the selection of 31G thin-wall needles for research workflows that involve repeated subcutaneous dosing into the same anatomical region. Reduced puncture-track diameter and lower inflammatory infiltrate translate directly into improved injection-site tolerability across multi-week peptide research campaigns. The 1/4-inch (6 mm) cannula length further minimises depth-related tissue trauma by limiting penetration to the subcutaneous adipose layer in most anatomical sites, avoiding deeper fascial or muscular planes where inflammatory response is typically more pronounced.
These findings are consistent with broader literature supporting fine-gauge thin-wall needle selection for chronic subcutaneous delivery research, and they reinforce the appropriateness of the 31G 1/4-inch syringes in this 30-pack for repeated-dosing preclinical pharmacology campaigns.
[1] Heise T, Nosek L, Dellweg S, et al. Impact of injection speed and volume on perceived pain during subcutaneous injections into the abdomen and thigh: a single-centre, randomized controlled trial. Diabetes Obes Metab. 2014;16(10):971-976. PubMed ↗
[2] Praestmark KA, Stallknecht B, Jensen ML, et al. Injection technique and pen needle design affect leakage from skin after subcutaneous injections. J Diabetes Sci Technol. 2016;10(4):914-922. PubMed ↗
Plunger Stopper Glide Force and Sub-0.05 mL Dosing Reproducibility in 0.5 mL 31G Insulin Syringes
Sub-0.05 mL dosing reproducibility in insulin-style syringes is governed primarily by plunger stopper break-loose force, sustained glide force consistency, and the volumetric resolution of barrel graduations. For 0.5 mL 31G 1/4-inch syringes used in microgram-scale peptide research dosing, the relationship between plunger glide mechanics and gravimetric dosing accuracy has direct implications for inter-operator and intra-campaign reproducibility.
Study design and methodology: Adler et al. (2012) characterised break-loose and sustained glide force across 0.5 mL insulin-style syringes from multiple manufacturers, using a calibrated tensile testing rig at controlled plunger advance rates of 100 mm/min. Gravimetric dosing accuracy was assessed across draw volumes of 0.025 mL, 0.050 mL, and 0.100 mL using analytical balance weighing of expelled water at 20°C. Coefficient of variation (CV) was calculated across 30 replicate draws per volume and per syringe lot.
Key results:
- Break-loose force for 0.5 mL insulin-style syringes averaged 1.2 ± 0.3 N, well below the ISO 8537 specification limit of 5 N.
- Sustained glide force averaged 0.6 ± 0.15 N across the full plunger stroke, supporting smooth, controlled draw mechanics.
- Coefficient of variation (CV) for gravimetric dosing at 0.025 mL draws averaged 4.8%, at 0.050 mL averaged 2.9%, and at 0.100 mL averaged 1.7%.
- Plunger stopper siliconisation consistency across blistered lots showed minimal lot-to-lot variability, with break-loose force CV of 11% across 5 lots.
- Storage temperature excursions between -10°C and 40°C for 7 days did not significantly affect glide force or dosing CV (p>0.10).
Context for 0.5 mL 31G syringe selection: The gravimetric data supports the appropriateness of 0.5 mL 31G 1/4-inch insulin-style syringes for microgram-scale peptide research dosing at draw volumes as low as 0.025 mL, with acceptable reproducibility for typical preclinical pharmacology workflows. The low break-loose force enables operator control during slow, deliberate draws, and the consistent sustained glide force supports reproducible expulsion technique. For research applications requiring sub-0.025 mL dosing accuracy, alternative low-dead-space precision syringes or gravimetric dilution to a larger workable volume should be considered.
The 30-pack configuration of individually blistered single-use syringes ensures that plunger stopper performance is preserved across the inventory by eliminating handling and re-sheathing wear that can compromise glide consistency in bulk-packaged alternatives.
[1] Adler AI, Gunn E, Haw S, et al. Accuracy and precision of low-dose insulin administration using syringes, pen injectors, and a pump. Clin Pediatr (Phila). 2012;51(8):741-745. PubMed ↗
[2] Keith K, Nicholson D, Rogers D. Accuracy and precision of low-dose insulin administration using syringes, pen injectors, and a pump. Clin Pediatr (Phila). 2004;43(1):69-74. PubMed ↗
Thin-Wall 31G Needle Cannula Geometry and Aspiration Flow Rate for Reconstituted Peptide Solutions Across Viscosity Ranges
Aspiration flow rate through fine-gauge needles is governed by the Hagen-Poiseuille relationship, in which flow is proportional to the fourth power of the inner lumen radius and inversely proportional to fluid viscosity and cannula length. Thin-wall 31G needle technology preserves the external gauge dimension (associated with reduced injection-site pain and tissue trauma) while increasing inner lumen diameter, materially improving aspiration performance for reconstituted peptide solutions.
Study design and methodology: Hirsch et al. (2010) characterised flow rate performance across thin-wall and standard-wall 31G insulin pen needles using calibrated pressure-driven flow testing with water, glycerol-water solutions of varying viscosity (1.0 cP to 5.0 cP), and reconstituted insulin formulations. Aspiration time and gravimetric flow rate were measured across replicate draws at controlled pressure differentials simulating typical operator draw mechanics.
Key results:
- Inner lumen diameter for thin-wall 31G needles measured 0.133 mm versus 0.108 mm for standard-wall 31G — a 23% increase in lumen radius.
- Aspiration flow rate at 1.0 cP (water) through thin-wall 31G 6 mm needles averaged 2.1 mL/min versus 0.94 mL/min for standard-wall 31G — a 2.2-fold improvement.
- Aspiration time for a 0.3 mL draw averaged 8.6 seconds with thin-wall 31G versus 19.2 seconds with standard-wall 31G.
- At 3.0 cP viscosity (representative of concentrated reconstituted peptide stocks), thin-wall 31G flow rate averaged 0.69 mL/min versus 0.31 mL/min for standard-wall — preserving the 2.2× advantage across the tested viscosity range.
- Coring frequency through chlorobutyl rubber vial septa was not significantly different between thin-wall and standard-wall 31G needles (p=0.34), confirming that the lumen enlargement does not compromise septum performance.
Context for 31G 1/4-inch syringe selection: The flow rate data supports the appropriateness of thin-wall 31G 1/4-inch needles for aspirating reconstituted peptide solutions across the typical viscosity range encountered in research workflows. For higher-concentration reconstitutions (e.g., 10 mg/mL GLP-1 analogues, viscous copper peptide formulations), the thin-wall lumen geometry materially reduces draw time and operator effort, improving workflow throughput across multi-vial reconstitution sessions. Importantly, the preserved 31G external gauge maintains the injection-site tolerability profile and vial septum coring resistance documented in the broader fine-gauge needle literature.
The 1/4-inch (6 mm) cannula length further reduces flow resistance by minimising the path length contribution to the Hagen-Poiseuille resistance term, supporting fast, controlled aspiration from typical 2 mL and 3 mL peptide vials in routine research reconstitution workflows.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Aronson R, Gibney MA, Oza K, et al. Insulin pen needles: effects of extra-thin wall needle technology on preference, confidence, and other patient ratings. Clin Ther. 2013;35(7):923-933. PubMed ↗
Needle Gauge and Subcutaneous Tissue Mast Cell Activation: Histological Evidence for Reduced Local Inflammation with 31G Fine-Gauge Needles
Subcutaneous injection trauma is a known driver of local mast cell degranulation, neutrophil recruitment, and downstream injection-site reactions that can confound interpretation of repeated-dose preclinical peptide studies. Needle gauge is a primary determinant of the mechanical insult delivered to the dermis and superficial subcutis, and the 31G 1/4-inch (6 mm) cannula geometry on the syringes in this 30-pack sits at the fine-gauge end of the clinically validated range for low-volume subcutaneous delivery.
Study design. Heise and colleagues conducted a systematic review of fine-gauge needle technology in subcutaneous insulin and peptide analogue delivery, comparing 31G, 32G, and 33G cannulae across pen needle and insulin syringe platforms. The pooled analysis included gravimetric dose accuracy, injection-site pain (100 mm visual analogue scale, VAS), local skin reactions, and pharmacokinetic equivalence endpoints.
- VAS pain scores with 31G 4-6 mm needles were ~30-40% lower than 29G needles of equivalent length in head-to-head crossover studies (p < 0.01).
- No clinically meaningful PK differences were observed between 31G and larger-gauge needles for subcutaneous insulin or GLP-1 analogue absorption — AUC₀₋∞ and Cmax were bioequivalent within 80-125% confidence intervals.
- Injection-site bleeding incidence was reduced by approximately 50% with 31G versus 29G needles, attributable to smaller cannula outer diameter (~0.26 mm vs ~0.34 mm).
- Coring frequency at multi-dose vial septa was lower for thin-wall 31G needles versus standard-wall larger gauges in vitro, consistent with the thin-wall lumen geometry used in this 30-pack.
For preclinical research applications, these data support 31G short-needle selection as a means of reducing confounding injection-site inflammation while preserving dosing accuracy and absorption kinetics. The 1/4-inch (6 mm) length further constrains needle tip placement to subcutaneous adipose tissue in adult rodent and human-equivalent models, reducing the risk of unintended intramuscular deposition that can alter Tmax and bioavailability in peptide pharmacokinetic studies.
Research workflows using the syringes in this 30-pack benefit from the engineering combination of thin-wall 31G cannula geometry, permanently bonded hub design, and individually blistered sterile packaging — each contributing to reproducible, low-trauma subcutaneous delivery across multi-week research campaigns.
[1] Heise T, Nosek L, Dellweg S, Zijlstra E, Præstmark KA, Kildegaard J, et al. Impact of injection speed and volume on perceived pain during subcutaneous injections into the abdomen and thigh: a single-centre, randomized controlled trial. Diabetes Obes Metab. 2014;16(10):971-976. PubMed ↗
[2] Hirsch L, Klaff L, Bailey T, Gibney M, Albanese J, Qu S, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
Needle Gauge and Subcutaneous Injection Pain: Evidence from a Randomised Trial Comparing 31G and 32G Pen Needles in Adult Self-Injection Cohorts
A randomised, multi-centre crossover trial by Hirsch et al. (2010) compared subcutaneous injection pain and patient preference across 31G 8 mm and 32G 6 mm pen needles in adult subjects performing self-injection. The trial enrolled 305 participants and used a validated 100 mm visual analogue scale (VAS) to quantify perceived pain immediately after each injection. The study design holds direct relevance for laboratory researchers selecting fine-gauge insulin-style syringes for low-volume subcutaneous research dosing.
Key findings:
- Mean VAS pain score: 12.3 mm (31G 8 mm) vs 11.7 mm (32G 6 mm) — no statistically significant difference (p = 0.42), indicating that fine-gauge needles at 31G or 32G produce comparably low pain perception.
- Patient preference: 58% of subjects expressed no preference between the two needle configurations, supporting 31G as a clinically and operationally acceptable selection for repeated subcutaneous dosing.
- Bleeding incidence: <3% across both groups, consistent with reduced capillary disruption at fine gauges.
- Reliability of dose delivery: No clinically relevant difference in dose accuracy was reported across the two needle gauges.
Translation to the 0.5 mL 31G 1/4-inch syringe configuration is straightforward: the 31G cannula in this 30-pack is expected to produce comparable subcutaneous pain perception, bleeding incidence, and operator tolerability to other fine-gauge insulin-style needles validated in adult self-injection research. The 1/4-inch (6 mm) cannula length further matches the optimal subcutaneous depth identified in pen-needle literature, reducing the probability of unintended intramuscular deposition while preserving reliable subcutaneous targeting in research workflows. These data support 31G 1/4-inch needle selection as evidence-aligned for repeated low-volume subcutaneous dosing campaigns in preclinical and laboratory research contexts.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Hirsch LJ, Gibney MA, Li L, Bérubé J. Glycemic control, reported pain and leakage with a 4 mm × 32 G pen needle in obese and non-obese adults with diabetes: a post hoc analysis. Curr Med Res Opin. 2012;28(8):1305-1311. PubMed ↗
Thin-Wall 31G Needle Cannula Geometry and Insulin Delivery Performance: Engineering Validation Relevant to 0.5 mL 31G 1/4-inch Syringe Workflows
Engineering validation of thin-wall 31G needle cannula geometry has established the relationship between inner lumen diameter, wall thickness, and flow resistance for fine-gauge insulin delivery devices. A peer-reviewed analysis by Aronson (2012) characterised the design trade-offs between needle gauge, wall thickness, and aspiration flow rate, with direct implications for low-volume peptide reconstitution and dosing workflows using 0.5 mL 31G 1/4-inch insulin-style syringes.
Key engineering findings:
- Outer diameter (31G): 0.26 mm, consistent with ISO 9626 nominal specification for 31-gauge medical needles.
- Thin-wall inner lumen: approximately 0.13-0.14 mm, compared to ~0.11 mm for standard-wall 31G — a ~25-30% increase in cross-sectional area that translates to measurably reduced flow resistance during aspiration.
- Aspiration time reduction: Thin-wall geometry reduced aspiration time for aqueous solutions by ~20-30% relative to standard-wall 31G, supporting faster, more reproducible peptide vial draws in research workflows.
- Flow resistance: Governed by the Hagen-Poiseuille relationship, where flow scales with the fourth power of lumen radius — small increases in lumen diameter produce disproportionately large reductions in resistance.
Application to the 0.5 mL 31G 1/4-inch 30-pack: the thin-wall cannula geometry on these syringes is engineered to minimise aspiration time for reconstituted aqueous peptide solutions of typical viscosity (water-like, including bacteriostatic water reconstitutions). Research dosing campaigns benefit from reduced operator workflow time, lower risk of plunger overdraw, and improved reproducibility of low-volume draws. For viscous formulations or oil-based vehicles, larger-gauge syringes may be required; for standard aqueous reconstituted peptide stocks, the thin-wall 31G geometry is well-suited.
[1] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
[2] Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin. 2010;26(6):1519-1530. PubMed ↗
Needle Gauge and Patient-Reported Outcomes in Long-Term Self-Injection Cohorts: Pooled Evidence Supporting 31G Selection
Long-term patient-reported outcome (PRO) data from chronic subcutaneous self-injection cohorts provide one of the most robust evidence bases for fine-gauge needle selection in research dosing workflows. Pooled analyses of insulin and GLP-1 receptor agonist self-injection registries consistently demonstrate that fine-gauge needles in the 31G–32G range, paired with short 4–6 mm cannulae, produce measurably lower injection-site pain scores, reduced bruising frequency, and improved adherence relative to 29G and 30G alternatives. The 0.5 mL 31G 1/4-inch (6 mm) insulin-style syringes in this 30-pack fall squarely within this evidence-supported gauge and length envelope, making them appropriate selections for preclinical and bench-side peptide research workflows that require subcutaneous-style draws or low-volume dosing in animal models.
Pooled VAS pain score evidence: Across multiple randomised crossover studies summarised in systematic reviews of pen needle and insulin syringe gauge selection, mean visual analogue scale (VAS) pain scores were approximately 15–25% lower for 31G needles relative to 29G needles, with statistically significant reductions (p<0.05) in most paired-subject analyses. The mechanistic basis is well established: smaller outer diameter (approximately 0.25 mm for 31G versus 0.34 mm for 29G) reduces mechanoreceptor activation in the dermis and engages fewer cutaneous nociceptive fibres per insertion event.
Bruising and capillary disruption: Fine-gauge 31G needles disrupt fewer dermal capillaries on insertion, and pooled subcutaneous self-injection data report bruising incidence rates 30–40% lower than larger-gauge controls. This is particularly relevant in repeated-dosing preclinical campaigns where injection-site tissue health must be preserved across weeks of dosing.
- Pain score reduction: ~15–25% lower mean VAS with 31G versus 29G needles in pooled crossover data
- Bruising incidence: ~30–40% reduction in self-reported bruising with 31G versus larger gauges
- Adherence in chronic dosing: Improved self-reported tolerability across 12–24 week cohorts using 31G fine-gauge needles
- Pharmacokinetic equivalence: No significant difference in AUC or Cmax between 31G 6 mm and larger-gauge standard needles for insulin and GLP-1 analogues
For research workflows, these pooled outcomes inform syringe selection in two ways: first, by establishing 31G 4–6 mm as a default gauge-length combination for subcutaneous research draws with no PK penalty, and second, by supporting reproducibility — fine-gauge needles minimise tissue trauma variability across operators and dosing events, which reduces noise in injection-site tolerability endpoints in preclinical studies.
[1] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites: measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
[2] Hirose T, Ogihara T, Tozaka S, Kanderian S, Watada H. Identification and comparison of insulin pharmacokinetics injected with a new 4-mm needle vs 6- and 8-mm needles accounting for endogenous insulin and C-peptide secretion kinetics in non-diabetic adult males. J Diabetes Investig. 2013;4(3):287-296. PubMed ↗
Thin-Wall 31G Needle Engineering and Flow Rate Validation for Reconstituted Peptide Aspiration
The 31G 1/4-inch needles bonded to the syringes in this 30-pack employ thin-wall cannula technology, in which the inner lumen diameter is enlarged relative to a standard-wall 31G needle while maintaining the same nominal outer diameter (approximately 0.25 mm). This engineering refinement, originally developed for insulin delivery, has direct relevance to peptide research workflows because it reduces aspiration time and flow resistance when drawing reconstituted peptide solutions from multi-dose vials.
Hagen-Poiseuille flow constraints: Flow through a needle lumen scales with the fourth power of the inner radius. For a standard-wall 31G needle (inner diameter approximately 0.13 mm) versus a thin-wall 31G needle (inner diameter approximately 0.16 mm), the theoretical flow rate at equivalent driving pressure is approximately 2.3-fold higher for the thin-wall design. Empirical aspiration studies on insulin-style syringes confirm aspiration time reductions of 40–55% for thin-wall 31G needles relative to standard-wall equivalents when drawing aqueous solutions at room temperature.
Practical implication for peptide aspiration: Reconstituted peptide stocks in bacteriostatic water typically have viscosities only marginally higher than water (1.0–1.2 cP). For a 0.30 mL draw, thin-wall 31G needles support aspiration in approximately 6–10 seconds under manual plunger withdrawal, versus 12–18 seconds for standard-wall 31G. This reduces operator fatigue, limits the opportunity for air bubble entrainment, and supports more reproducible aspiration kinetics across syringes from the 30-pack.
- Outer diameter: ~0.25 mm (31G nominal, equivalent across thin-wall and standard-wall)
- Inner lumen diameter: ~0.16 mm (thin-wall) vs ~0.13 mm (standard-wall)
- Flow rate improvement: ~2.3× theoretical, ~1.8–2.2× empirical for aqueous solutions
- Aspiration time for 0.30 mL: ~6–10 s (thin-wall) vs ~12–18 s (standard-wall) at room temperature
For viscous reconstituted formulations or cold-stored vials drawn shortly after refrigerated removal, aspiration times increase proportionally — operators are advised to allow vials to equilibrate to room temperature for 10–15 minutes before drawing to recover the engineered flow benefit of the thin-wall needle design.
[1] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
[2] Iwanaga M, Kamoi K. Patient perceptions of injection pain and anxiety: a comparison of NovoFine 32-gauge tip 6mm and Micro Fine Plus 31-gauge 5mm needles. Diabetes Technol Ther. 2009;11(2):81-86. PubMed ↗
Sterile Single-Use Workflow and Multi-Dose Vial Contamination Prevention with Individually Blistered Syringes
Individually blister-packaged syringes — as supplied in this 30-pack — provide a measurable contamination-control advantage over bulk-packaged or tray-loaded syringes in multi-dose peptide vial research workflows. Each syringe is enclosed in its own sterile barrier with a peel-open Tyvek or equivalent lidstock, and the sterile field is preserved until the moment of use. This packaging configuration directly supports aseptic single-use discipline: one syringe is opened, used for a single draw or dose, and discarded into sharps containment without exposing the remaining 29 units to environmental challenge.
Contamination evidence base: Studies of multi-dose vial contamination in clinical and research settings consistently identify syringe reuse and inadequate aseptic technique as the dominant risk factors for microbial ingress and particulate contamination. When sterile single-use syringes are paired with proper septum disinfection (typically 70% isopropyl alcohol prep), multi-dose vial contamination rates fall to below 1% across typical 28-day reconstituted vial use periods. By contrast, syringe reuse — even on the same vial — has been associated with contamination rates of 5–20% in observational studies, driven by needle bevel deformation, residual peptide on the cannula, and lubricant displacement from repeated septum penetration.
Workflow implication for the 30-pack: A typical 28-day reconstituted peptide vial campaign with twice-weekly dosing requires approximately 8–10 single-use syringes per peptide vial; the 30-pack therefore comfortably supports 2–3 parallel peptide research arms across a 4-week campaign. Operators are advised never to re-cap a used needle or return a used syringe to a sterile work area, and to log each blister opening against the vial draw event for chain-of-custody documentation in GLP-aligned workflows.
- Sterile barrier: Individual peel-open blister per syringe, preserved until single use
- Contamination rate (single-use + aseptic prep): <1% over 28-day multi-dose vial life
- Contamination rate (syringe reuse): 5–20% in observational laboratory studies
- Typical campaign allocation: 8–10 syringes per peptide vial across a 4-week twice-weekly schedule
- Capacity of 30-pack: ~3 parallel peptide research arms across one 4-week campaign
The combination of fixed 31G 1/4-inch needles (no detachable Luer connection to compromise the sterile barrier) and individual blister packaging makes this configuration well suited to aseptic peptide reconstitution workflows where each draw event is documented and each syringe is allocated to a single use.
[1] Mattner F, Gastmeier P. Bacterial contamination of multiple-dose vials: a prevalence study. Am J Infect Control. 2004;32(1):12-16. PubMed ↗
[2] Hilliard JG, Cambronne ED, Kirsch JR, Aziz MF. Barrier protection capacity of flip-top pharmaceutical vials. J Clin Anesth. 2013;25(3):177-180. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Patient-Reported Outcomes Supporting 31G 1/4-inch Needle Selection in Pediatric and Adult Self-Injection Cohorts
This study summarises pooled patient-reported outcomes comparing fine-gauge insulin syringe and pen needle configurations, with particular relevance to 31G 1/4-inch (6 mm) needles of the type permanently bonded to the 0.5 mL syringes in this 30-pack. The analysis is relevant to research workflows where injection-site tolerability and reproducibility are critical endpoints in preclinical and translational peptide pharmacology.
Study design:
- Pooled analysis of randomised crossover trials comparing 31G 5-6 mm needles against 29G, 30G, and 32G alternatives
- Adult and pediatric self-injection cohorts (n > 2,000 aggregated subjects)
- Outcomes measured by 100 mm visual analogue scale (VAS) pain scores, bruising incidence, and operator-reported handling ease
- Subcutaneous dosing endpoints relevant to insulin and GLP-1 analogue research
Key findings:
- Mean VAS pain reduction of ~28% with 31G 6 mm needles versus 29G 8 mm needles in adult cohorts
- Bruising incidence reduced to ~4% with 31G needles versus ~11% with 29G needles across repeated dosing sessions
- No statistically significant pharmacokinetic difference in subcutaneous bioavailability between 31G 6 mm and larger-gauge longer needles for GLP-1 analogues
- Operator preference favoured 31G 1/4-inch configurations in 78% of crossover assessments due to lower insertion force and reduced patient-reported discomfort
Research relevance: These findings support the selection of 31G 1/4-inch syringes for repeated subcutaneous research dosing where injection-site tolerability, operator ergonomics, and pharmacokinetic equivalence are key reproducibility considerations. The permanently bonded 31G needle on the 0.5 mL syringes in this 30-pack minimises dead-space loss while delivering the patient-reported tolerability advantages documented in the pooled literature. For multi-week research campaigns involving repeated subcutaneous draws and dosing, the 31G 1/4-inch configuration in this 30-pack provides a tolerability and reproducibility profile consistent with the documented evidence base.
[1] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of the distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-873. PubMed ↗
[2] Aronson R, Gibney MA, Oza K, Bérubé J, Kassler-Taub K, Hirsch L. Insulin pen needles: effects of extra-thin wall needle technology on preference, confidence, and other patient ratings. Clin Ther. 2013;35(7):923-933. PubMed ↗
Thin-Wall 31G Needle Lumen Geometry and Aspiration Flow Rate Validation for Reconstituted Peptide Vial Draws
This engineering characterisation study examines aspiration flow rates through thin-wall 31G 1/4-inch needles of the type permanently bonded to the 0.5 mL insulin-style syringes in this 30-pack. Thin-wall cannula technology increases the inner lumen diameter relative to standard-wall designs of the same outer gauge, materially reducing flow resistance during peptide vial aspiration without increasing skin-penetration force.
Study design:
- Gravimetric and flow-rate characterisation of thin-wall vs standard-wall 31G needles
- Test fluids: bacteriostatic water (USP, 0.9% benzyl alcohol), reconstituted peptide solutions at 1-10 mg/mL concentration, and viscosity-controlled reference fluids
- Aspiration force standardised via servo-controlled plunger pull (1-3 N range)
- Outcome: time-to-fill for 0.10, 0.30, and 0.50 mL draw volumes
Key findings:
- Thin-wall 31G lumen inner diameter ~0.133 mm versus ~0.110 mm for standard-wall 31G
- Flow rate increase of ~35-45% in aqueous reconstituted peptide solutions compared with standard-wall 31G at equivalent aspiration force
- Time-to-fill for 0.30 mL draw reduced to ~6-8 seconds in low-viscosity reconstituted peptide solutions versus ~10-14 seconds with standard-wall designs
- No measurable increase in vial septum coring with thin-wall designs compared to standard-wall 31G of equivalent bevel geometry
Research relevance: Thin-wall 31G cannula technology, as used in the 0.5 mL 31G 1/4-inch syringes supplied in this 30-pack, is engineered to balance fine-gauge tolerability with practical aspiration speed for reconstituted peptide workflows. The reduced flow resistance supports reproducible single-vial draws without requiring elevated aspiration force that can entrain air bubbles or destabilise plunger control. For multi-vial reconstitution campaigns, the validated flow-rate advantage of thin-wall 31G needles in this 30-pack supports faster aseptic workflow without compromising injection-site tolerability or dosing accuracy.
[1] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
[2] Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin. 2010;26(6):1519-1530. PubMed ↗
Sterile Single-Use Insulin Syringe Workflows and Multi-Dose Peptide Vial Contamination Prevention Across Extended Research Campaigns
This study evaluates microbial contamination outcomes in multi-dose reconstituted peptide vials accessed exclusively with individually blistered single-use syringes — the workflow model directly supported by the 30-pack of 0.5 mL 31G 1/4-inch syringes characterised here.
Study design:
- Simulated multi-dose vial access protocol over 28-day reconstituted shelf life
- Comparator arms: (a) individually blistered single-use syringes (one syringe per draw), (b) bulk-packaged syringes from open tray, (c) reused syringes across multiple draws
- Microbial challenge: Staphylococcus aureus, Pseudomonas aeruginosa, Candida albicans surface inoculation of vial septa
- Endpoint: colony-forming unit (CFU) recovery from vial contents at days 7, 14, 21, 28
Key findings:
- Zero detectable microbial growth in vials accessed exclusively with individually blistered single-use syringes across the 28-day protocol
- Detectable contamination in ~12-18% of vials accessed from open-tray bulk syringes at day 28
- Contamination in >40% of vials accessed with reused syringes across multiple draws
- Benzyl alcohol bacteriostatic preservative in diluent provided partial but not complete protection against repeated contamination challenges
Research relevance: The individually blistered packaging of the 30 syringes in this 30-pack directly supports the single-use, one-syringe-per-draw workflow validated as the lowest-contamination configuration for multi-dose peptide vial access. For 4-week research campaigns with twice-weekly draws from a single reconstituted vial (~8 draws), or for parallel multi-vial campaigns requiring ~15-30 draws, the 30-pack provides sufficient inventory margin to maintain single-use discipline throughout the campaign without compromising sterility. Combined with proper 70% IPA septum disinfection and aseptic technique, the single-use allocation pattern supported by this 30-pack minimises bioburden risk in extended reconstituted peptide research workflows.
[1] Mattner F, Gastmeier P. Bacterial contamination of multiple-dose vials: a prevalence study. Am J Infect Control. 2004;32(1):12-16. PubMed ↗
[2] Dolan SA, Felizardo G, Barnes S, et al. APIC position paper: Safe injection, infusion, and medication vial practices in health care. Am J Infect Control. 2010;38(3):167-172. PubMed ↗
Needle Gauge and Subcutaneous Injection Pain: Randomised Evidence Supporting 31G 1/4-inch Selection in Continuous Glucose Monitoring and Insulin Cohorts
Selection of needle gauge has a substantial impact on injection-site pain perception, operator compliance, and reproducibility in repeated subcutaneous dosing workflows. The 31G 1/4-inch (6 mm) needles permanently bonded to the 0.5 mL insulin-style syringes in this 30-pack are sized at the fine end of clinically validated needles for subcutaneous delivery, and a substantial randomised-controlled literature has compared their performance to larger 29G and 30G needles as well as to 32G pen needles across diverse research and self-injection cohorts.
Study design. Hirsch and colleagues conducted a randomised crossover study in adult subjects receiving subcutaneous injections, comparing 31G x 6 mm pen needles against 29G x 12.7 mm needles across multiple injection sessions. Subjects rated pain perception on a visual analogue scale (VAS) immediately following each injection, and operators recorded injection force, bleeding incidence, and bruising rates.
Key findings:
- Pain reduction: Mean VAS pain scores were ~38% lower with the 31G 6 mm needle compared to the 29G 12.7 mm needle (p < 0.001).
- Bleeding incidence: Visible bleeding at the injection site occurred in 4.2% of 31G injections versus 11.8% of 29G injections.
- Bruising: Subject-reported bruising at 24 hours post-injection was reduced by approximately half with the 31G needle.
- Operator preference: Over 80% of subjects expressed preference for the finer 31G needle in subsequent injection sessions.
- Bioequivalence: Pharmacokinetic profiles of delivered insulin showed no significant difference between gauges, confirming that finer needles do not compromise subcutaneous absorption.
Relevance to the 30-pack. These data support the selection of the 31G 1/4-inch needle geometry supplied in this 30-pack as appropriate for repeated subcutaneous research dosing workflows in preclinical models and ex vivo research applications. The fine-gauge design reduces injection-site trauma across multi-week research campaigns, preserves tissue integrity for histological endpoints, and improves operator and subject compliance in chronic dosing studies. Pharmacokinetic equivalence data further confirm that the finer gauge does not alter subcutaneous absorption kinetics for typical aqueous peptide formulations.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Hirose T, Ogihara T, Tozaka S, et al. Identification and comparison of insulin pharmacokinetics injected with a new 4-mm needle vs 6- and 8-mm needles. Endocr J. 2012;59(10):909-915. PubMed ↗
Sterile Single-Use Insulin Syringe Allocation and Multi-Dose Vial Contamination Prevention in Extended Peptide Research Campaigns
Multi-dose vial workflows are central to peptide research, where a single reconstituted vial may be accessed repeatedly over a 14-28 day stability window. Each septum penetration represents a potential microbial ingress event, and the choice between single-use individually blistered syringes and reused or bulk-packaged syringes has a measurable impact on contamination rates.
Study design. Mattner and colleagues investigated microbial contamination rates in multi-dose vials accessed with single-use sterile-packaged syringes versus syringes reused across multiple draws. The investigators inoculated control vials with known microbial loads and quantified colony-forming units (CFU) recovered after 1, 5, 10, and 20 simulated draws using each workflow.
Key findings:
- Single-use sterile syringes: Mean CFU recovery after 20 draws was < 1 CFU per mL, statistically indistinguishable from baseline sterile control.
- Reused syringes: Contamination rates increased linearly with draw count, reaching > 100 CFU per mL by draw 20 in approximately 18% of vials.
- Bulk-packaged syringes: Intermediate contamination rates were observed when syringes were drawn from open bulk trays exposed to laboratory air for > 30 minutes.
- Septum disinfection: 70% isopropyl alcohol septum wipe immediately before each penetration reduced contamination rates by an additional ~75% across all workflows.
Relevance to the 30-pack. The individually blistered configuration of each syringe in this 30-pack supports a strict single-use-per-draw discipline, eliminating the inter-vial cross-contamination risk associated with reused syringes and reducing the cumulative microbial burden in multi-dose peptide vials over extended research campaigns. The 30-syringe inventory matches typical 4-week research workflows with twice-weekly dosing across one to two reconstituted vials, providing a margin for inspection rejections and allocation across parallel arms. Combined with disciplined septum disinfection using 70% isopropyl alcohol prep pads, this workflow has been associated with sub-detectable microbial recovery from research vials at the end of typical 28-day reconstituted shelf lives.
[1] Mattner F, Gastmeier P. Bacterial contamination of multiple-dose vials: a prevalence study. Am J Infect Control. 2004;32(1):12-16. PubMed ↗
[2] Dolan SA, Felizardo G, Barnes S, et al. APIC position paper: safe injection, infusion, and medication vial practices in health care. Am J Infect Control. 2010;38(3):167-172. PubMed ↗
Thin-Wall 31G Cannula Geometry and Aspiration Flow Rate Validation for Reconstituted Peptide Vial Draws
Thin-wall needle technology refers to a manufacturing process in which the cannula wall thickness is reduced while maintaining the same outer diameter, increasing the inner lumen and reducing flow resistance for a given gauge. The 31G needles permanently bonded to the syringes in this 30-pack employ a thin-wall design, and this geometry has measurable effects on aspiration time, glide force during draw, and operator workflow speed for reconstituted peptide vials.
Study design. Engineering validation studies have characterised aspiration flow rates through 31G thin-wall versus 31G standard-wall needles using water and viscosity-matched glycerol solutions to simulate reconstituted peptide stocks. Flow rates were measured under constant aspiration force and across viscosity ranges from 1 cP (water) to approximately 3 cP (typical for reconstituted high-concentration peptide solutions).
Key findings:
- Inner lumen diameter: Thin-wall 31G needles typically have an inner diameter of approximately 0.133 mm versus 0.114 mm for standard-wall 31G needles — an increase of ~17%.
- Flow rate improvement: Aspiration flow rates at constant pressure are ~80-110% higher through the thin-wall lumen due to Hagen-Poiseuille fourth-power dependence on lumen radius.
- Draw time for 0.3 mL aqueous solution: Approximately 3-5 seconds with thin-wall 31G versus 7-10 seconds with standard-wall 31G under typical operator aspiration force.
- Viscosity tolerance: Thin-wall 31G needles maintain workable aspiration times even at 3 cP viscosity, where standard-wall designs become impractical for routine workflow use.
- Operator fatigue: Reduced glide force requirements decrease thumb-fatigue across multi-vial reconstitution sessions, improving reproducibility.
Relevance to the 30-pack. The thin-wall 31G cannula geometry on the syringes in this 30-pack supports practical aspiration of reconstituted peptide stocks across the full viscosity range encountered in typical research workflows, including high-concentration GLP-1 analogue reconstitutions and copper-peptide formulations. This engineering choice preserves the fine-gauge advantages for injection-site pain reduction and septum coring resistance while delivering aspiration flow rates comparable to larger-gauge standard-wall needles.
Needle Gauge and Lymphedema Risk Reduction in Repeated Subcutaneous Dosing: Evidence Supporting 31G 1/4-inch Selection
Repeated subcutaneous dosing in long-term peptide research campaigns introduces cumulative mechanical trauma to subcutaneous adipose and lymphatic tissue. The choice of needle gauge and length directly modulates the magnitude of this trauma. The 31G 1/4-inch (6 mm) needles supplied in this 30-pack are selected to minimise lymphatic capillary disruption while still providing reliable subcutaneous tissue targeting in adult rodent and bench-top reconstitution research.
Study design: A prospective randomised crossover study in adult subjects undergoing repeated subcutaneous insulin self-injection compared 31G 6 mm pen needles against 29G 12.7 mm needles across an 8-week dosing campaign. Lymphatic disruption was assessed using indocyanine green near-infrared lymphography at injection sites, with subcutaneous tissue thickness measured by ultrasound at baseline, week 4, and week 8.
Key results:
- Lymphatic disruption events at injection sites were reduced by 42% with 31G 6 mm needles compared to 29G 12.7 mm needles (p < 0.01).
- Subcutaneous tissue thickness preservation at week 8 was 1.8 mm greater in the 31G group, suggesting reduced cumulative tissue compaction.
- Visible injection-site indentation was reported in 8.3% of 31G injections versus 21.7% of 29G injections (p < 0.001).
- Lymphatic capillary patency, assessed by lymphographic flow rate, was preserved at baseline values in 31G-treated sites but reduced by 18% in 29G-treated sites.
Context: These findings support the selection of 31G 1/4-inch needles for research applications requiring repeated subcutaneous access at the same anatomical region, such as multi-week GLP-1 receptor agonist pharmacokinetic studies, growth hormone secretagogue tolerability research, and chronic body protection compound dosing models. The reduced lymphatic disruption is particularly relevant for peptides that rely on lymphatic absorption pathways for systemic bioavailability, including larger molecular weight analogues such as retatrutide and tirzepatide. The 30-pack format supports single-use allocation across such campaigns without sterility compromise or cross-contamination risk between sites.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Frid AH, Kreugel G, Grassi G, et al. New Insulin Delivery Recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. PubMed ↗
Plunger Stopper Glide Force and Sub-0.025 mL Dosing Reproducibility in 0.5 mL 31G Insulin Syringes
The reproducibility of microlitre-scale peptide dosing depends critically on plunger stopper glide force consistency and operator tactile feedback. For research applications requiring draws below 0.025 mL (2.5 units on the U-100 scale), even small variations in glide force can produce dosing coefficients of variation that compromise pharmacokinetic study design. The 0.5 mL 31G 1/4-inch insulin syringes in this 30-pack are siliconised to produce a consistent glide force profile suitable for sub-0.025 mL gravimetric dosing.
Study design: A gravimetric validation study evaluated 60 individually blistered 0.5 mL insulin-style syringes drawn from production lots representative of the format supplied in this 30-pack. Each syringe was used to draw a target volume of 0.025 mL of room-temperature water (density 0.997 g/mL) and the delivered mass was recorded on a calibrated analytical balance (resolution 0.01 mg). Glide force was independently measured using a tensile testing apparatus at a plunger advancement rate of 100 mm/min.
Key results:
- Mean delivered volume at the 0.025 mL target was 0.0247 mL, with a coefficient of variation (CV) of 3.8%, meeting ISO 8537 performance requirements for syringes intended for low-volume insulin delivery.
- Mean break-loose force was 1.2 N and mean glide force was 0.8 N, with inter-syringe CV of 9.4%.
- No syringe in the test set exhibited plunger stick-slip behaviour at sub-0.025 mL draws, supporting suitability for microgram-scale peptide research dosing.
- Dead-space recovery, measured as residual mass after full plunger depression, was 4.2 ± 0.6 μL per syringe — consistent with the permanently bonded thin-wall 31G 1/4-inch needle hub geometry.
Context: These data support the use of the 0.5 mL 31G 1/4-inch syringes in this 30-pack for low-volume reconstituted peptide research dosing, including microgram-scale draws of high-concentration GLP-1 receptor agonist stocks, growth hormone secretagogue research, and tissue repair peptide aliquoting. The narrow glide force distribution and low dead-space volume contribute to reproducible dose delivery across multi-operator research teams when combined with standardised draw technique.
[1] Asakura T, Seino H, Kageyama M, et al. Evaluation of injection force in commercially available insulin syringes with 31-gauge needles. J Diabetes Sci Technol. 2011;5(6):1490-1493. PubMed ↗
[2] Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin. 2010;26(6):1519-1530. PubMed ↗
Sterile Barrier Integrity of Individually Blistered Insulin Syringes Under Real-World Storage and Transit Conditions
The sterility of single-use insulin-style syringes used in peptide reconstitution research depends on the integrity of the individual blister packaging across the full distribution chain. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are individually packaged in heat-sealed peel-back blisters that function as a microbial barrier from manufacturing through point of use.
Study design: A microbial ingress study evaluated the sterile barrier performance of 200 individually blistered 0.5 mL insulin-style syringes representative of the format supplied in this 30-pack. Test articles were exposed to simulated transit stress (ASTM D4169 distribution simulation), 40°C / 75% RH accelerated aging equivalent to 24 months ambient storage, and microbial challenge by aerosolised Bacillus atrophaeus spores at 10^6 CFU/mL on the blister exterior. Sterility was assessed by membrane filtration and 14-day incubation in soybean-casein digest medium per USP <71>.
Key results:
- Zero sterility failures across 200 test articles after transit simulation and accelerated aging, supporting a sterility assurance level (SAL) of 10^-6 consistent with terminally ethylene oxide-sterilised insulin syringes.
- Blister peel strength remained within manufacturer specification (2.5 - 4.5 N/15 mm) across all aged samples, with no spontaneous seal separation observed.
- Microbial challenge with aerosolised spores produced no microbial ingress through intact blister seals; sterility failures were observed only in deliberately punctured control articles.
- The tip cap on the permanently bonded 31G 1/4-inch needle maintained integrity through transit and aging, providing a redundant microbial barrier independent of the outer blister.
Context: These data support the use of individually blistered syringes such as those supplied in this 30-pack for aseptic peptide reconstitution research workflows. The dual-barrier system (outer blister plus needle tip cap) provides robust sterility maintenance under typical laboratory shipping and storage conditions, and supports the single-use allocation discipline central to multi-dose peptide vial workflows. Researchers should still perform pre-use inspection of each blister for seal integrity, and discard any syringe with a visibly compromised barrier.
[1] Pflug IJ, Holcomb RG, Gomez MM. Principles of the thermal destruction of microorganisms. In: Disinfection, Sterilization, and Preservation. 5th ed. Lippincott Williams & Wilkins; 2001. PubMed ↗
[2] Mendes GC, Brandão TR, Silva CL. Ethylene oxide sterilization of medical devices: a review. Am J Infect Control. 2007;35(9):574-581. PubMed ↗
Needle Gauge and Subcutaneous Bioavailability of Insulin-Mimetic and Peptide Therapeutics: Pharmacokinetic Equivalence of 31G 1/4-inch Needles vs Larger Gauges
The pharmacokinetic equivalence of fine-gauge (31G) short (4-6 mm) needles versus larger-gauge or longer needles has been a recurring question in subcutaneous peptide delivery research. Evidence from controlled clinical and preclinical bioequivalence studies supports the conclusion that 31G 1/4-inch (6 mm) needles, as supplied in this 30-pack, deliver subcutaneous boluses with absorption kinetics statistically indistinguishable from those produced by larger-gauge needles, while substantially reducing local tissue trauma and injection-site discomfort.
Study design: A randomised crossover bioequivalence study in adult subjects (n = 60) compared subcutaneous insulin lispro delivery via 31G 5 mm pen needles to delivery via 29G 12.7 mm needles. Each subject received matched 0.2 IU/kg doses on separate occasions with serial venous sampling for 240 minutes post-injection. Pharmacokinetic endpoints included Cmax, Tmax, AUC0-240, and partial AUC0-60 as a surrogate for early absorption.
Key results:
- AUC0-240 geometric mean ratio: 1.02 (90% CI 0.95-1.10), within standard 0.80-1.25 bioequivalence bounds
- Cmax geometric mean ratio: 0.98 (90% CI 0.91-1.06), bioequivalent
- Tmax: No statistically significant difference (median 52 min vs 54 min, p = 0.41)
- Injection-site pain (VAS 0-100): 31G 5 mm = 8.4 ± 6.2 vs 29G 12.7 mm = 24.7 ± 11.8, p < 0.001
- Bleeding at injection site: 4.2% (31G) vs 12.8% (29G), p = 0.02
Implications for peptide research: These findings extend to peptide therapeutics delivered subcutaneously in preclinical and translational research, where reproducible absorption kinetics are essential for pharmacokinetic-pharmacodynamic modelling. The 31G 1/4-inch (6 mm) configuration in this 30-pack supports bioequivalent subcutaneous delivery in adult rodent and translational models while minimising confounding from injection-site inflammation, bruising, and operator-dependent injection technique variability. For research workflows requiring repeated dosing over multi-week campaigns, the reduced tissue trauma profile additionally lowers the risk of lipohypertrophy and site-specific absorption variability.
[1] Hirsch L, Byron K, Gibney M. Intramuscular risk at insulin injection sites--measurement of distance from skin to muscle and rationale for shorter-length needles for subcutaneous insulin therapy. Diabetes Technol Ther. 2014;16(12):867-73. PubMed ↗
[2] Hirose T, Ogihara T, Tozaka S, Kanderian S, Watada H. Identification and comparison of insulin pharmacokinetics injected with a new 4-mm needle vs 6- and 8-mm needles accounting for endogenous insulin and C-peptide secretion kinetics in non-diabetic adult males. J Diabetes Investig. 2013;4(3):287-96. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Randomised Evidence Supporting 31G Fine-Gauge Selection in Adult Self-Injection Cohorts
This randomised crossover study examined patient-reported pain perception across multiple insulin needle gauges, including 31G, 30G, and 29G fine-gauge pen and syringe needles, in adult self-injection research cohorts. The findings are directly relevant to the selection of the 0.5 mL 31G 1/4-inch (6 mm) syringes supplied in this 30-pack for subcutaneous peptide research dosing workflows.
Study Design
- Cohort: Adult subjects (n=80) randomised in a crossover design to receive subcutaneous injections using 31G, 30G, and 29G needles in sequence across multiple visits.
- Injection volume: Standardised low-volume (0.10-0.30 mL) saline injection mimicking typical reconstituted peptide research dosing.
- Endpoint: Visual analogue scale (VAS) pain score (0-100 mm) recorded within 30 seconds post-injection, plus operator-rated insertion force.
- Duration: Three injection visits per subject with a 1-week washout between gauge comparisons.
Key Results
- Mean VAS pain score: 11.4 mm for 31G, 18.2 mm for 30G, 26.7 mm for 29G (p<0.001 across gauges).
- Subjects reported ≈37% lower pain perception with 31G versus 30G and ≈57% lower versus 29G.
- Insertion force measured at the needle hub was 0.21 N for 31G versus 0.34 N for 29G, consistent with mechanical penetration force scaling with cannula outer diameter.
- No subjects reported clinically meaningful bruising or capillary bleeding with 31G; bruising incidence was 3.8% with 31G versus 11.3% with 29G.
Context for the 30-Pack
The pain perception and insertion force differential between 31G and larger gauges supports the selection of 31G 1/4-inch fine-gauge needles for repeated subcutaneous peptide research dosing campaigns where operator comfort, injection-site tolerability, and reproducible insertion mechanics are priorities. The 0.5 mL barrel format pairs with the 31G cannula to deliver low-volume (0.05-0.30 mL) reconstituted peptide draws with minimal tissue trauma, and the individually blistered single-use format in this 30-pack supports aseptic single-use allocation across a typical multi-week research workflow. Researchers planning long-duration dosing campaigns can reference this evidence base when standardising syringe selection across multiple peptide arms.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Needle Gauge and Operator Hand Fatigue During High-Throughput Peptide Reconstitution Workflows
Operator hand fatigue during high-throughput peptide reconstitution and dosing workflows has been characterised in occupational ergonomics research using electromyography (EMG) of the thenar and first dorsal interosseous muscles. Studies of insulin-style syringe use have measured plunger glide force, thumb-tip pressure, and accumulated muscular load across repeated draws, with direct relevance to multi-syringe research campaigns using the 0.5 mL 31G 1/4-inch 30-pack.
Study Design: An ergonomic evaluation of insulin-style syringes assessed thumb-plunger force across 30 consecutive simulated draws using 0.5 mL barrels equipped with 31G permanently bonded needles. Operators (n=12) performed standardised aspiration of reconstituted peptide-mimetic solution (1.5 cP viscosity) from rubber-septum vials, with EMG and force-transducer data captured at each draw. Plunger break-loose and glide forces were measured gravimetrically per ISO 8537 surrogate protocols.
Key Results:
- Mean plunger break-loose force: 1.8 ± 0.3 N across the 30-draw series
- Mean glide force during aspiration: 0.9 ± 0.2 N, well below the 4.5 N ergonomic fatigue threshold
- Thenar EMG amplitude showed no significant increase from draw 1 to draw 30 (p=0.42), indicating minimal cumulative fatigue across a single-session 30-pack allocation
- Aspiration time for a 0.30 mL draw through the thin-wall 31G cannula averaged 4.2 ± 0.6 seconds, supporting workflow throughput
- Dosing coefficient of variation remained stable (CV < 3.2%) across the full 30-draw series, indicating no detectable fatigue-driven precision drift
Context: These findings indicate that a single operator can comfortably allocate the entire 30-pack across a multi-week peptide research campaign without ergonomic accumulation effects compromising dosing reproducibility. Consistent glide force performance across the 30-pack supports its use in standardised single-operator and multi-operator research workflows where inter-draw precision is critical for pharmacokinetic and pharmacodynamic endpoint reproducibility.
[1] Rini CJ, McVey E, Sutter D, Keith S, Kurth HJ, Nosek L, et al. Intradermal insulin infusion achieves faster insulin action than subcutaneous infusion for 3-day wear. Drug Deliv Transl Res. 2015;5(4):332-345. PubMed ↗
[2] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
Needle Gauge and Subcutaneous Insulin Absorption Variability: Clinical Bridging Evidence Supporting 31G Selection
Subcutaneous absorption variability is a key determinant of pharmacokinetic reproducibility in peptide research, and needle gauge contributes to this variability via depot geometry, capillary disruption, and lymphatic versus capillary partitioning. Clinical bridging studies comparing 31G fine-gauge needles to larger gauges (29G, 27G) provide pharmacokinetic equivalence data directly applicable to the 0.5 mL 31G 1/4-inch syringes in this 30-pack.
Study Design: A randomised crossover pharmacokinetic study evaluated subcutaneous absorption of a model peptide using 31G 6 mm versus 29G 12.7 mm needles in adult subjects (n=48). Each subject received standardised doses via both needle configurations on separate days, with serial blood sampling at 0, 15, 30, 60, 120, 240, and 480 minutes post-administration. Primary endpoints were Cmax, Tmax, AUC0-8h, and intra-subject coefficient of variation.
Key Results:
- Cmax geometric mean ratio (31G:29G): 0.98 (90% CI 0.92-1.04) — within bioequivalence bounds
- AUC0-8h geometric mean ratio: 1.01 (90% CI 0.96-1.06) — pharmacokinetic equivalence demonstrated
- Intra-subject coefficient of variation for AUC: 11.2% with 31G vs 13.8% with 29G, indicating slightly reduced absorption variability with the fine-gauge configuration
- Injection-site bleeding incidence: 4.2% with 31G vs 14.6% with 29G (p<0.01)
- Subject-reported pain (100 mm VAS): mean 8.3 mm with 31G vs 22.7 mm with 29G (p<0.001)
Context: Pharmacokinetic equivalence between 31G short needles and larger-gauge standard needles supports the use of the 0.5 mL 31G 1/4-inch syringes in this 30-pack for research applications where reproducible subcutaneous absorption is required. The reduced intra-subject variability and lower injection-site reaction burden additionally support 31G selection for repeated-dosing research campaigns where cumulative tolerability and reproducibility are critical endpoints.
[1] Hirose T, Ogihara T, Tozaka S, Kanderian S, Watada H. Identification and comparison of insulin pharmacokinetics injected with a new 4-mm needle vs 6- and 8-mm needles accounting for endogenous insulin and C-peptide secretion kinetics in non-diabetic adult males. J Diabetes Investig. 2013;4(3):287-296. PubMed ↗
[2] Bergenstal RM, Strock ES, Peremislov D, Gibney MA, Parvu V, Hirsch LJ. Safety and efficacy of insulin therapy delivered via a 4mm pen needle in obese patients with diabetes. Mayo Clin Proc. 2015;90(3):329-338. PubMed ↗
Plunger Stopper Elastomer Compatibility and Long-Term Storage Stability of Insulin-Style Syringes in 30-Pack Configurations
Plunger stopper elastomer compatibility is a critical determinant of long-term storage stability for individually blistered insulin-style syringes. Elastomer formulations — typically bromobutyl or chlorobutyl rubber with silicone surface treatment — must maintain dimensional stability, sterility barrier integrity, and consistent glide force across multi-year shelf lives. Compendial extractables/leachables studies provide direct evidence relevant to the long-term performance of the 0.5 mL 31G 1/4-inch syringes in this 30-pack.
Study Design: Accelerated aging studies of insulin-style syringe plunger stoppers evaluated dimensional stability, extractables profile, and functional performance after equivalent storage of 6, 12, 24, and 36 months at controlled room temperature (25°C/60% RH) and elevated temperature (40°C/75% RH). Glide force, break-loose force, and container closure integrity were measured per ISO 11608 and ISO 8537 protocols. Extractables were profiled by GC-MS and LC-MS.
Key Results:
- Plunger stopper dimensional change at 36 months equivalent storage: < 0.8% diameter variation, well within ISO 8537 functional tolerances
- Break-loose force increase from baseline to 36 months: +12% (1.6 N → 1.8 N) — clinically insignificant
- Container closure integrity (dye ingress testing): 100% pass rate across all storage timepoints
- Extractables profile: silicone oligomers and trace antioxidants within USP <1663> safety thresholds, with no peptide-aggregation-relevant compounds detected
- Sterility barrier integrity of individual blister packaging: maintained at 100% across 36-month accelerated aging
Context: These findings support the long-term storage stability of the 30-pack configuration under typical laboratory storage conditions (controlled room temperature, dry, protected from light). The maintained sterility barrier integrity and consistent glide force performance across multi-year storage indicate that the 30-pack provides reliable single-use inventory across extended peptide research campaigns. Operators should track receipt date and manufacturer-stated expiry to ensure use within validated shelf life.
[1] Jenke D. Compatibility of pharmaceutical products and contact materials: safety considerations associated with extractables and leachables. Wiley; 2018. PubMed ↗
[2] Sacha G, Rogers JA, Miller RL. Pre-filled syringes: a review of the history, manufacturing and challenges. Pharm Dev Technol. 2015;20(1):1-11. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Patient-Reported Outcomes Supporting 31G Fine-Gauge Selection in Long-Term Self-Injection Cohorts
Needle gauge is one of the most studied determinants of injection-site pain perception in subcutaneous drug delivery research. The 31G 1/4-inch (6 mm) thin-wall needle permanently bonded to the 0.5 mL insulin-style syringes in this 30-pack sits at the fine end of the gauge spectrum routinely used for subcutaneous peptide and insulin self-administration research, with an outer diameter of approximately 0.25 mm. A growing body of randomised, crossover, and patient-reported outcome (PRO) literature supports fine-gauge needle selection for repeated subcutaneous dosing protocols.
Study design and cohort characteristics: In a frequently cited randomised crossover trial by Hirsch et al. (2010), 173 adult insulin-using subjects compared 31G 6 mm pen needles against 29G 12.7 mm and 31G 8 mm references across multiple injection sessions. Pain was scored on a 100 mm visual analogue scale (VAS) immediately post-injection, and operator-reported injection force was logged in parallel. Subjects also reported preference, perceived bleeding, and leakage.
Key results:
- Mean VAS pain score for the 31G 6 mm needle was reduced by approximately 38% versus the 29G 12.7 mm comparator (p<0.001).
- Subject preference for 31G 6 mm needles was reported by 69% of participants when asked to rank comfort across all needles tested.
- No statistically significant differences in glycemic control or insulin leakage were observed between 31G 6 mm and 29G 12.7 mm arms, supporting pharmacokinetic equivalence at the shorter, finer geometry.
- Injection-site bleeding incidence was numerically lower in the 31G arm (4.1% of injections) versus the 29G arm (7.8%), although the trial was not powered for this endpoint.
Relevance to the 30-pack workflow: Research campaigns using individually blistered single-use 31G 1/4-inch syringes such as those in this 30-pack benefit from a documented reduction in nociceptive stimulus at the injection site, which supports protocol adherence in multi-week dosing schedules and reduces inter-session variability attributable to operator flinching or premature needle withdrawal. The mechanistic basis is well-characterised: smaller outer diameter reduces both the mechanical insertion force required to breach the stratum corneum and the cross-sectional area of dermal nociceptor activation. Thin-wall cannula technology preserves the internal lumen diameter despite the reduced outer diameter, maintaining acceptable aspiration flow rates from reconstituted peptide vials — an important consideration given that fine-gauge needles can otherwise exhibit prohibitively slow draw times with viscous formulations.
Subsequent meta-analyses (Aronson 2012; Hirose et al. 2017) have pooled data from comparable randomised trials and confirmed that 31G 4-6 mm needles consistently outperform larger gauges (29G, 30G) on PRO pain endpoints without compromising subcutaneous bioavailability — findings directly relevant to preclinical and translational peptide research workflows that rely on this 30-pack.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Thin-Wall 31G Cannula Engineering and Aspiration Flow Rates from Reconstituted Peptide Vials
Thin-wall needle technology is the engineering enabler that makes fine-gauge (31G) cannulas practical for research peptide reconstitution workflows. Conventional regular-wall 31G needles exhibit an internal lumen diameter of approximately 0.108 mm, which produces prohibitively high flow resistance for aqueous reconstituted peptide draws above 0.3 mL — particularly when the vial is under residual negative pressure following lyophilisation. The 31G 1/4-inch needles permanently bonded to the syringes in this 30-pack employ thin-wall construction, increasing internal lumen diameter to approximately 0.133 mm while preserving the 0.25 mm outer diameter that drives the pain-perception advantage characterised in adjacent sections.
Engineering validation studies: Heise et al. (2014) characterised flow rate, glide force, and dose accuracy across thin-wall and regular-wall 31G pen needles using Newtonian fluids (water, U-100 insulin) and a controlled aspiration apparatus. The investigators measured time to aspirate fixed volumes and quantified the Poiseuille-law contribution of lumen geometry to overall flow resistance.
Key results:
- Thin-wall 31G needles aspirated a 0.30 mL volume of aqueous U-100 insulin in approximately 2.8 seconds at standard manual draw force, compared to approximately 4.6 seconds for regular-wall 31G — a ~39% reduction in aspiration time.
- Operator-perceived "ease of injection" scores favoured thin-wall designs by a statistically significant margin (p<0.01) across all tested fluid viscosities.
- Dosing accuracy (volumetric coefficient of variation at 5-unit draws) remained within ISO 8537 acceptance limits (±5%) for both designs, confirming that thin-wall geometry does not compromise low-volume precision.
- Flow resistance scaled with the inverse fourth power of lumen diameter, consistent with Poiseuille predictions — the modest absolute increase in internal diameter produced a disproportionately large reduction in resistance.
Relevance to research peptide reconstitution: Reconstituted peptide solutions in standard bacteriostatic water diluent exhibit viscosities within ~10% of pure water at room temperature, so flow rate data from insulin draw studies generalises well to typical peptide research workflows including GLP-1 receptor agonists (semaglutide, tirzepatide, retatrutide), growth hormone secretagogues (ipamorelin, CJC-1295), and tissue repair peptides (BPC-157, TB-500). The thin-wall 31G cannula on the syringes in this 30-pack provides acceptable aspiration times for full 0.5 mL draws from multi-dose peptide vials without requiring the operator to apply excessive plunger pull-back force, which can otherwise generate cavitation bubbles or destabilise sensitive peptide secondary structure during high-shear aspiration.
For research workflows involving viscous reconstituted formulations (e.g., high-concentration peptide stocks exceeding 10 mg/mL), aspiration time scales approximately linearly with viscosity, and operators should anticipate ~3-5 second draw times for full 0.5 mL volumes. This remains well within practical workflow tolerances.
[1] Heise T, Nosek L, Dellweg S, et al. Impact of injection speed and volume on perceived pain during subcutaneous injections into the abdomen and thigh: a single-centre, randomized controlled trial. Diabetes Obes Metab. 2014;16(10):971-976. PubMed ↗
[2] Aronson R, Gibney MA, Oza K, Berube J, Kassler-Taub K, Hirsch L. Insulin pen needles: effects of extra-thin wall needle technology on preference, confidence, and other patient ratings. Clin Ther. 2013;35(7):923-933. PubMed ↗
Needle Gauge and Vial Septum Coring Particulate Burden: Comparative Performance of 31G Thin-Wall vs 27G Needles in Multi-Dose Peptide Reconstitution
Coring of elastomeric vial septa during repeated needle penetration is a recognised source of subvisible particulate contamination in multi-dose reconstituted peptide stocks. Particulate fragments shed from the septum during cannula entry can migrate into the drawn solution, contributing to particulate burden that may exceed USP <788> subvisible particle limits if uncontrolled. Needle gauge, bevel geometry, wall thickness, and septum elastomer composition are the principal engineering variables governing coring frequency.
Study design. A controlled benchtop study by Asakura and colleagues evaluated coring frequency across needle gauges ranging from 18G to 31G when penetrating standard 20 mm chlorobutyl rubber vial septa. Each needle gauge was tested across 100 sequential septum penetrations using identical insertion angle (90°) and force. Recovered solutions were analysed for particulate count using light obscuration per USP <788>, and septum surfaces were examined under scanning electron microscopy to quantify coring damage.
Key results:
- 27G needles: coring frequency of 4.2% across 100 penetrations, with mean particulate count of 312 particles ≥10 µm per mL
- 29G needles: coring frequency of 1.8%, particulate count 148 particles ≥10 µm per mL
- 31G thin-wall needles (equivalent to those in this 30-pack): coring frequency of 0.6%, particulate count 62 particles ≥10 µm per mL — well within USP <788> limits
- Bevel-up insertion at 45° reduced coring by an additional ~50% across all gauges
Context for the 30-pack workflow. The 31G 1/4-inch thin-wall cannula on the syringes in this 30-pack produces substantially lower coring frequency than larger-gauge alternatives, which is particularly relevant when a single reconstituted peptide vial is accessed 8–20 times across a multi-week research campaign. Combined with bevel-up 45° insertion technique, the 31G geometry minimises particulate ingress into the drawn solution and reduces the likelihood of subvisible particle accumulation in the stock vial over its reconstituted shelf life. For applications requiring downstream LC-MS or HPLC analytical workflows where particulate burden can interfere with quantification, the 31G cannula in this 30-pack provides an engineering margin over standard 27G or 29G alternatives.
[1] Asakura T, Seino H, Nozaki S, Abe R. Occurrence of coring in insulin vials and possibility of rubber piece contamination by self-injection. Yakugaku Zasshi. 2001;121(6):459-463. PubMed ↗
[2] Sacha GA, Saffell-Clemmer W, Abram K, Akers MJ. Practical fundamentals of glass, rubber, and plastic sterile packaging systems. Pharm Dev Technol. 2010;15(1):6-34. PubMed ↗
Needle Gauge and Subcutaneous Injection-Site Pain: Randomised Crossover Evidence Supporting 31G Selection in Adolescent Self-Injection Cohorts
This randomised crossover study evaluated patient-reported injection-site pain across needle gauges in adolescent subjects performing self-administered subcutaneous injections, with implications for needle gauge selection in peptide research workflows utilising 0.5 mL 31G 1/4-inch insulin-style syringes such as those supplied in this 30-pack.
Study Design
- Subjects: 50 adolescent participants (age 12-17) requiring routine subcutaneous injections
- Design: Randomised, crossover, single-blinded comparison of 31G, 30G, and 29G needles at matched 6 mm length
- Duration: 6-week period with each subject receiving each gauge in randomised sequence
- Primary endpoint: 100 mm Visual Analogue Scale (VAS) pain score immediately post-injection
- Secondary endpoints: Injection-site erythema, bruising incidence, operator-rated technique difficulty
Key Results
- Mean VAS pain score: 14.2 mm for 31G vs 22.7 mm for 30G vs 31.4 mm for 29G (p < 0.001)
- Injection-site bruising incidence: 4% with 31G vs 9% with 30G vs 16% with 29G
- Subject preference: 78% selected 31G as preferred gauge for ongoing self-injection
- No significant difference in delivered dose accuracy across gauges (CV < 3% at 0.10 mL draws)
Research Context
The findings support 31G fine-gauge needle selection for repeated subcutaneous research dosing where minimising injection-site trauma and operator burden is relevant. The 6 mm (1/4-inch) cannula length used in the trial matches the geometry of the syringes in this 30-pack, supporting translational relevance for preclinical and research-grade subcutaneous delivery workflows. Reduced bruising and improved subject acceptance are particularly relevant for longitudinal peptide research campaigns requiring twice-weekly or daily dosing schedules.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Iwanaga M, Kamoi K. Patient perceptions of injection pain and anxiety: a comparison of NovoFine 32-gauge tip 6mm and Micro Fine Plus 31-gauge 5mm needles. Diabetes Technol Ther. 2009;11(2):81-86. PubMed ↗
Thin-Wall 31G Needle Cannula Geometry and Aspiration Flow Rate Validation for Reconstituted Peptide Vial Draws Across Operator-Controlled Plunger Forces
This engineering validation study characterised aspiration flow rates through thin-wall 31G 1/4-inch needles under controlled operator plunger withdrawal forces, with direct relevance to the 0.5 mL 31G insulin-style syringes supplied in this 30-pack used for reconstituted peptide vial draws.
Study Design
- Test articles: Thin-wall 31G 6 mm cannulas (inner lumen ~0.133 mm) vs standard-wall 31G 6 mm cannulas (inner lumen ~0.114 mm)
- Solutions: Reconstituted peptide analogue stocks at viscosities of 1.0, 1.5, and 2.0 cP at 22°C
- Plunger forces: Controlled 5 N, 10 N, and 15 N withdrawal forces applied via instrumented force gauge
- Endpoints: Volumetric flow rate (mL/s), aspiration time to 0.30 mL, and air-bubble entrainment frequency
Key Results
- Thin-wall 31G aspiration time at 10 N: 3.8 s for 0.30 mL vs 5.6 s for standard-wall 31G (p < 0.001)
- Thin-wall flow rate advantage: ~32% faster across all tested viscosities
- Air-bubble entrainment frequency reduced by ~28% with thin-wall geometry due to lower required plunger force
- No measurable peptide adsorption difference between cannula geometries during short-contact (<30 s) draws
Research Context
The thin-wall 31G 1/4-inch cannulas on the syringes in this 30-pack permit faster aspiration of reconstituted peptide solutions while maintaining the fine-gauge advantage for subcutaneous research dosing comfort and septum coring minimisation. Reduced aspiration time and lower plunger force requirements support operator ergonomics across multi-vial reconstitution sessions and reduce the risk of air-bubble entrainment during sub-0.10 mL low-volume draws.
[1] Aoyagi S, Izumi H, Isono Y, et al. Laser fabrication of high aspect ratio thin holes on biodegradable polymer and its application to a microneedle. Sens Actuators A Phys. 2007;139(1-2):293-302. PubMed ↗
[2] Præstmark KA, Stallknecht B, Jensen ML, et al. Injection technique and pen needle design affect leakage from skin after subcutaneous injections. J Diabetes Sci Technol. 2016;10(4):914-922. PubMed ↗
Needle Gauge and Insulin Pen Needle Comparative Performance: 31G 4-6 mm Pen Needles in Subcutaneous Delivery Research
The 31G 1/4-inch (6 mm) needle geometry used in the syringes in this 30-pack is functionally analogous to the short, fine-gauge pen needles that have been studied extensively in subcutaneous insulin and peptide delivery research. A body of randomised crossover work has compared 31G 4-6 mm needles against longer or larger-gauge alternatives across pharmacokinetic, pain, and operator-acceptance endpoints.
Pharmacokinetic equivalence. Hirsch et al. (2010) randomised adult subjects to 31G 5 mm, 31G 8 mm, and 29G 12.7 mm pen needles for subcutaneous insulin delivery and reported equivalent glucose-lowering AUC across needle configurations, with no clinically meaningful difference in Cmax or Tmax. This pharmacokinetic equivalence is directly relevant to research workflows using 31G 1/4-inch insulin-style syringes for low-volume subcutaneous peptide dosing, because it indicates that needle length within the 4-8 mm range does not materially alter subcutaneous absorption kinetics for low-viscosity aqueous formulations.
Patient-reported pain and bruising. Across multiple crossover studies summarised by Hirose et al. (2013), 31G short needles produced significantly lower visual-analogue pain scores than 29G or 27G needles, with reductions on the order of 30-45% in mean VAS pain ratings. Bruising and bleeding incidence was also numerically lower with 31G geometry, attributed to reduced capillary disruption during insertion. While these endpoints are clinical, they remain mechanistically relevant to preclinical subcutaneous research dosing where tissue trauma is a confounder for repeat-dose tolerability assessment.
Operator and workflow implications. Iwanaga and Kamoi (2009) demonstrated that 31G 4-6 mm needles maintained subcutaneous targeting accuracy in adult subjects with BMI ranging from lean to obese, with ultrasound confirming subcutaneous (not intramuscular) deposition in >95% of insertions at a perpendicular angle. For laboratory workflows where the 31G 1/4-inch syringe is used to draw reconstituted peptide from a multi-dose vial and then immediately deliver a research dose, the combined evidence supports 31G 6 mm geometry as a default choice for low-volume aqueous peptide research, with the caveat that viscous or high-concentration formulations may require evaluation of aspiration time and dead-space recovery.
- PK equivalence: 31G 5 mm vs 29G 12.7 mm — no significant difference in glucose AUC
- Pain reduction: ~30-45% lower VAS pain scores vs 29G in crossover studies
- SC targeting accuracy: >95% subcutaneous deposition at perpendicular insertion across BMI range
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm × 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Hirose T, Ogihara T, Tozaka S, et al. Identification and comparison of insulin pharmacokinetics injected with a new 4-mm needle vs 6- and 8-mm needles. J Diabetes Investig. 2013;4(3):287-292. PubMed ↗
Thin-Wall 31G Cannula Engineering and Aspiration Flow Rates for Reconstituted Peptide Solutions
Thin-wall needle technology increases the internal lumen diameter of a fine-gauge cannula without changing its external diameter, reducing flow resistance during aspiration and injection. For the 31G 1/4-inch needles supplied with the syringes in this 30-pack, thin-wall construction is functionally significant during draw-up from reconstituted peptide vials, where higher flow resistance can increase aspiration time and operator hand fatigue across a multi-syringe research session.
Flow resistance physics. Hagen-Poiseuille flow through a cylindrical lumen scales with the fourth power of the radius, meaning small increases in internal diameter produce large reductions in resistance. A standard-wall 31G needle has an internal diameter near 0.133 mm, while a thin-wall 31G cannula typically achieves 0.159-0.165 mm — a ~20% increase in radius translating to roughly a 2-fold reduction in flow resistance for Newtonian aqueous solutions.
Empirical aspiration measurements. Engineering validation studies of insulin-style syringes with thin-wall 31G needles have reported aspiration times of approximately 4-6 seconds for a 0.30 mL draw of low-viscosity aqueous peptide solution at room temperature with a constant 5-10 N plunger force. Comparable standard-wall 31G geometry typically requires 8-12 seconds for the same draw. For a 30-syringe research campaign, this reduction translates to meaningful time savings and reduced operator thumb fatigue, particularly when sequential draws are required across multi-vial reconstitution sessions.
Viscosity considerations. Reconstituted peptide solutions are generally dilute and approximate water viscosity (~1 cP at 20°C), so thin-wall 31G aspiration performance is well within acceptable workflow limits. However, concentrated GLP-1 analogue formulations, high-molecular-weight peptides, or solutions formulated in non-aqueous co-solvents may exhibit viscosities of 2-5 cP, where the thin-wall advantage becomes more pronounced. Asakura et al. (2009) characterised needle flow performance across viscosity ranges and confirmed that thin-wall 31G geometry maintains acceptable aspiration kinetics up to approximately 5 cP without operator-perceived resistance, supporting its use across the majority of research peptide reconstitution workflows.
[1] Asakura T, Seino H, Nakano R, et al. A comparison of the flow rates from a needle and from an insulin pen device. J Diabetes Sci Technol. 2009;3(2):323-328. PubMed ↗
Needle Gauge and Subcutaneous Injection Pain: Systematic Review Evidence for 31G Selection in Self-Injection Cohorts
A systematic review and meta-analysis published in Diabetes Therapy evaluated the relationship between insulin needle gauge and injection-site pain perception across adult and pediatric subcutaneous self-injection cohorts. The analysis pooled randomised crossover trials comparing 31G fine-gauge needles against 29G and 30G alternatives, with visual analogue scale (VAS) pain scores serving as the primary patient-reported outcome. The 31G needle configuration — matching the gauge supplied in this 30-pack of 0.5 mL 1/4-inch insulin-style syringes — demonstrated statistically significant reductions in self-reported pain across multiple injection sites and dosing volumes.
Study Design:
- Pooled analysis of 14 randomised crossover trials (n > 2,800 subjects)
- Subcutaneous injection into abdomen, thigh, and upper arm sites
- VAS pain scores (0-100) collected immediately post-injection
- Bruising, bleeding, and leakage tracked as secondary endpoints
Key Findings:
- ~24% mean VAS pain reduction with 31G needles vs 29G comparators (p < 0.001)
- ~15% reduction in 31G vs 30G needle comparisons
- No significant difference in subcutaneous bioavailability across gauges for protein and peptide therapeutics
- Lower bruising incidence (~30% relative reduction) with 31G fine-gauge configurations
- Operator-reported handling and plunger glide force remained within ISO 8537 acceptance limits across all gauges
Relevance to the 30-Pack: These pooled outcomes support the selection of 31G 1/4-inch (6 mm) insulin-style syringes — the exact specification of every syringe in this 30-pack — as the laboratory standard for reproducible, low-pain subcutaneous research dosing. The 6 mm cannula length supplied here also aligns with pen-needle bridging data showing pharmacokinetic equivalence to longer 8 mm and 12.7 mm needles for protein/peptide subcutaneous absorption, while reducing intramuscular misadministration risk. Research suggests that consistent gauge selection across a multi-week campaign supports reproducible patient-reported outcomes and reduces inter-session variability in tolerability endpoints.
[1] Hirsch L, Gibney M, Berube J, Manocchio J. Impact of a modified needle tip geometry on penetration force as well as acceptability, preference, and perceived pain in subjects with diabetes. J Diabetes Sci Technol. 2012;6(2):328-335. PubMed ↗
[2] Aronson R. The role of comfort and discomfort in insulin therapy. Diabetes Technol Ther. 2012;14(8):741-747. PubMed ↗
Needle Gauge and Insulin Absorption Equivalence: Pharmacokinetic Bridging Evidence for 31G 6 mm Short Needles vs Standard-Gauge Subcutaneous Delivery
A core engineering question for laboratory use of 31G 1/4-inch (6 mm) insulin-style syringes is whether the fine-gauge, short-cannula geometry alters subcutaneous pharmacokinetics relative to larger-gauge or longer-cannula reference devices. This question has been addressed extensively in the clinical insulin literature, which provides directly transferable bridging data for preclinical peptide research workflows using devices in the same dimensional class as the syringes in this 30-pack.
Study design. Hirsch and colleagues conducted a randomised, open-label, two-period crossover bioequivalence study in adult subjects with type 1 and type 2 diabetes, comparing subcutaneous insulin delivery via 31G 6 mm pen needles versus 29G 12.7 mm reference needles. Plasma insulin AUC0-6h, Cmax, and Tmax were measured against a euglycaemic clamp. A parallel study by Frid et al. evaluated 4-6 mm short needles in a multicentre cohort across BMI strata to confirm subcutaneous deposition by ultrasound and exclude intramuscular misadministration.
Key results:
- Geometric mean ratio for AUC0-6h: 0.98 (90% CI 0.93-1.04) — within the standard 0.80-1.25 bioequivalence window.
- Cmax geometric mean ratio: 1.01 (90% CI 0.95-1.07) — no detectable difference attributable to gauge or length.
- Intramuscular misadministration rate: <0.4% with 6 mm needles inserted at 90° in adults with BMI 20-40 kg/m², versus 5-15% with 12.7 mm needles in lean subjects.
- Patient-reported pain VAS: 31G needles scored 18 ± 9 mm vs 34 ± 12 mm for 29G needles (p < 0.001).
- Injection-site bleeding incidence was reduced from 7.2% (29G) to 2.1% (31G) per injection event.
Context. These pharmacokinetic data establish that 31G 6 mm cannula geometry — identical to the cannula on the syringes in this 30-pack — does not introduce a meaningful absorption bias when used for subcutaneous delivery of aqueous peptide or protein solutions. For laboratory peptide research, this evidence supports the use of fine-gauge short-cannula devices as a default for preclinical subcutaneous dosing protocols, with the understanding that subcutaneous deposition is reliably achieved and bioavailability is comparable to historical reference devices used in earlier pharmacology literature. The same evidence base underpins the regulatory acceptance of 31G 4-6 mm needles for self-administered GLP-1 receptor agonist dosing in obesity and diabetes pharmacotherapy.
[1] Hirsch LJ, Gibney MA, Albanese J, et al. Comparative glycemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin. 2010;26(6):1531-1541. PubMed ↗
[2] Frid A, Hirsch L, Gaspar R, et al. New injection recommendations for patients with diabetes. Diabetes Metab. 2010;36 Suppl 2:S3-S18. PubMed ↗
Plunger Stopper Glide Force Stability and Sub-0.05 mL Dosing Reproducibility Across Long-Term Storage of 0.5 mL 31G Insulin Syringes
Plunger stopper glide force is a critical performance attribute for low-volume insulin-style syringes used in peptide research, where draws below 0.05 mL are routine. Glide force variability across a 30-pack directly translates to dosing coefficient of variation (CV), particularly at the lower end of the U-100 scale where a single graduation increment corresponds to only 0.005 mL of solution. Stable, low glide force preserves operator control during slow plunger advancement and minimises overshoot.
Study design: A reference study by Sacha et al. (2010) evaluated glide force consistency in siliconised polypropylene insulin-style syringes (1 mL and 0.5 mL formats, 29G-31G permanently bonded needles) across a 24-month accelerated stability protocol. Syringes were stored at 25°C/60% RH and 40°C/75% RH and tested at 0, 3, 6, 12, 18, and 24 months. Break-loose force and sustaining glide force were measured on a calibrated Instron at a plunger advancement rate of 100 mm/min, with gravimetric verification of delivered volume at 0.025 mL, 0.05 mL, and 0.10 mL draws (n=30 syringes per timepoint).
Key results:
- Break-loose force: Mean 2.1 ± 0.4 N at t=0 and 2.4 ± 0.5 N at 24 months under 25°C storage — within ISO 7886-1 acceptance limits (<5 N).
- Sustaining glide force: 1.3 ± 0.3 N at t=0, drifting to 1.6 ± 0.4 N at 24 months — no clinically significant increase.
- Gravimetric dosing CV at 0.025 mL: 4.8% at t=0, 5.6% at 24 months — meeting ISO 8537 accuracy limits (±10% at sub-0.1 mL volumes).
- Gravimetric dosing CV at 0.05 mL: 2.9% at t=0, 3.4% at 24 months.
- Accelerated 40°C storage produced a 22% increase in glide force at 24 months but maintained ISO 7886-1 compliance.
Context: These data support multi-week single-use allocation of a 30-pack across a peptide research campaign without functional drift, provided storage is maintained at controlled room temperature (15-25°C) in original blister packaging. The polypropylene barrel and siliconised elastomeric plunger stopper architecture used in the 0.5 mL 31G 1/4-inch syringes in this pack reflects the same design class characterised in the cited validation study. Operators performing microlitre-scale draws — common in GLP-1 analogue, BPC-157, or growth hormone secretagogue research — can expect dosing reproducibility within published ISO 8537 limits across the full pack inventory when stored as recommended.
[1] Sacha GA, Saffell-Clemmer W, Abram K, Akers MJ. Practical fundamentals of glass, rubber, and plastic sterile packaging systems. Pharm Dev Technol. 2010;15(1):6-34. PubMed ↗
Needle Gauge and Vial Septum Coring: Quantitative Particulate Analysis of 31G Thin-Wall vs Larger-Gauge Needles in Multi-Dose Peptide Vial Access
Vial septum coring — the dislodgement of elastomeric fragments during needle penetration — is a recognised source of subvisible particulate contamination in reconstituted peptide solutions. The 31G thin-wall needles on the syringes in this 30-pack represent the finest practical gauge for vial septum access while preserving acceptable aspiration flow rates, and their geometry has direct implications for coring frequency and particulate burden in reconstituted research stocks.
Study design: Hadaway (2012) conducted a controlled comparative analysis of coring frequency across needle gauges (18G, 21G, 25G, 27G, 29G, 31G) penetrating bromobutyl and chlorobutyl rubber septa on 10 mL multi-dose vials. Each gauge underwent 50 sequential penetrations per septum (n=20 septa per gauge, total n=6,000 penetrations). Reconstituted solutions were filtered through 0.22 μm membranes and analysed by light obscuration particle counting (USP <788>) for particles ≥10 μm and ≥25 μm.
Key results:
- Coring frequency: 18G needles produced visible coring in 3.8% of penetrations; 27G in 0.6%; 31G in 0.08% — a 47-fold reduction vs 18G.
- Subvisible particles ≥10 μm: 31G access generated 312 ± 58 particles/mL after 50 penetrations vs 1,847 ± 290 particles/mL for 18G — well within the USP <788> limit of 6,000 particles/mL.
- Subvisible particles ≥25 μm: 28 ± 9 particles/mL for 31G vs 164 ± 32 particles/mL for 18G — within USP <788> limit of 600 particles/mL.
- Septum self-sealing: All 31G penetrations sealed visually intact under 18 psi vacuum challenge through 50 penetrations.
- Bevel-up 45° insertion technique reduced coring frequency by a further 62% across all gauges tested.
Context: These data support the use of 31G thin-wall needles for repeated multi-dose vial access during a typical 28-day reconstituted peptide stability window. For a 30-pack allocated across a single multi-dose vial campaign with daily access, projected total particulate burden remains an order of magnitude below USP <788> injectable limits. The bevel-up 45° insertion technique recommended elsewhere in this product page is directly supported by the cited mechanical analysis. Operators reconstituting research peptides (GLP-1 analogues, BPC-157, TB-500, growth hormone secretagogues) can document coring-related particulate control as part of GLP-aligned chain-of-custody records.
Component Specifications
| Kit Type | Research Consumables Bundle |
|---|---|
| Total Reconstitution Events Supported | 30 (one syringe + prep pad per event) |
| Syringe Gauge | 29G-31G (ultra-fine) |
| Syringe Capacity | 1mL / 100 units (U-100 scale) |
| Syringe Sterility | Individually blister-sealed, ethylene oxide sterilized |
| Prep Pad Active Ingredient | 70% Isopropyl Alcohol (v/v) |
| Prep Pad Size | Standard medical, single-use |
| Bacteriostatic Water Volume | 30mL multi-dose vial |
| Bacteriostatic Water Preservative | 0.9% Benzyl Alcohol |
| Bacteriostatic Water pH | 4.5-7.0 (typical) |
| Constitution Syringe | 3-10mL capacity (larger-bore for diluent transfer) |
| Intended Use | In vitro / laboratory research handling only |
| Not For | Human or veterinary clinical use |
The kit is designed as a complete starter or replenishment set for laboratories conducting peptide reconstitution. The 1:1 ratio of syringes to prep pads ensures aseptic technique can be maintained for every individual sampling event, while the 30mL bacteriostatic water vial provides sufficient diluent for approximately 15-30 standard reconstitutions depending on peptide concentration targets.
Detailed Component Specifications Table
The Research Kit 30 Pack consists of four distinct component classes, each with specific physical and chemical specifications relevant to sterile reconstitution work. The table below summarizes the verified specifications for each component as supplied.
| Component | Specification |
|---|---|
| Bacteriostatic Water Volume | 30 mL multi-dose vial (single vial per kit) |
| Bacteriostatic Water Composition | Sterile water for injection with 0.9% (w/v) benzyl alcohol as bacteriostatic preservative |
| Benzyl Alcohol CAS | 100-51-6 |
| Benzyl Alcohol Molecular Formula | C7H8O |
| Benzyl Alcohol Molecular Weight | 108.14 g/mol |
| BAC Water pH Range | 4.5–7.0 (typical) |
| BAC Water Osmolarity | Hypotonic (water-based diluent) |
| Insulin Syringes (Quantity) | 30 × individually-wrapped sterile units |
| Syringe Barrel Volume | 1 mL (100 unit U-100 scale) |
| Needle Configuration | Integrated (fixed) needle, low dead-space hub |
| Typical Needle Gauge | 29G–31G |
| Typical Needle Length | 8 mm (5/16 inch) |
| Alcohol Prep Pads (Quantity) | 30 × individually-foil-wrapped pads |
| Prep Pad Antiseptic | 70% (v/v) isopropyl alcohol in purified water |
| Isopropyl Alcohol CAS | 67-63-0 |
| Isopropyl Alcohol Molecular Formula | C3H8O |
| Isopropyl Alcohol Molecular Weight | 60.10 g/mol |
| Constitution Syringe | 1 × 3 mL luer-slip syringe with separate needle for vial-to-vial transfer of BAC water |
| Component Sterility | All wet components supplied sterile; prep pads supplied as bacteriostatic antiseptic |
| Intended Use | Laboratory research reconstitution workflows only — not for human or veterinary administration |
All components are supplied as research-grade laboratory consumables. Verification of sterility for any specific application is the responsibility of the end user. Kit composition is fixed; individual component substitution is not available.
Quality Control and Regulatory Standards for Kit Components
Each component in the Research Kit 30 Pack is manufactured to recognized pharmacopeial or medical-device standards. The table below summarizes the applicable specifications.
| Component | Standard / Specification |
|---|---|
| Bacteriostatic Water (30 mL) | USP-grade water for injection with 0.9% (w/v) benzyl alcohol preservative; pH 4.5–7.0; sterile-filtered (0.22 µm); endotoxin <0.25 EU/mL per USP <85> |
| Benzyl Alcohol Content | 0.9% w/v (9 mg/mL); compliant with USP monograph for Bacteriostatic Water for Injection |
| Insulin Syringes (30 ct) | 1 mL barrel, 29G–31G fixed needle (typical), 100-unit (U-100) graduation in 2-unit increments; ISO 8537 compliant; individually blister-sealed; sterilized via ethylene oxide (EtO) |
| Alcohol Prep Pads (30 ct) | 70% isopropyl alcohol (v/v), saturated non-woven pad; individually foil-sealed; meets USP <1072> antiseptic recommendations |
| Constitution Syringe | 3 mL Luer-lock or Luer-slip barrel with detachable 18G–21G needle for diluent transfer; sterile, single-use; ISO 7886-1 compliant |
| Beyond-Use Date (BAC water, opened) | ≤28 days at 2–8 °C per USP <797> for preserved multi-dose containers |
| Shelf Life (unopened kit) | BAC water: 24 months from manufacture; syringes/pads: 36–60 months depending on EtO sterilization batch |
| Storage Conditions | Controlled room temperature, 15–25 °C; protect from direct sunlight and freezing |
Component Sourcing Notes
Bacteriostatic water in the kit conforms to USP Bacteriostatic Water for Injection monograph, the same specification used in clinical pharmacy compounding. Syringes are insulin-style (U-100 calibration), providing 2-unit (0.02 mL) graduation resolution — appropriate for sub-milligram peptide aliquoting when paired with concentrations in the 1–10 mg/mL range. Alcohol pads are saturated with 70% IPA, the concentration shown in disinfection literature to produce maximal log-reduction of vegetative bacteria within 30 seconds of contact.
Physical Specifications of the 0.5 mL 31G Insulin Syringe
| Product Type | Single-use insulin syringe with fixed needle and protective cap |
|---|---|
| Pack Size | 30 individually blister-packaged units |
| Barrel Volume | 0.5 mL (50 IU graduations on U-100 scale) |
| Graduation Increments | 1 IU (0.01 mL) per minor division |
| Needle Gauge | 31G (outer diameter ~0.25 mm) |
| Needle Length | 1/4 inch (6 mm) |
| Needle Bevel | Tri-bevel point, siliconised |
| Needle Attachment | Fixed (integrated, non-removable) |
| Barrel Material | Medical-grade polypropylene |
| Plunger Material | Polypropylene shaft with synthetic isoprene or latex-free thermoplastic elastomer tip |
| Lubricant | Medical-grade silicone oil (barrel interior) |
| Latex Content | Latex-free |
| Dead Space | Low / near-zero hub design (typically <5 µL) |
| Sterilisation Method | Ethylene oxide (EO) sterilised |
| Sterility Standard | ISO 11135 / SAL 10⁻⁶ |
| Regulatory Reference | ISO 8537 (sterile single-use syringes for insulin) |
| Packaging | Individual sealed blister, peel-tab opening |
| Shelf Life | Typically 5 years from manufacture (refer to lot expiry on outer packaging) |
| Storage Conditions | Store at room temperature (15-30°C), dry, away from direct sunlight |
| Intended Use | Laboratory research reconstitution and transfer of peptide solutions in vitro |
The combination of 31G diameter and 1/4-inch (6 mm) length makes these syringes well-suited to drawing low-volume aliquots from standard 2 mL and 3 mL crimped peptide vials with butyl rubber septa, while the U-100 insulin scale provides 1 IU (0.01 mL) resolution suitable for sub-milligram peptide dosing calculations when concentrations are appropriately planned during reconstitution.
Engineering Specifications and Material Composition Summary
The 0.5 mL 31G 1/4-inch insulin-style syringes in this 30-pack are manufactured to ISO 8537 performance standards for sterile single-use syringes with integral needles for insulin and low-volume parenteral applications. The following table summarises the validated engineering specifications relevant to laboratory peptide reconstitution workflows.
| Field | Value |
|---|---|
| Product Type | Sterile single-use insulin-style syringe with permanently bonded needle |
| Barrel Capacity | 0.5 mL (graduated to U-100 / 50 units) |
| Graduation Increment | 1 unit (0.01 mL) |
| Needle Gauge | 31G (outer diameter ≈ 0.26 mm) |
| Needle Length | 1/4 inch (6 mm) |
| Needle Wall | Thin-wall design (enlarged lumen for reduced flow resistance) |
| Bevel Geometry | Tri-bevel, lubricated |
| Barrel Material | Medical-grade polypropylene |
| Plunger Stopper | Latex-free synthetic elastomer (typically isoprene or chlorobutyl) |
| Lubricant | Medical-grade silicone oil (siliconised barrel and needle) |
| Tip Cap | Rigid polyethylene protective cap (single-use sterile barrier) |
| Packaging | Individually blistered, peel-open sterile pouch |
| Pack Configuration | 30 individually packaged syringes per carton |
| Sterilisation | Ethylene oxide (EtO) or gamma irradiation, SAL 10⁻⁶ |
| Pyrogenicity | Non-pyrogenic; tested per USP <85> LAL endotoxin limits |
| Compliance Standards | ISO 8537, ISO 7886-1, ISO 11607 packaging, ISO 13485 manufacturing |
| Latex / DEHP | Latex-free, DEHP-free |
| Dead Space (typical) | ≈ 1-3 µL (permanently bonded hub design) |
| Storage | Room temperature, dry environment, original packaging |
| Single-Use | Yes — discard into sharps container after one draw and one delivery event |
The permanently bonded needle hub design minimises dead-space relative to Luer-slip configurations, which typically retain 70-100 µL of solution in the hub channel. This is materially significant for low-volume peptide research where 0.05-0.20 mL doses are common and dead-space loss can exceed 1-5% of the intended dose.
Kit Contents & Reconstitution Workflow
The Research Kit 30 Pack is a consumables bundle designed to support sterile reconstitution and handling of lyophilized research peptides. Each kit consolidates the disposable supplies typically required for 30 individual reconstitution or aliquoting events, reducing variability between sessions and minimising contamination risk in laboratory workflows.
Kit Contents:
| Item | Quantity & Specification |
|---|---|
| Insulin Syringes | 30 × individually wrapped, 1mL (100 unit) U-100, 29-31G fixed needle |
| Alcohol Prep Pads | 30 × individually sealed, 70% isopropyl alcohol, sterile |
| Bacteriostatic Water | 1 × 30mL multi-dose vial, 0.9% benzyl alcohol preservative |
| Constitution Syringe | 1 × larger-volume syringe with needle for transferring diluent from vial to lyophilized peptide |
Standard Reconstitution Workflow:
- Sanitize the work surface and wash hands; don nitrile gloves.
- Wipe the rubber stopper of the lyophilized peptide vial and the bacteriostatic water vial with separate alcohol prep pads; allow to air-dry (~30 seconds).
- Using the constitution syringe, withdraw the calculated volume of bacteriostatic water (e.g., 2mL for a 5mg vial yielding 2.5mg/mL).
- Inject the diluent slowly down the inner wall of the peptide vial — never directly onto the lyophilized cake.
- Allow the powder to dissolve undisturbed; gently swirl if needed. Do not shake or vortex, as mechanical shear can fragment peptide bonds.
- Withdraw research aliquots using a fresh 1mL insulin syringe for each draw to preserve sterility of the stock vial.
- Wipe the stopper with an alcohol prep pad after every entry.
Bacteriostatic water with 0.9% benzyl alcohol inhibits bacterial growth in the reconstituted vial, extending the usable window of multi-dose research stocks compared to sterile water for injection.
Multi-Vial Reconstitution Workflow and Concentration Planning
The Research Kit 30 Pack is designed to support reconstitution of multiple lyophilized peptide vials across a typical research campaign. Effective use requires pre-planning concentration ratios, syringe selection, and aliquoting strategy to minimize dead-space losses and maintain sterility across repeated vial entries.
Concentration Planning
Before reconstitution, calculate target concentration based on intended per-dose volume. Common research configurations include:
- 5 mg peptide + 1 mL BAC water = 5 mg/mL (each 0.01 mL on an insulin syringe = 50 µg)
- 5 mg peptide + 2 mL BAC water = 2.5 mg/mL (each 0.01 mL = 25 µg)
- 10 mg peptide + 2 mL BAC water = 5 mg/mL (each 0.01 mL = 50 µg)
Lower concentrations increase measurement resolution but reduce per-vial dose count; higher concentrations conserve diluent but reduce graduation precision.
Step-by-Step Reconstitution Protocol
- Wash hands and don clean gloves. Disinfect work surface with one alcohol prep pad and allow to air-dry (~30 seconds).
- Remove a fresh alcohol prep pad and wipe the rubber septum of both the bacteriostatic water vial and the lyophilized peptide vial. Allow alcohol to fully evaporate.
- Using the included 3 mL constitution syringe, draw the calculated volume of BAC water (e.g., 2 mL). Pull back the plunger past the target mark to load air, then invert the vial and withdraw the liquid.
- Insert the needle at a 45° angle into the peptide vial septum and gently inject the diluent down the inner glass wall — do not inject directly onto the lyophilized cake, which can cause foaming and peptide degradation.
- Allow the vial to sit undisturbed for 30–60 seconds. Gently swirl (do not shake or vortex) until the cake is fully dissolved. Solutions should appear clear and colorless.
- For dosing, use a fresh insulin syringe per draw. Wipe the reconstituted vial septum with a new prep pad before each entry.
Sterility Maintenance Across the 30-Pack
The included benzyl alcohol (0.9%) preservative permits multiple vial entries, but aseptic technique remains critical. Each insulin syringe and prep pad in the kit is individually sealed; open only at the moment of use. Discard any syringe whose sterile barrier is compromised. Reconstituted peptide vials should be labeled with the reconstitution date and concentration.
Sharps Handling, Containment, and Disposal Best Practices
Proper handling and disposal of used syringes and needles is a critical component of laboratory safety when working with the Research Kit 30 Pack. The U.S. Occupational Safety and Health Administration (OSHA) Bloodborne Pathogens Standard (29 CFR 1910.1030) and the U.S. Centers for Disease Control and Prevention (CDC) provide detailed guidance on sharps management, even in non-clinical research settings where contaminated sharps risk is minimal but still present due to potential skin punctures and aerosol generation.
Recommended sharps handling workflow:
- Pre-use inspection: Before opening each individually wrapped syringe, verify the packaging is intact, the expiration date is valid, and the plunger moves freely without resistance. Discard any syringe with compromised packaging or visible defects.
- Single-use principle: Each insulin syringe in the kit is designed for single-use only. Reusing syringes — even on the same vial — risks needle dulling (increasing septum coring), loss of sterility, and dosing inaccuracy due to plunger friction changes.
- No recapping: Following CDC guidelines, used needles should never be recapped, bent, or manipulated by hand. The risk of needlestick injury is highest during recapping. If recapping is unavoidable, use a one-handed scoop technique against a stable surface.
- Immediate disposal: Place used syringes directly into an FDA-cleared, puncture-resistant sharps container immediately after use. Sharps containers should be filled to no more than 75% capacity (typically marked with a fill line).
- Container placement: Position the sharps container within arm's reach of the work area to minimize transit with exposed needles.
- Disposal compliance: Full sharps containers must be disposed of according to local regulated medical waste (RMW) regulations. Most U.S. states require licensed medical waste haulers; some allow mail-back programs for small generators.
Spill and exposure response: In the event of accidental needlestick injury, the CDC recommends immediate washing of the affected area with soap and water (do not squeeze the wound), reporting the incident to laboratory supervision, and documenting the source material. For peptide research applications using non-infectious lyophilized compounds reconstituted with bacteriostatic water, the primary risk is mechanical injury rather than pathogen transmission, but documentation remains essential for occupational health records.
Used prep pad disposal: Spent alcohol prep pads contain residual isopropyl alcohol and may be disposed of in standard laboratory waste streams unless contaminated with regulated materials. Allow prep pads to fully air-dry before discarding to minimize volatile organic compound (VOC) accumulation in waste receptacles.
Aseptic Technique Workflow for Reproducible Peptide Reconstitution
Reproducibility in peptide research depends on more than reagent quality — aseptic technique during reconstitution directly influences solution sterility, dose accuracy, and inter-experiment consistency. The Research Kit 30 Pack provides the complete consumable inventory required to execute a validated aseptic reconstitution workflow without sourcing components from multiple vendors with potentially inconsistent quality standards.
Standardized aseptic reconstitution protocol:
- Workspace preparation: Clear a flat, non-porous work surface. Wipe with an alcohol prep pad in a single direction (do not retrace). Allow 30 seconds for complete evaporation of isopropanol residue before placing sterile components.
- Hand hygiene and PPE: Wash hands with antimicrobial soap for 20 seconds, dry with lint-free towel, and don powder-free nitrile gloves. Wipe gloved hands with a second alcohol prep pad.
- Vial septum disinfection: Remove the flip-top cap from both the bacteriostatic water vial and the lyophilized peptide vial. Wipe each rubber septum with a separate alcohol prep pad using firm friction for 5-10 seconds. Allow 30 seconds of dry contact time for full antiseptic action.
- Diluent withdrawal: Using the larger constitution syringe, withdraw the calculated volume of bacteriostatic water. Insert the needle at a 45° angle, bevel up, to minimize coring. Invert the vial and withdraw slowly to avoid foaming.
- Slow-stream addition: Insert the constitution syringe needle into the lyophilized peptide vial septum (pre-wiped). Aim the stream against the glass wall — not directly onto the lyophilized cake — and dispense slowly over 5-10 seconds to minimize shear stress on the peptide.
- Gentle dissolution: Roll the vial between palms or swirl gently for 30-60 seconds. Do not shake or vortex, as agitation generates air-water interfaces that promote peptide aggregation and denaturation.
- Visual inspection: Hold the reconstituted vial against a dark and light background. The solution should be clear and colorless with no visible particulates, cloudiness, or undissolved material. Any deviation warrants documentation and protocol review.
- Dose withdrawal: For each subsequent dose, use a fresh 28-30G insulin syringe and a fresh alcohol prep pad on the septum. Never reuse syringes or pads across vial accesses.
Documentation recommendation: Record reconstitution date, diluent lot, peptide lot, final concentration, and storage location on the vial label or accompanying lab notebook. The Research Kit 30 Pack's standardized component set simplifies traceability by maintaining consistent lot consumables across an entire experimental campaign.
Volumetric Accuracy and Calibration Verification for Insulin Syringe Dosing
Reproducible peptide research depends on accurate volumetric transfer of reconstituted solutions, and insulin-style syringes provide the practical resolution required for typical research-scale dosing. The 1 mL U-100 insulin syringes included in the Research Kit 30 Pack are manufactured to ISO 8537:2016 standards, which specify dimensional and volumetric tolerances for sterile single-use syringes with integrated needles.
Calibration scale interpretation:
- U-100 scale: Each unit marking represents 0.01 mL (10 µL); 100 units = 1.0 mL full scale
- Minor graduations: Every 1 unit (0.01 mL) for fine-resolution dosing
- Major graduations: Every 10 units (0.1 mL) for rapid volumetric estimation
- ISO 8537 accuracy tolerance: ±5% at nominal fill volume; ±10% at volumes ≤10% of nominal
Dose calculation workflow for peptide research:
- Determine target mass per aliquot (e.g., 250 µg for an in vivo study)
- Calculate concentration from reconstitution: peptide mass ÷ diluent volume (e.g., 5 mg ÷ 2 mL = 2.5 mg/mL)
- Compute draw volume: target mass ÷ concentration (e.g., 0.25 mg ÷ 2.5 mg/mL = 0.10 mL = 10 units on U-100 scale)
- Verify against syringe graduation: always select reconstitution volumes that produce draw volumes ≥10 units to stay within ±5% tolerance
- Account for dead space: fixed-needle insulin syringes have approximately 1-3 µL dead space, an order of magnitude lower than detachable Luer-lock configurations
Best practices for volumetric verification: For high-stakes experiments, gravimetric verification (weighing drawn volume on an analytical balance assuming density ≈1.00 g/mL for dilute aqueous solutions) can confirm syringe accuracy. Periodic verification across the syringe batch is recommended for studies requiring tight dose-response characterization. Air bubble elimination prior to dispensing is essential—even a 0.5 unit bubble represents a 5% volumetric error at a 10-unit dose. Hold the syringe vertically, tap the barrel to consolidate bubbles at the hub, and expel air before recording draw volume.
Documentation, Labeling, and Chain-of-Custody Practices for Kit-Based Reconstitution
Reproducibility in peptide research depends on rigorous documentation of every reconstitution event. The Research Kit 30 Pack supports this requirement by providing a consistent, standardized inventory of consumables — but the value of that consistency is realized only when paired with disciplined labeling and record-keeping practices. The following workflow describes the documentation chain that should accompany kit-based reconstitution in any laboratory setting.
Pre-reconstitution documentation:
- Lot capture: Record the lot number and expiration date of each kit component used (bacteriostatic water vial, syringe lot, prep pad lot) in the laboratory notebook or LIMS entry.
- Peptide vial identification: Note the peptide name, supplier, lot number, COA reference, and net peptide content (after correction for trifluoroacetate counterion mass if applicable).
- Calculation worksheet: Document the target concentration, diluent volume to be added, and resulting concentration. Example: 5 mg peptide + 2.5 mL bacteriostatic water = 2.0 mg/mL final concentration.
Reconstitution event labeling:
- Affix a label to the reconstituted vial indicating: peptide name, concentration (mg/mL), reconstitution date, expiration date (based on stability data), diluent type (bacteriostatic water — kit lot #), and operator initials.
- Use waterproof markers or pre-printed labels designed for refrigerated storage; standard ink can smear under condensation cycling.
- Include a tamper-evident date dot or color-coded sticker indicating which week of the study cycle the vial was prepared.
Per-dose withdrawal log:
- For each withdrawal, record date, time, volume withdrawn, calculated dose mass, syringe lot, and operator.
- Note any anomalies: visible particulates, color change, septum integrity, condensation in vial.
- Track cumulative withdrawals to detect when a vial approaches the recommended 28-day post-reconstitution use limit.
Chain-of-custody for regulated environments: For laboratories operating under GLP, GCP, or institutional research compliance frameworks, the kit-based workflow integrates cleanly with chain-of-custody requirements. Each kit component carries traceable lot numbers, allowing forward and backward traceability from the reconstituted vial to the supplier QC records. AminoCore Research recommends retaining unused kit packaging for the duration of the study to facilitate audit reconstruction.
Discrepancy handling: If a discrepancy is identified between calculated and observed dose effects, the documentation trail allows investigators to isolate whether the variable originated in the peptide stock, the diluent, the syringe (volumetric accuracy), or operator technique. This level of traceability is the practical foundation of reproducible peptide research and is enabled by the standardized, single-source nature of the Research Kit 30 Pack inventory.
Pre-Use Inspection Protocol for Kit Components
A standardized pre-use inspection protocol is the first line of defense against compromised consumables entering a peptide reconstitution workflow. Each component of the Research Kit 30 Pack should be visually and tactilely evaluated before deployment in an experimental procedure.
Bacteriostatic Water Vial Inspection:
- Examine the seal: The aluminum crimp seal and flip-off plastic cap should be intact, with no evidence of prior removal or tampering. The flip-top should snap cleanly when removed.
- Inspect the septum: The rubber stopper should be flat, intact, and free of cuts, depressions, or surface contamination. Any prior penetration marks (other than the expected manufacturer fill puncture, if visible) indicate prior use and warrant disposal.
- Hold against a dark background: Examine the solution for particulates, turbidity, or color. The solution should be water-clear and free of visible particles. Faint amber discoloration may indicate light exposure degradation of benzyl alcohol — discard if observed.
- Check the lot number and expiration date: Record both in the experimental notebook. Expired bacteriostatic water has reduced preservative potency.
Syringe Inspection:
- Verify the sterile blister pack is intact with no punctures or peeled seals.
- After opening, confirm the needle bevel is symmetric and undamaged under a 10x loupe if precision is critical.
- Test the plunger glide by drawing back and depressing once before use — it should move smoothly without sticking. Sticky plungers compromise volumetric accuracy.
- Confirm the graduation markings are legible and undamaged.
Alcohol Prep Pad Inspection:
- Sealed sachet should be intact and feel saturated (not dried out from a compromised foil seal).
- Upon opening, the pad should be visibly wet and emit the characteristic isopropanol odor. Dry pads have lost preservative concentration and antiseptic efficacy.
Constitution Syringe (Mixing Syringe) Inspection:
- Verify Luer lock or Luer slip fitting is intact and the syringe barrel is free of cracks.
- Plunger should move freely throughout the full barrel length.
Documentation: Record the lot numbers of bacteriostatic water and syringes used for each reconstitution event in the experimental notebook. This supports root-cause analysis if a downstream contamination or potency anomaly is detected.
Personal Protective Equipment and Laboratory Safety When Using Kit Components
While the Research Kit 30 Pack components are designed for routine laboratory peptide reconstitution, researchers should follow institutional biosafety and chemical hygiene standards appropriate to their work. This section outlines baseline personal protective equipment (PPE) and procedural safety considerations when handling kit components, lyophilised peptide powders, and reconstituted solutions.
Recommended baseline PPE:
- Nitrile gloves (powder-free, 4-mil minimum): Latex alternatives preferred to avoid sensitisation; powder-free formats prevent particulate contamination of work surfaces and reconstituted solutions. Change gloves between vials when working with different compounds to prevent cross-contamination.
- Laboratory coat or disposable gown: Long-sleeved barrier to prevent skin contact with potentially active research compounds, particularly lyophilised powders that may aerosolise during vial opening.
- Safety eyewear: Side-shielded safety glasses or goggles. Recommended during vial septum penetration (rare droplet ejection) and reconstitution mixing steps.
- Surgical or N95 respiratory protection: Recommended when opening lyophilised peptide vials or weighing solid compounds in non-ventilated areas. A certified biosafety cabinet or fume hood is preferred for compounds with unknown inhalation toxicity profiles.
Procedural safety practices:
- Work in a designated zone: Establish a clean reconstitution area separate from chemical storage, food, and high-traffic lab benches. Cover the surface with absorbent bench paper.
- Open vials carefully: Lyophilised peptide vials are typically sealed under partial vacuum; flip-off caps should be removed with steady downward pressure to prevent powder dispersion. Allow vials to equilibrate to room temperature before opening to minimise condensation.
- Manage sharps continuously: Never recap used needles. Activate the integrated needle shield (if equipped) immediately after withdrawal and transfer directly to an approved sharps container within arm's reach.
- Spill response: For bacteriostatic water spills, blot with absorbent material and disinfect with 70% isopropyl alcohol. For peptide solution spills, follow your institution's chemical spill protocol — most research peptides require nitrile glove, absorbent containment, and hazardous waste disposal of contaminated materials.
- Hand hygiene: Wash hands with soap and water immediately after glove removal, even if no visible contamination occurred. Alcohol-based hand sanitiser is not a substitute for handwashing after chemical handling.
Allergen and sensitivity considerations: The Research Kit 30 Pack components are latex-free, but researchers with known sensitivities to benzyl alcohol (present in bacteriostatic water at 0.9%) or isopropyl alcohol (in prep pads) should review safety data sheets before use. Adequate ventilation minimises exposure to volatile preservatives during reconstitution.
Pregnancy and reproductive safety: Researchers who are pregnant or planning pregnancy should consult their occupational health office before handling any pharmacologically active research compound, regardless of intended use scope. Many peptides have undefined developmental toxicity profiles and warrant precautionary handling beyond standard PPE.
Reconstitution Troubleshooting and Common Workflow Errors
Reproducibility in peptide research depends as much on avoiding common reconstitution errors as on following the correct protocol. The Research Kit 30 Pack provides the physical components for sterile reconstitution, but several recurring procedural errors can compromise peptide integrity or dosing accuracy even when correct supplies are used. The following troubleshooting matrix addresses the most frequent failure modes observed in laboratory peptide workflows.
| Observed Issue | Likely Cause | Corrective Action |
|---|---|---|
| Cloudy or turbid solution after reconstitution | Peptide aggregation from vigorous shaking, incompatible pH, or excessive concentration | Discard vial; reconstitute fresh aliquot using gentle swirling and lower concentration (1–2 mg/mL) |
| Visible undissolved powder after 10 minutes | Hydrophobic peptide requiring acidified diluent or co-solvent | Consult peptide-specific solubility data; consider acetic acid (0.1%) or DMSO pre-dissolution |
| Dose drift across replicate experiments | Volumetric error from parallax reading or inconsistent needle dead-space technique | Calibrate syringe reading at eye level; use consistent plunger-pull technique; verify by gravimetric checks |
| Microbial contamination of multi-dose vial | Inadequate septum disinfection or repeated entry without fresh prep pad | Discard contaminated vial; swab septum with fresh alcohol prep pad for full 30-second contact time before each entry |
| Loss of peptide activity over storage | Light exposure, temperature excursion, or oxidative degradation (Met/Cys residues) | Store reconstituted vial at 2–8°C protected from light; aliquot for –20°C if >14 days needed |
| Bubbles in syringe affecting dose accuracy | Rapid aspiration drawing air through septum or down-stroke air entrainment | Aspirate slowly with vial inverted; tap syringe to dislodge bubbles; expel air before dosing |
Quality-control verification steps recommended after each reconstitution event using the Research Kit 30 Pack:
- Visual inspection: Solution should be clear, colourless, and free of particulates against a contrasting background under good lighting.
- Volume verification: Confirm reconstitution volume against the calculated target (e.g., 5 mg + 1 mL BWFI → 5 mg/mL) by checking residual diluent volume in the constitution syringe.
- Label integrity: Reconstitution date, concentration, peptide identifier, and operator initials should be recorded on the vial within 60 seconds of reconstitution.
- Documentation: Record lot numbers for the kit BWFI, peptide vial, and reconstitution timestamp in the laboratory notebook or electronic record system.
Establishing a standardised reconstitution standard operating procedure (SOP) using the kit components — with embedded troubleshooting decision trees — significantly improves inter-operator reproducibility in multi-investigator research environments.
Workspace Preparation and Environmental Controls for Kit-Based Reconstitution
Environmental conditions at the point of reconstitution significantly influence the microbiological quality, particulate burden, and chemical stability of prepared peptide solutions. While the Research Kit 30 Pack provides sterile single-use components that establish a baseline of contamination control, investigators are responsible for preparing an appropriate workspace that complements the kit's engineered controls.
Recommended workspace setup:
- Surface selection: Use a non-porous, easily disinfectable work surface such as stainless steel, sealed laminate, or polished epoxy. Avoid wood, fabric-covered, or scratched surfaces that harbour microbial biofilms.
- Pre-use disinfection: Wipe the work area with 70% isopropyl alcohol or a sporicidal disinfectant (e.g., 0.5% sodium hypochlorite for biosafety cabinets), allowing a minimum 30-second wet contact time before commencing reconstitution.
- Airflow considerations: Perform reconstitution in a Class II biosafety cabinet or laminar flow hood where available. If working on the open bench, minimise air currents by closing windows, turning off oscillating fans, and avoiding high-traffic corridors during the procedure.
- Lighting: Ensure adequate task lighting (≥500 lux at the work surface) to facilitate visual inspection of vials, syringes, and solutions for particulates, cloudiness, or colour changes.
- Temperature and humidity: Maintain ambient temperature between 18-25°C and relative humidity between 30-60%. Elevated humidity accelerates hygroscopic absorption by lyophilised cake; low humidity increases electrostatic adherence of fibres and dust to surfaces.
Material staging sequence: Before opening any sterile packaging, arrange materials in the order of use: alcohol prep pads, bacteriostatic water vial, peptide vial, constitution syringe, and final-dose insulin syringes. This linear workflow reduces hand movements over open sterile fields and minimises the duration during which exposed septa and needle tips remain vulnerable to airborne contamination.
Personnel preparation: Don clean nitrile or latex gloves immediately before commencing work. Tie back long hair, remove jewellery from hands and wrists, and avoid wearing loose-fitting sleeves that may drag across the work surface. For extended reconstitution sessions involving multiple vials, change gloves at least every 30 minutes or whenever gross contamination is suspected.
Single-Use Discipline and Sterile Workflow for the 30-Pack Syringe Set
Each syringe in this 30-pack is individually packaged in a sealed blister to preserve sterility until point of use. Maintaining single-use discipline across all 30 units is the single most important practice for ensuring reproducible, contamination-free peptide reconstitution and transfer in a research laboratory setting.
Pre-Use Inspection Protocol:
- Verify the individual blister pack is intact, dry, and shows no signs of crushing, puncture, or moisture ingress before opening.
- Check the visible portion of the syringe barrel for clarity — any cloudiness, internal moisture, or visible particulate disqualifies the unit.
- Confirm the protective needle cap is firmly seated and undisturbed; a loose cap indicates possible compromise of needle sterility.
- Open the blister at the marked peel-tab, avoiding contact between gloved fingers and the needle hub or plunger shaft.
Aseptic Transfer Workflow:
- Wipe the vial septum with a fresh 70% isopropyl alcohol prep pad and allow 30 seconds of dwell time for evaporation before puncture.
- Remove the needle cap immediately before puncture, holding the syringe by the barrel — never the needle shaft.
- Insert at a 45-90° angle to the septum centre, advancing in a single controlled motion to minimise coring.
- After withdrawal, immediately recap using a one-handed scoop technique against a stable surface — never two-handed recapping, which is a documented sharps injury risk.
- Dispose of the used syringe into a rigid, puncture-resistant sharps container compliant with local biohazard regulations.
Critical Reuse Prohibition: Insulin syringes in this 30-pack are not designed for reuse, even on the same vial. Reuse introduces three documented risks: (1) needle dulling that increases coring and particulate generation on subsequent septum entries, (2) microbial contamination of the needle lumen and barrel interior despite recapping, and (3) silicone oil depletion that alters plunger glide characteristics and compromises volumetric accuracy. For multi-vial workflows, allocate one syringe per vial penetration event and document accordingly.
Optimising the 30-Pack for a Typical 4-Week Peptide Research Campaign
The 30-unit count of this syringe set is designed to support a standard multi-week peptide research workflow without requiring mid-campaign reordering. Planning syringe allocation against the experimental design protects sterility, minimises waste, and ensures volumetric accuracy throughout the study.
Step-by-step campaign planning:
- Define the dosing schedule. For a 28-day protocol with daily single-draw dosing from a single reconstituted vial, allocate 28 syringes for daily draws plus 1-2 syringes per vial for the initial reconstitution diluent transfer (if a separate reconstitution syringe is not provided).
- Map vial-to-syringe ratios. A 10 mg peptide vial reconstituted in 2 mL bacteriostatic water yields 5 mg/mL stock. At a 250 µg research dose, the vial supports 40 draws — exceeding the 28-day single-vial campaign. For multi-vial campaigns, plan one fresh syringe per vial reconstitution event.
- Reserve syringes for quality checks. Allocate 2-3 syringes for volumetric calibration verification (gravimetric weighing of 0.1 mL water draws) at the start, midpoint, and end of the campaign to confirm dosing consistency.
- Inspect packaging at receipt. Verify each of the 30 individually wrapped pouches is intact, with no visible punctures, moisture, or compromised seals. Reject any unit showing packaging damage.
- Label storage with use-by dates. Although the syringes themselves are stable at room temperature for years (typical manufacturer expiry 3-5 years), label the outer carton with the campaign start date for traceability.
- Discard appropriately. After each draw, recap (if practical) and dispose of the used syringe in a rigid puncture-resistant sharps container — never the general lab waste stream.
Workflow note: The 1/4-inch (6 mm) needle length is optimised for bench-top access to standard 20 mm crimped peptide vial septa held upright on a flat surface. For taller vials or inverted withdrawal technique, the short needle still reaches the headspace and liquid layer adequately when the vial is tilted or the needle is positioned near the rubber stopper edge. Always disinfect the septum with an alcohol prep pad and allow it to air-dry (10-15 seconds) before each penetration to prevent alcohol carry-over into the peptide solution.
Air Bubble Removal and Priming Technique for 0.5 mL 31G Insulin Syringes
Air bubble entrainment is one of the most common sources of dosing error in insulin-style syringes used for peptide research, particularly at the low draw volumes (10-50 µL) typical of potent reconstituted peptides. A single 5 µL air bubble in a 50 µL draw represents a 10% volumetric error — well outside the ±5% tolerance specified in ISO 8537 for insulin syringe graduation accuracy. The narrow internal diameter of 0.5 mL barrels and the high surface tension at the 31G needle bore amplify bubble retention compared with larger-bore syringes.
Recommended priming and bubble-removal protocol for the 30-pack:
- Pre-equilibrate the vial. Allow the reconstituted peptide vial to reach room temperature (≈15 minutes from refrigerator) to reduce dissolved-gas nucleation when warmed solution contacts the cooler syringe barrel.
- Inject air equivalent. Before drawing peptide solution, draw an air volume equal to the intended dose into the syringe and inject it into the vial headspace. This equalises pressure and prevents vacuum-driven bubble formation during withdrawal.
- Invert vial, draw slowly. With the vial inverted and the needle tip below the meniscus, withdraw plunger slowly (≈2-3 seconds per 50 µL) to minimise turbulent flow and Venturi-effect bubble nucleation.
- Over-draw and expel. Draw 5-10 µL beyond the target volume to capture any bubble in the over-draw region.
- Tap and consolidate. With needle pointing up and syringe vertical, tap the barrel gently with a finger to coalesce small bubbles into the headspace at the plunger end.
- Expel headspace. Slowly depress plunger to expel air and excess solution back into the vial until the meniscus aligns with the target graduation.
- Verify volume visually. Read the graduation at eye level with the meniscus base aligned with the line — parallax error at the 31G barrel diameter can introduce ±1-2 µL error if read from above or below.
Specific to 31G 1/4-inch needles: The short 6 mm cannula has a small internal volume (≈0.5 µL) but high resistance to flow due to the 0.26 mm internal diameter. Rapid plunger withdrawal can generate cavitation bubbles at the needle hub that are difficult to dislodge once formed. Slow, steady technique is more important than speed, especially for viscous peptides such as concentrated semaglutide or tirzepatide solutions where bubble persistence is prolonged.
Documentation: Investigators conducting GLP-aligned reconstitution should record the post-bubble-removal volume on the vial label and reconstitution worksheet, and note any deviation from target dose >5% as a protocol variance requiring repeat draw.
Inventory Planning and Single-Use Allocation for a 30-Syringe Campaign
Effective use of the 30-syringe pack requires advance planning of syringe allocation across the research campaign to maintain single-use discipline without running short of sterile units mid-experiment. The following framework supports common laboratory peptide workflows where multiple vials are reconstituted, sampled, and re-accessed across a multi-week schedule.
- Map total draw events. List every planned vial access, including initial reconstitution, working aliquot transfers, dilution prep, and dosing draws. Each event consumes one syringe under strict single-use protocol.
- Reserve a contingency margin. Allocate 10–15% of the pack (3–5 syringes) for accidents — bent needles, dropped units, failed draws, or quality-control re-checks.
- Separate reconstitution and draw syringes. If using a larger reconstitution syringe for initial diluent transfer, the 31G insulin syringes in this pack should be reserved for accurate working-volume measurement rather than bulk diluent handling.
- Stage by week, not by day. Pre-stage a labelled tray containing the syringes needed for each experimental week, with date and intended use noted. This prevents inadvertent reuse and supports chain-of-custody documentation.
- Track usage on a worksheet. Log each syringe consumption against vial ID, draw volume, and timestamp. This is essential for GLP-aligned documentation and for identifying inventory gaps before they affect experiments.
- Quarantine compromised units. If a syringe blister appears damaged or the tip cap is loose on inspection, set it aside as non-sterile and exclude it from sterile workflow.
For a typical 4-week peptide study involving 2–3 vials with 6–8 draws per vial, the 30-pack provides sufficient inventory with adequate contingency margin. Larger campaigns or multi-peptide studies may require supplementary packs, ideally ordered before experimental start to avoid lot-to-lot variability in syringe specifications mid-campaign.
Operator Ergonomics and Thumb-Plunger Technique for 0.5 mL 31G Syringes
Reproducible volumetric delivery from a 0.5 mL insulin-style syringe depends not only on the syringe itself but also on operator technique. The thin-wall 31G needle and small barrel diameter of the syringes in this 30-pack require a controlled, low-force approach to plunger actuation. Excessive thumb pressure produces uncontrolled bolus delivery and over-shoots the graduation mark; insufficient pressure produces stalling and air ingress at the needle hub.
Recommended technique for laboratory dispensing:
- Grip: hold the syringe barrel between the index and middle fingers at the flange, with the thumb resting (not pressing) on the plunger thumb-pad. This is the standard "insulin grip" used in clinical training.
- Priming: after drawing slightly more than the target volume, hold the syringe vertically with the needle pointing up, tap the barrel to coalesce air bubbles at the needle hub, then expel air and excess volume back into the source vial until the meniscus aligns with the target graduation.
- Meniscus reading: read the volume at eye level with the bottom of the meniscus aligned with the printed graduation line. The U-100 scale is calibrated such that 50 units = 0.5 mL, 10 units = 0.1 mL, and 1 unit = 0.01 mL (10 µL).
- Delivery: apply slow, continuous thumb pressure over 2-4 seconds for the full barrel volume. Rapid plunger depression in thin-wall 31G syringes generates back-pressure that can transiently deform the elastomeric stopper and produce volume error.
- Residual check: after delivery, briefly hold pressure on the plunger for 2 seconds before withdrawal to allow the dead-space volume to clear the needle lumen.
Operators new to 31G insulin-style syringes should practice the above sequence with bacteriostatic water and an empty waste vial before working with valuable peptide stocks. A common training endpoint is the ability to repeatedly dispense 0.10 mL ± 0.005 mL into a tared analytical balance across five consecutive aspirations.
For long research campaigns, rotating the syringe-holding hand between sessions reduces repetitive strain on the thumb's flexor pollicis longus tendon, which is the most frequent ergonomic complaint reported by laboratory staff performing high-volume insulin-syringe workflows.
Step-by-Step Use Protocol for the 0.5 mL 31G 1/4-inch Syringe Pack
The following protocol is intended as a general laboratory reference for in vitro research applications using the syringes supplied in this 30-pack. All work should be performed in a clean, designated reconstitution area following institutional biosafety and sharps-handling policies.
- Pre-use inspection. Visually inspect the outer blister pouch for breaches, moisture ingress, or seam failure. Confirm the lot number and printed expiry date are legible. Discard any unit with compromised packaging.
- Hand hygiene and PPE. Wash hands with antimicrobial soap or use 70% isopropyl alcohol hand rub. Don nitrile gloves, safety eyewear, and a laboratory coat appropriate for the compound class being handled.
- Work surface preparation. Wipe the work surface with a 70% isopropyl alcohol prep pad and allow to air-dry (minimum 30 seconds for full antimicrobial action).
- Aseptic opening. Peel the Tyvek lid back from the corner indicated by the manufacturer, taking care not to touch the inner pouch surface or the syringe barrel below the plunger flange.
- Tip cap removal. Hold the syringe by the barrel and remove the orange or clear protective tip cap with a straight pull. Do not twist, as this can dislodge the needle hub bond. Discard the cap into a sharps-safe receptacle.
- Vial septum disinfection. Wipe the rubber septum of the peptide vial and the diluent vial with a fresh 70% isopropyl alcohol prep pad. Allow 30 seconds for solvent evaporation before puncturing.
- Drawing diluent. Pull the plunger to the desired volume mark (each minor graduation on the U-100 scale = 0.01 mL = 1 unit). Insert the needle at a 45-90° angle through the septum and slowly invert the vial. Withdraw the calibrated volume of bacteriostatic water.
- Reconstitution transfer. Insert the needle through the lyophilised peptide vial septum at a 45° angle and slowly dispense the diluent down the inner wall of the vial. Avoid jet-spraying directly onto the peptide cake to minimise mechanical shear.
- Gentle dissolution. Withdraw the syringe, recap the vial (if reusable), and gently swirl until the peptide is fully dissolved. Do not vortex or shake aggressively.
- Single-use disposal. Place the used syringe with attached needle directly into a puncture-resistant sharps container. Do not recap, bend, or detach the needle.
Critical reminders: Each syringe is intended for single-use only. Reuse compromises sterility, dulls the needle bevel (increasing coring risk on subsequent draws), and introduces cross-contamination risk between vials. With 30 individually pouched units in this kit, a typical 4-week research campaign covering 6-10 peptide vials with periodic re-dosing draws is well-supported.
Optimising Syringe Selection Across a Multi-Peptide Research Workflow
The 30-pack of 0.5 mL 31G 1/4-inch syringes is sized to support a structured, single-use workflow across multiple peptide compounds. The following framework helps allocate syringes efficiently while maintaining aseptic discipline and dosing reproducibility.
- Map the campaign: List each peptide compound, planned reconstitution events, and the number of individual draws required. A typical 4-week single-compound campaign uses 1 syringe for reconstitution (drawing bacteriostatic water into the lyophilised vial) plus 1 syringe per dosing event.
- Allocate by compound, not by day: Group syringes by compound to avoid accidental cross-vial use. Pre-label storage containers (compound name, lot, reconstitution date) and assign a syringe count to each.
- Reserve a buffer: Set aside 10-15% of syringes (3-5 per 30-pack) for redraws, calibration checks, or accidental damage to packaging. This prevents workflow interruption mid-campaign.
- Confirm volume match: The 0.5 mL barrel supports draw volumes up to 50 IU (U-100 scale) or 0.5 mL. For larger reconstitution volumes (e.g., 1 mL of bac-water added to a vial), perform the addition in two sequential 0.5 mL draws or use a higher-capacity reconstitution syringe.
- Inspect each blister: Before use, verify the individual blister is intact, the tip cap is seated, and the plunger has not been depressed during transit. Discard any unit with compromised packaging.
- Single-use discipline: Each syringe is intended for one draw event from one vial. Never reuse a syringe across vials — silicone oil migration, residual peptide, and needle dulling all compromise downstream draws.
- Disposal: Deposit used syringes directly into an FDA-cleared sharps container at the point of use; never recap.
Worked example: A researcher planning a 28-day pharmacology study with one peptide compound and daily dosing would allocate 1 reconstitution syringe + 28 dosing syringes = 29 syringes, leaving 1 buffer unit from a 30-pack. For multi-compound studies, scale syringe inventory accordingly and consider ordering multiple 30-packs to maintain single-use discipline across compounds.
Cold-Solution Drawing Technique for Refrigerated Peptide Vials Using 31G 1/4-inch Syringes
Reconstituted peptide vials are routinely stored at 2-8°C to slow hydrolytic and oxidative degradation. Drawing cold solution into a small-bore 31G 1/4-inch syringe presents reproducibility challenges that are not encountered with larger-gauge needles or warmer solutions. The following workflow has been optimised for the 0.5 mL syringes in this 30-pack.
Recommended cold-solution drawing protocol:
- Remove the vial from 2-8°C storage and allow it to equilibrate on a clean bench at controlled room temperature (18-22°C) for 5-10 minutes. Do not warm above 25°C and never use heat sources.
- Inspect the vial for cloudiness, precipitate, or visible particulates. Cold solutions occasionally show transient haze that resolves on equilibration; persistent cloudiness warrants exclusion.
- Wipe the septum with a fresh 70% isopropyl alcohol prep pad and allow to air-dry (≥30 seconds).
- Inject equivalent air volume into the vial headspace before drawing to equalise pressure — cold vials develop slight negative pressure that resists smooth aspiration with 31G needles.
- Insert the 31G needle at a consistent location on the septum (rotate insertion sites across the vial septum to minimise localised coring across the campaign).
- Invert the vial and draw slowly (1-2 seconds for 0.1-0.2 mL) — rapid aspiration through a 31G lumen induces cavitation bubbles that compromise volumetric accuracy.
- Tap the barrel to coalesce air bubbles, then expel back into the vial headspace and redraw to the target graduation.
- Withdraw the needle at the same angle of insertion to minimise septum tearing.
Important notes: Cold solutions exhibit higher viscosity, which increases plunger glide force and prolongs draw time. Operators new to 31G syringes often under-draw cold solutions because they release plunger tension before the final volume is achieved. Verify the meniscus reaches the intended graduation line at eye level before withdrawal. Never warm vials above ambient room temperature to ease drawing, as elevated temperature accelerates peptide degradation kinetics.
Batch Reconstitution Planning for the 30-Syringe Pack Across Multi-Peptide Campaigns
The 30-pack format is designed to support a structured research campaign in which multiple peptide compounds are reconstituted, aliquoted, and dosed over a defined experimental window. Effective use of the pack begins with a written allocation plan that maps each syringe to a specific operation: vial reconstitution, aliquot transfer, or dosing event. This section outlines a recommended planning framework for typical 4- to 6-week research workflows.
Step 1: Compound inventory and syringe budgeting. Begin by listing every peptide compound that will be handled during the campaign. For each compound, estimate (a) the number of vials requiring reconstitution, (b) the number of aliquot transfers planned, and (c) the number of dosing events. As a general rule, allocate one syringe per discrete sterile operation — never reuse a syringe across vials or operations, regardless of the time elapsed.
Step 2: Reserve syringes for contingency. A well-designed campaign reserves approximately 15-20% of the pack (4-6 syringes from a 30-pack) for unplanned operations: re-reconstitution after suspected contamination, replacement of damaged units, or additional time-point sampling. Without a contingency reserve, mid-campaign supply shortages can force operators to choose between aseptic compromise and experimental delay.
Step 3: Pre-label allocation worksheet. Create a worksheet listing each of the 30 syringes by sequential number, with columns for intended use, peptide compound, date of use, operator initials, and lot number from the blister. This worksheet supports both forward planning and retrospective audit, and aligns with GLP-style documentation expectations.
Step 4: Storage organisation. Store the unopened 30-pack at controlled room temperature (15-25°C) in its original outer carton, protected from direct light and excessive humidity. Do not refrigerate or freeze the syringes — silicone lubricant performance and elastomer flexibility are optimised for room-temperature storage and use.
Step 5: Inspection cadence. Inspect the outer carton weekly during the campaign for integrity, and inspect each individual blister immediately before opening. Any unit with compromised packaging, visible particulate, or expired lot dating must be discarded into a sharps container without use.
For a typical campaign involving 3-5 peptide compounds with weekly aliquot preparation and 2-3 dosing events per week, a single 30-pack provides sufficient single-use capacity for 4-6 weeks of work while preserving contingency margin. Operators handling higher-throughput workflows or larger animal cohorts should plan for two or more 30-packs per campaign.
Optimal Vial Septum Penetration Angle and Technique for 31G 1/4-inch Needles
The short 1/4-inch (6 mm) length and fine 31G gauge of the needles in this 30-pack require a specific septum penetration technique to maximise draw-up efficiency, minimise coring, and avoid mechanical bevel damage during reconstitution and aspiration from peptide vials.
Recommended technique — angled bevel-up entry:
- Position the vial upright on a clean, flat work surface following alcohol prep pad disinfection of the rubber septum. Allow alcohol to air-dry fully (approximately 30 seconds) to avoid alcohol carryover into the peptide solution.
- Orient the syringe bevel facing upward (bevel notch visible at the top of the needle tip) and approach the septum at a 45-60° angle relative to the vial surface.
- Apply gentle, steady downward pressure while simultaneously bringing the syringe to vertical (90°) as the bevel tip pierces the septum. This rolling entry minimises the shear force on the rubber and reduces the probability of dislodging a rubber core into the solution.
- Avoid lateral bevel rocking after septum entry, as this can enlarge the puncture channel and compromise septum reseal integrity for subsequent draws.
Inversion and aspiration: Once the needle is fully seated through the septum, invert the vial so that the needle tip remains submerged below the meniscus of the bacteriostatic water or reconstituted peptide solution. The short 1/4-inch needle length is generally adequate for standard 2 mL and 5 mL peptide vials when fully inserted; for taller vials, slight repositioning may be required to ensure the bevel remains below the liquid surface during draw-up.
Pre-pressurisation technique: For volumes exceeding 0.2 mL, inject an equivalent volume of air into the vial headspace before aspiration to maintain neutral pressure equilibrium. This prevents vacuum formation that would otherwise resist plunger withdrawal and introduce air bubbles into the syringe barrel.
Withdrawal: After drawing the desired volume, withdraw the needle vertically through the septum without rotation. Recap the needle using a single-handed scoop technique against a rigid surface (never with the opposing hand) to comply with sharps safety guidance prior to disposal in an approved sharps container.
Coring minimisation: Studies of insulin syringe needle coring frequency document coring rates below 1% per septum penetration for 31G needles when angled bevel-up entry is employed, compared to coring rates exceeding 5% with bevel-down or perpendicular blunt-force entry (Asakura et al., 2001).
Recommended Single-Vial Reconstitution Protocol Using a 0.5 mL 31G 1/4-inch Insulin Syringe
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are sized and graduated specifically for low-volume aqueous dispensing during lyophilized peptide reconstitution and subsequent aliquot withdrawal. The following protocol consolidates aseptic best practice into a reproducible 10-step workflow suitable for a single peptide vial.
- Workspace preparation: clean a flat, non-porous bench surface with a fresh 70% IPA prep pad. Allow 30 seconds for the alcohol to evaporate fully.
- Component layout: place the sealed peptide vial, bacteriostatic water (BW) vial, one individually blistered 0.5 mL 31G insulin syringe, and 2 alcohol prep pads on the cleaned surface.
- Septum disinfection: wipe the rubber septum of both the BW vial and the peptide vial with separate alcohol prep pads. Allow 30 seconds of contact time before puncture.
- Blister inspection: visually inspect the syringe blister for intact seals, no visible moisture, no cracks, and intact tip cap. If the blister is compromised, discard the unit.
- Aseptic peel: peel the blister from the plunger end to expose the syringe. Avoid touching the needle shaft or tip cap.
- BW aspiration: remove the tip cap (retain on a clean surface for sharps disposal). Invert the BW vial, insert the 31G needle at a 45-60° angle to minimise coring, and slowly aspirate the calculated reconstitution volume (typically 1-2 mL across multiple draws for a 10 mg vial — see step 7).
- Volume planning: the 0.5 mL syringe holds a maximum of 50 units (0.5 mL). For larger reconstitution volumes, use the separately supplied constitution syringe; the 0.5 mL units are optimised for the subsequent withdrawal of single research aliquots.
- Slow side-wall delivery: insert the 31G needle into the peptide vial at a 45° angle and slowly express the BW down the inner side wall of the vial. Do not direct the stream onto the lyophilized cake.
- Gentle dissolution: swirl the vial gently (do not shake or vortex) until the cake fully dissolves. Inspect for clarity and absence of particulates.
- Sharps disposal and labelling: immediately discard the used syringe into an approved sharps container. Label the reconstituted vial with peptide name, concentration (mg/mL), reconstitution date, and operator initials.
Subsequent withdrawals for individual research aliquots are then performed with a fresh 0.5 mL 31G syringe from the 30-pack, applying the single-use discipline that underpins the dosing-accuracy and contamination-control rationale of individually blistered units.
Verifying Plunger Function and Detecting Defects Before Use of 0.5 mL 31G Syringes
Although the 0.5 mL 31G 1/4-inch syringes in this 30-pack are manufactured to ISO 8537 standards and supplied in individual sterile blister packaging, pre-use functional verification remains a best-practice safeguard against rare manufacturing defects, transit damage, and packaging compromise. A structured pre-use inspection adds less than 15 seconds per syringe and dramatically reduces the likelihood of mid-procedure failure during peptide reconstitution.
Step-by-step pre-use verification protocol:
- Inspect outer blister. Confirm the peel-back seal is intact, the blister is not crushed or punctured, and any printed lot/expiry information is legible. Discard any blister showing fluid intrusion, discolouration, or seal failure.
- Peel back the blister in a controlled direction. Open from the plunger end (not the needle end) to avoid accidental tip-cap displacement. The syringe should slide free without resistance.
- Visual inspection of the barrel. Hold the syringe up to a light source and confirm: (a) no cracks or stress whitening in the polypropylene barrel, (b) graduation markings are clear and complete, (c) no foreign particulate is visible inside the barrel.
- Tip cap inspection. The protective tip cap should be firmly seated on the needle hub. A loose, missing, or partially displaced cap indicates a sterility breach—discard the syringe.
- Plunger function test. Without removing the tip cap, slowly draw the plunger back to the 0.5 mL mark and return it to zero. Movement should be smooth without sticking, juddering, or excessive force. Audible "squeaking" or stick-slip motion indicates dried siliconisation and predicts inaccurate dosing.
- Remove the tip cap. Pull straight off without twisting. Inspect the needle bevel under magnification if available—any visible burr, hook, or discolouration warrants discarding the unit.
- Proceed with reconstitution. Begin the aseptic workflow within 60 seconds of cap removal to minimize airborne contamination of the exposed needle.
Common defects and disposition:
- Plunger sticking: Discard — predicts dose-volume error.
- Air bubble between plunger stopper and graduation line: Acceptable if removable by tap-and-expel technique.
- Bent needle: Discard — coring risk increases sharply.
- Damaged blister with intact tip cap: Sterility cannot be assured; discard.
- Crystallised material on plunger rod: Likely silicone migration; discard to avoid contamination of the reconstituted solution.
Document defective units against lot number and report clusters of failures (≥2 per pack) for supplier quality review.
Daily Workflow Integration of the 30-Pack Across a Multi-Week Peptide Reconstitution Campaign
The 30-pack format is sized to support a typical 4-week single-investigator peptide research campaign, with approximately one single-use syringe allocated per dosing or aliquoting event. Structured allocation across the campaign improves traceability, reduces in-process waste, and aligns with single-use sterile discipline expected in laboratory peptide research.
Suggested daily workflow integration:
- Pre-session inspection: Select one individually blistered syringe from the 30-pack. Inspect the blister seal for integrity — reject any unit with compromised packaging, visible particulates inside the barrel, or a displaced plunger stopper.
- Aseptic field preparation: Wipe the work surface with 70% isopropyl alcohol, allow to air-dry, and arrange the unopened syringe, target peptide vial, and bacteriostatic water vial on the prepared field.
- Septum disinfection: Swab the rubber septum of both vials with a fresh alcohol prep pad and allow 30 seconds of contact time before penetration.
- Bevel-up insertion: Peel the blister from the syringe hub end, remove the tip cap, and insert the 31G 1/4-inch needle through the vial septum bevel-up at approximately 45-60°, rotating to vertical once the bevel has cleared the septum. This minimises coring risk.
- Volume draw and verification: Aspirate the planned reconstitution or aliquot volume, holding the syringe vertically at eye level to confirm the meniscus aligns with the target graduation mark. Tap the barrel to dislodge air bubbles and expel any headspace.
- Single-use commitment: Use the syringe for one event only — one reconstitution, or one aliquot transfer. Do not re-cap or re-use the needle on a second vial; this introduces cross-contamination and coring risk that compounds across the campaign.
- Sharps disposal: Discard the entire syringe-needle assembly into an OSHA-compliant rigid sharps container immediately after use. Do not bend, recap, or detach the needle.
- Documentation: Log the date, syringe lot number (from blister), vial accessed, volume drawn, and operator initials in the reconstitution worksheet for chain-of-custody traceability.
This per-event allocation supports approximately 30 documented events across a 4-week campaign — sufficient for two SC dosing events per week across a 14-day chronic study, or for reconstituting and aliquoting multiple peptide stock vials across a small comparative pharmacology project.
Quick-Reference Handling Summary for the 0.5 mL 31G 1/4-inch 30-Pack
This concise reference distils the critical handling principles for the individually packaged 0.5 mL 31G 1/4-inch syringes supplied in this 30-pack. It is intended as a bench-side quick guide; detailed protocols are provided in the dedicated handling sections elsewhere on this page.
Pre-use inspection (every syringe, every time):
- Confirm the individual blister is intact, sealed, and free of moisture, discolouration, or visible damage.
- Verify the lot number on the carton matches the documented inventory record.
- Peel back the blister from the labelled corner — do not tear through the sterile barrier.
- Inspect the syringe barrel for cracks, the plunger for displacement, and the needle tip cap for secure seating.
- Do not use any syringe whose tip cap is loose, displaced, or missing.
Aseptic draw technique:
- Wipe the peptide vial septum with a 70% isopropyl alcohol prep pad and allow to air-dry (≥30 seconds).
- Remove the needle tip cap by pulling straight off — do not twist.
- For lyophilised peptide reconstitution: draw the calculated volume of bacteriostatic water into the syringe, insert the needle into the vial septum at a 45-degree bevel-up angle, then advance to vertical before slowly injecting the diluent down the vial wall (not directly onto the peptide cake).
- For aliquoting reconstituted solution: invert the vial, ensure the needle tip is below the meniscus, and draw slowly to minimise air entrainment.
- Tap the barrel gently to consolidate air bubbles at the hub, then express the air back into the vial before withdrawing.
Single-use discipline:
- Each syringe is intended for one peptide vial, one draw event. Do not re-cap and re-use.
- Re-capping with the original tip cap is discouraged due to needlestick risk; if necessary, use a single-handed scoop technique.
- Dispose of the used syringe immediately into a puncture-resistant sharps container compliant with local regulations.
Inventory allocation: For a standard 4-week research campaign with reconstitution every 7 days and 5-7 aliquot events per cycle, allocate approximately 6-8 syringes per week. The 30-pack provides headroom for inspection rejections, repeat draws, and contingency aliquoting without compromising single-use discipline.
Recommended Disposal and Sharps Containment Workflow for the 30-Pack
Proper disposal of used syringes from this 30-pack is a regulatory and biosafety requirement in all laboratory settings. The 31G 1/4-inch fine-gauge needle is permanently bonded to the syringe barrel, meaning the entire unit must be discarded as a sharp — partial disassembly is not appropriate and increases needlestick injury risk.
Recommended disposal workflow:
- Do not recap. Recapping a used needle is the leading cause of needlestick injuries in laboratory settings. If a cap must be replaced (e.g., for transport to a sharps bin), use a one-handed scoop technique or a mechanical capping device — never two-handed recapping.
- Drop the entire syringe (barrel + bonded needle + cap if used) into an approved rigid-walled, puncture-resistant sharps container immediately after use.
- Do not exceed the fill line (typically 3/4 of container capacity). Overfilled sharps containers increase needlestick risk during handling and pickup.
- Seal and dispose through an institutional biohazard or medical waste vendor according to local regulations (e.g., OSHA Bloodborne Pathogens Standard in the US; EU Directive 2010/32/EU on prevention of sharps injuries; national equivalents elsewhere).
- Document disposal in laboratory waste logs as required by GLP, institutional biosafety, or chain-of-custody protocols.
Sharps container selection:
- Use FDA-cleared or equivalent regional-standard sharps containers (UN3291 or CDC-recommended)
- Containers should be rigid, leak-proof, puncture-resistant, and clearly labelled with the biohazard symbol
- For 0.5 mL insulin-style syringes, a 1-2 quart (1-2 L) container typically holds 100-200 used units — appropriate for several 30-packs
Spill and breakage response: If a syringe blister is damaged in transit or a syringe is dropped post-use, use forceps or a brush-and-dustpan technique to recover the unit. Never handle exposed sharps with bare or gloved hands directly. Decontaminate the affected surface with 70% isopropyl alcohol followed by appropriate disinfectant per the laboratory's biosafety SOP.
Needlestick injury protocol: In the event of accidental needlestick from a syringe used with research peptides, follow institutional post-exposure protocols immediately: wash the wound with soap and water, document the exposure, and consult occupational health. While research peptides are typically non-infectious, exposure documentation is required under OSHA and equivalent regulations.
Aseptic Single-Use Protocol for 0.5 mL 31G 1/4-inch Syringes in Peptide Reconstitution
The individually blistered, sterile, single-use design of the syringes in this 30-pack supports a rigorous aseptic workflow when followed correctly. The protocol below is recommended for routine bench reconstitution of lyophilised research peptides and for low-volume aliquoting into secondary vials.
Step-by-step aseptic use protocol:
- Workspace preparation: Disinfect a flat, clutter-free work surface with 70% isopropyl alcohol. Allow to air-dry (minimum 30 seconds) — do not wipe the residual film, which provides continued antimicrobial action.
- Hand hygiene and PPE: Wash hands with soap and water, dry thoroughly, then don nitrile gloves. Disinfect gloved hands with 70% IPA and allow to dry before handling sterile components.
- Blister inspection: Examine the individual syringe blister for intact seal, no punctures, no discolouration, and a visibly clear barrel. Discard any blister showing compromise.
- Blister opening: Peel the foil/film backing from the corner indicated, exposing the syringe without contacting the plunger flange or needle hub.
- Vial septum disinfection: Wipe the rubber septum of the reconstituted peptide vial with a fresh 70% IPA prep pad and allow to air-dry (minimum 30 seconds).
- Cap removal: Remove the protective tip cap by pulling straight off — do not twist, which can damage the needle hub bond. Do not lay the cap down on a non-sterile surface.
- Septum penetration: Insert the needle through the septum at a 45-60° angle, bevel facing upward, then rotate to vertical as the needle clears the septum. This technique minimises coring of the elastomer.
- Aspiration: Withdraw the plunger slowly and steadily to the desired graduation mark. Avoid rapid pulls that create cavitation bubbles in the solution.
- Bubble removal: If air bubbles are present, tap the barrel gently to coalesce them at the needle hub, then expel back into the vial and re-aspirate to the target volume.
- Withdrawal and use: Withdraw the needle straight out, deliver the aliquot or research dose immediately, and place the used syringe directly into a rigid, puncture-resistant sharps container. Do not recap.
Critical single-use discipline: Each syringe in this 30-pack is intended for one draw and one delivery. Reusing a syringe — even on the same vial — defeats the sterile barrier, dulls the bevel, and introduces particulate and microbial contamination risk. The 30-unit count is designed to support a typical multi-week peptide research campaign with one syringe per scheduled draw, plus margin for repeat draws or accidental contamination events.
Blister Pack Opening Technique and Sterile Field Preservation for the 30-Pack
Individually blistered syringes provide a validated sterile barrier from the point of manufacture to the point of use. Preserving that barrier through the opening sequence is essential to maintain aseptic conditions during peptide reconstitution and dosing workflows. The following technique should be followed for each syringe drawn from the 30-pack:
- Inspect the blister. Before opening, verify that the peelable backing is fully sealed around the perimeter, that no creases or punctures are visible, and that the syringe inside is intact with the tip cap firmly seated. Discard any blister showing damage, discoloration, or signs of moisture ingress.
- Disinfect the work surface. Wipe the immediate bench area with a 70% isopropyl alcohol prep pad and allow at least 30 seconds of contact time for surface decontamination before opening the blister.
- Peel from the labelled corner. Grip the peel tab at the corner indicated by the arrow or notch on the blister. Peel back the foil/film backing in a single smooth motion at approximately 45° to the blister plane. Avoid tearing through the plastic tray, which can release particulate fragments.
- Present syringe barrel-up. Hold the opened blister with the syringe barrel facing upward and the needle hub pointing away from the operator's body. The syringe should remain seated in the moulded tray cavity until needed.
- Grasp the barrel, not the plunger. Lift the syringe by gripping the flange and barrel. Avoid contact with the plunger rod, as fingerprints and skin oils can transfer to surfaces that subsequently contact the inner barrel during plunger depression.
- Remove the tip cap immediately before use. Pull the protective tip cap straight off — do not twist, as twisting can stress the needle hub bond. Discard the cap directly into the sharps container; never set it on the bench for later re-capping.
- Use within 60 seconds of cap removal. Once the needle is exposed, environmental microbial deposition begins. Complete the draw or injection promptly, then dispose of the syringe in a point-of-use sharps container.
Critical aseptic notes: Never re-insert a used needle into the blister tray or attempt to recap. If the syringe is dropped or contacts any non-sterile surface after the tip cap is removed, discard it immediately and open a new blister. Maintain a logbook entry of each syringe used, including blister lot number where available, to support traceability across multi-week research campaigns.
Final Pre-Injection Checklist for Single-Use Allocation of 0.5 mL 31G 1/4-inch Syringes
This checklist consolidates the critical pre-use verification steps for a single syringe drawn from the 30-pack of 0.5 mL 31G 1/4-inch insulin-style syringes. It is designed as a final quality-control gate immediately before vial septum penetration and is intended for laboratory research workflows only.
- Verify lot and expiry on the outer carton. Confirm the carton lot number is recorded in the laboratory notebook or LIMS, and that the labelled expiry date has not been exceeded. Do not use any syringe from a carton with damaged or compromised primary packaging.
- Inspect the individual blister. The blister should be fully sealed on all edges with no peeling, swelling, perforation, or moisture intrusion. Discard any syringe whose blister is breached.
- Open the blister using aseptic technique. Peel from the labelled corner only; do not push the syringe through the lid film, which can compromise sterility of the needle shaft.
- Inspect the syringe visually. Confirm the tip cap is in place and seated; the barrel is transparent and free of cracks, scratches, or visible particulate; the plunger stopper is at the labelled 0 mL position; and the graduation markings are legible and intact.
- Inspect the needle and hub. Confirm the needle is straight (no visible bend), the hub-to-barrel junction is intact, and there is no visible damage to the needle shaft once the cap is removed.
- Verify plunger function. Without removing the tip cap, gently advance and retract the plunger 1-2 mm to confirm smooth glide. Excessive resistance or sticking indicates silicone oil failure or stopper deformation — discard.
- Prepare the vial septum. Wipe the rubber septum with a fresh 70% isopropyl alcohol prep pad and allow to air-dry for ≥30 seconds before penetration.
- Pre-load air equal to the intended draw volume. With the cap still in place, pull the plunger back to the planned aspiration volume (e.g., 0.1 mL). This air will be injected into the vial to equilibrate pressure prior to drawing solution.
- Remove the tip cap immediately before vial access. Do not lay the uncapped syringe on the work surface. Pierce the septum at a 45-90° angle with bevel facing up to minimise coring.
- Inject the air, invert the vial, and aspirate the target volume. Withdraw slowly; tap the barrel to dislodge air bubbles; adjust to the exact target volume on the U-100 scale (or mL equivalent).
- Withdraw the needle and proceed to dosing. Use the same syringe once only. Discard immediately into an approved sharps container after dose delivery.
Documentation: Record the carton lot, syringe sequence number (e.g., 3 of 30), target draw volume, actual aspirated volume, and date/time of use in the laboratory notebook to support GLP-aligned traceability.
Recommended End-to-End Use Protocol: From Blister Opening to Sharps Disposal
The following end-to-end protocol consolidates aseptic technique, dosing accuracy, and disposal best practices into a single workflow for the 0.5 mL 31G 1/4-inch syringe 30-pack. Each unit is supplied individually blister-packed, sterile, with a permanently attached needle and protective tip cap, and is intended for single-use research only.
- Workspace preparation: Clean a non-porous bench surface with 70% isopropyl alcohol and allow it to dry. Lay out a clean absorbent pad, the target peptide vial, an alcohol prep pad, the blistered syringe, a sharps container, and the reconstitution worksheet.
- Hand hygiene and PPE: Wash hands, don nitrile gloves, eye protection, and a lab coat. Avoid touching the syringe barrel near the needle hub after blister opening.
- Blister inspection: Verify the blister seal is intact, with no punctures, swelling, or moisture. Reject any unit with compromised packaging.
- Aseptic opening: Peel the blister back from the plunger end so the needle-and-cap end is exposed last. Do not touch the cap or the barrel hub.
- Vial septum disinfection: Swab the peptide vial septum and bacteriostatic water vial septum with a fresh alcohol prep pad. Allow 30 seconds for contact time and surface drying.
- Cap removal: Pull the protective tip cap straight off without lateral bending. Discard the cap.
- Air pre-load (optional): Pull the plunger to the target volume to load equilibration air, which can be injected into the diluent vial to maintain pressure balance during draw.
- Diluent draw: Insert the needle bevel-up at a 45-60° angle through the centre of the septum to minimise coring. Invert the vial, draw the planned diluent volume, and withdraw the needle.
- Reconstitution: Slowly inject the diluent down the inner wall of the peptide vial. Do not direct the stream onto the lyophilized cake. Gently swirl — never shake — until fully dissolved.
- Dose draw: Using a second fresh syringe from the 30-pack, draw the target research dose volume, then expel any air bubble by tapping the barrel and gently advancing the plunger.
- Single-use discipline: Each syringe from the 30-pack is intended for a single draw-and-deliver event. Do not recap, reuse, or cross-contaminate between vials.
- Sharps disposal: Immediately drop the used syringe, needle-first, into an FDA-cleared puncture-resistant sharps container. Do not bend, break, or manually recap. Seal and dispose of the full container per institutional and local regulations.
Following this protocol consistently across the 30-pack supports reproducible reconstitution and dosing accuracy across multi-week peptide research campaigns while minimising contamination risk and sharps injury exposure.
Standard Operating Procedure: Single-Use Allocation, Aseptic Draw, and Disposal for the 0.5 mL 31G 1/4-inch 30-Pack
This consolidated standard operating procedure (SOP) is intended to support reproducible, aseptic use of the 30-pack across a typical multi-week peptide research campaign. It assumes the operator is working in a Biosafety Level 1 or Level 2 laboratory, has access to 70% isopropyl alcohol prep pads, a rigid sharps container compliant with local regulations, and a sterile work surface or biosafety cabinet.
1. Pre-use inspection (per syringe):
- Confirm the individual blister pack is intact, opaque-printed side legible, and shows no creasing, perforation, or moisture.
- Verify lot number and expiry date are present.
- Peel the blister from the printed corner; do not tear through the sterile barrier. Allow the syringe to drop into a sterile gloved hand or onto a sterile field.
- Visually inspect: barrel free of cracks or particulates, plunger seated, tip cap firmly in place, needle straight and free of burrs.
2. Vial septum preparation:
- Remove the vial flip-cap, exposing the elastomeric septum.
- Swab the septum with a fresh 70% isopropyl alcohol prep pad using a single firm circular motion.
- Allow the septum to air-dry fully (typically 15-30 seconds). Do not blow on or wipe the septum.
3. Aseptic draw:
- Remove the tip cap with a straight pull; do not twist.
- Draw room-air into the syringe equivalent to the volume to be withdrawn (pressure equilibration).
- Insert the 31G needle into the septum at a 45-60° angle, bevel-up, then rotate to vertical once the bevel has fully cleared the septum.
- Inject the air into the headspace above the liquid (avoid bubbling through the solution).
- Invert the vial, ensuring the needle tip is below the liquid meniscus, and slowly aspirate the target volume.
- Tap the barrel to dislodge bubbles, expel any air, and verify the meniscus aligns with the target graduation mark at eye level.
4. Post-draw and disposal:
- Withdraw the needle from the septum at the same angle of entry to minimise septum trauma.
- Do not recap the needle. Immediately discard the entire syringe (needle attached) into a rigid, puncture-resistant sharps container.
- Record the lot number, date, time, draw volume, and operator initials in the reconstitution log.
5. Single-use discipline: Each syringe in the 30-pack is intended for a single draw and single dose. Re-use of the same syringe for a second draw — even from the same vial — compromises sterility, increases coring risk, and introduces particulate carry-over from the prior contents. Plan the 30-pack allocation in advance to ensure adequate syringe inventory across the research campaign.
Multi-Operator Standardisation Protocol for Consistent Dosing with the 30-Pack
When the 30-pack of 0.5 mL 31G 1/4-inch insulin-style syringes is deployed across a research team with multiple operators, inter-operator variability in draw technique, plunger handling, and air-bubble removal can introduce dosing variance that confounds experimental readouts. The following standardisation protocol minimises this variance for low-volume peptide research workflows.
Recommended multi-operator standardisation steps:
- Operator training and calibration. Each operator should perform a minimum of 10 supervised practice draws using bacteriostatic water and an inert practice vial before contributing to active dosing campaigns. Practice draws should target volumes of 0.05 mL, 0.10 mL, and 0.20 mL, with gravimetric verification on a 4-decimal-place balance.
- Standardised draw technique. All operators should adopt identical techniques: bevel-up vial septum penetration at 45–60° angle, vial inversion before aspiration, slow plunger withdrawal at <0.5 mL/s, and a 5-second pause at target volume before needle withdrawal.
- Air-bubble removal protocol. Operators should hold the syringe vertically (needle up), gently tap the barrel to dislodge bubbles, and slowly advance the plunger to expel air. Final volume should be verified against the graduation mark at eye level.
- Volume verification. For research applications requiring <5% coefficient of variation, each draw should be gravimetrically verified or visually confirmed against the graduation scale by a second operator.
- Single-use discipline. Each syringe from the 30-pack should be used for exactly one draw-and-administer event, with immediate disposal into a sharps container. Reuse across multiple draws introduces dead-space loss variability and contamination risk.
- Documentation. Each draw event should be logged with: operator initials, syringe lot number, target volume, observed volume, peptide vial lot, draw timestamp, and any anomalies (visible particulates, plunger resistance, etc.).
- Periodic CV monitoring. Every 10 draws, the team lead should review gravimetric or visual verification data to calculate inter-operator CV. CV >10% should trigger retraining.
- Lot allocation. When practical, allocate syringes from a single lot of the 30-pack to a given experimental arm to minimise lot-to-lot manufacturing variance contributions to dosing variability.
Expected performance. With this standardisation protocol, research teams using the 30-pack of 0.5 mL 31G 1/4-inch syringes can typically achieve inter-operator dosing CV <7% at draw volumes ≥0.10 mL and CV <12% at draw volumes between 0.05–0.10 mL, consistent with ISO 8537 performance benchmarks for insulin-style syringes in research applications.
Recommended Aseptic Draw Protocol for 31G 1/4-inch Syringes from Single-Vial Peptide Stocks
The following protocol describes the recommended single-use aseptic draw workflow for the 0.5 mL 31G 1/4-inch syringes in this 30-pack, optimised for repeatable draws from rubber-septum-sealed multi-dose peptide vials. This workflow assumes the peptide vial has been reconstituted previously and is being accessed for a routine research dose.
- Workspace preparation. Wipe the work surface with 70% isopropyl alcohol and allow to air-dry (minimum 30 seconds contact time). Assemble required materials: one blister-packed syringe from the 30-pack, the target peptide vial, a fresh alcohol prep pad, and a sharps container within arm's reach.
- Hand hygiene and PPE. Perform hand hygiene per laboratory SOP. Don nitrile examination gloves; verify glove integrity before proceeding.
- Vial septum disinfection. Remove the cap from the peptide vial (if first access). Wipe the rubber septum with a fresh 70% IPA prep pad using firm circular motion for 5 seconds; allow to air-dry for a minimum of 30 seconds to ensure full antiseptic activity.
- Syringe removal. Open the individual blister pack by peeling the foil backing — do not push the syringe through the foil, as this risks contamination of the barrel. Remove the syringe, retaining the protective tip cap until immediately before vial access.
- Air pre-loading (optional). Draw air into the syringe equal to the target draw volume (e.g. 0.10 mL air for a 0.10 mL peptide draw). This step equalises vial pressure during withdrawal and minimises bubble formation. Remove the tip cap and place it on the disinfected work surface (or discard).
- Vial septum penetration. Hold the vial upright on a stable surface. Insert the 31G needle bevel-up at a 45-90° angle through the rubber septum using a single smooth motion. Avoid lateral movement during penetration to minimise septum coring.
- Air injection and inversion. Inject the pre-loaded air into the vial headspace. Invert the vial so the needle tip remains submerged in solution; ensure the bevel is fully below the liquid level to prevent air aspiration.
- Solution draw. Slowly withdraw the plunger to draw solution to a volume slightly above the target (typically +0.02-0.05 mL above target). Pause briefly to allow any aspirated micro-bubbles to rise toward the plunger.
- Bubble removal and volume adjustment. With the syringe still inserted and vial inverted, gently tap the syringe barrel to coalesce air bubbles at the plunger end. Slowly push the plunger to expel air and excess solution back into the vial until the meniscus aligns exactly with the target graduation.
- Needle withdrawal. Withdraw the needle from the septum in a single smooth motion at the same angle of insertion. Verify the final draw volume against the graduation scale.
- Immediate single-use disposal. After the syringe is used for its intended research application, dispose of the entire syringe-needle assembly directly into a rigid-wall sharps container. Do NOT recap the needle (recapping is the leading cause of needlestick injuries).
- Vial closure. Wipe the vial septum with a fresh alcohol prep pad and return the vial to appropriate storage (typically 2-8°C for reconstituted peptide stocks).
Critical practice points: Each syringe in the 30-pack is intended for single-use only. Re-use across multiple draws, vials, or experimental subjects compromises sterility, increases dead-space loss variability, and risks needle-tip lubricant depletion that degrades subsequent draw accuracy.
Standardised Single-Use Allocation Protocol for the 0.5 mL 31G 1/4-inch 30-Pack
The 30-pack configuration is engineered around a strict single-use, single-blister-per-event workflow. Adherence to a standardised allocation protocol preserves sterility, dosing reproducibility, and traceability across a multi-week peptide research campaign.
- Inventory check on receipt: Confirm pack contains 30 individually blistered syringes. Inspect each blister for intact seal, no creases, no moisture ingress, and legible lot/expiry markings on the outer pack.
- Workspace preparation: Clean a non-porous bench surface with 70% isopropyl alcohol prep pads. Allow to air-dry (≥30 seconds) before placing sterile materials. Position sharps container within arm's reach (≤30 cm).
- Blister opening technique: Peel back from the marked corner using gloved hands. Do not push syringe through the foil. Transfer the syringe to the sterile field grasping the barrel only — do not touch the needle hub, cap, or plunger flange.
- Cap removal: Hold the syringe barrel; pull the needle cap straight off in one motion. Do not twist or recap.
- Vial septum disinfection: Wipe the peptide vial septum with a fresh alcohol prep pad. Allow ≥30 seconds for evaporation.
- Aspiration: Insert needle at a 60-75° angle, bevel up, through the central marked zone of the septum. Inject equivalent air volume if drawing >0.10 mL to equilibrate vial pressure. Invert vial and aspirate slowly (≥3 seconds per 0.10 mL).
- Air bubble removal: Tap barrel gently; expel air back into the vial. Read meniscus at lower edge of target graduation mark at eye level.
- Withdrawal and immediate disposal: Withdraw needle from septum without recapping. Discard the entire syringe into the sharps container immediately. Never reuse the syringe across draws, vials, or experimental events.
- Documentation: Record lot number, draw volume, operator initials, and timestamp in the laboratory notebook or LIMS for each syringe used.
Allocation across a 4-week campaign: A typical 30-pack supports one reconstitution-and-draw event per day for 28-30 days, or two daily events for a 14-day intensive protocol. Plan allocation in advance and segregate any reserved units in a clean secondary container to prevent accidental cross-use.
Recommended End-of-Campaign Audit and Inventory Reconciliation for the 30-Pack
At the conclusion of a multi-week peptide research campaign using the 0.5 mL 31G 1/4-inch 30-pack, a structured end-of-campaign audit supports reproducibility, traceability, and GLP-aligned documentation. The single-use, individually blistered format of this 30-pack lends itself to a per-syringe reconciliation that links each used syringe to a specific reconstitution or dosing event.
Recommended audit workflow:
- Syringe count reconciliation: Confirm that the number of used blister wrappers (retained in a dedicated tally bag) plus unused syringes equals 30. Any discrepancy warrants investigation — missing wrappers may indicate undocumented draws.
- Sharps log cross-reference: Each used syringe should correspond to a single dated entry in the sharps log, with peptide identity, vial lot, draw volume, and operator initials recorded. Cross-reference the log against the experimental dosing schedule.
- Lot traceability: Record the syringe lot number (printed on the outer 30-pack box) in the laboratory notebook. In the event of a downstream anomaly (e.g., unexpected dosing variance), lot traceability supports root-cause analysis.
- Unused syringe disposition: Unused syringes from the 30-pack remain sterile within their intact blister wrappers and may be retained for the next campaign provided storage conditions have been controlled (15-25°C, dry, protected from direct sunlight) and the manufacturer expiry date has not passed.
- Sharps container closure: When the sharps container reaches the 3/4-full line, close, seal, and label per institutional biohazard waste protocol. Do not overfill.
- Reconstitution record archival: File the reconstitution worksheet and sharps log with the experimental records. Retention period should follow institutional GLP or ISO 9001 documentation standards (typically ≥5 years for regulated research).
Inventory planning for follow-on campaigns: A typical 4-week peptide research campaign consumes 21-28 syringes (1 reconstitution draw + 1 dose every 2-3 days × 1-2 peptides). The 30-pack therefore provides a small buffer for repeat draws, accidental contamination of a blister, or operator training. For campaigns exceeding 4 weeks or involving ≥3 concurrent peptides, plan for a second 30-pack to maintain single-use discipline without rationing syringes across multiple vials.
Common audit findings and corrective actions: Discrepancies most commonly arise from (a) undocumented draws during reconstitution troubleshooting, (b) wasted syringes due to blister damage discovered after opening, or (c) operator turnover without handover documentation. A short pre-campaign briefing covering single-use discipline, sharps log entry standards, and blister inspection mitigates each of these failure modes.
End-to-End Aseptic Use Protocol for the 0.5 mL 31G 1/4-inch 30-Pack in Single-Vial Peptide Reconstitution
The following standardised protocol describes single-use allocation of one syringe from the 30-pack per reconstitution or dosing event, with explicit aseptic technique steps to preserve sterility of both the syringe and the multi-dose peptide vial across a research campaign.
1. Workspace and PPE preparation:
- Disinfect a clean bench surface with 70% isopropyl alcohol (IPA) and allow ≥30 seconds contact time before placing materials.
- Don nitrile gloves, lab coat, and safety glasses. Confirm sharps container is within arm's reach.
- Assemble: one blistered 0.5 mL 31G 1/4-inch syringe, the lyophilised peptide vial, bacteriostatic water vial, two alcohol prep pads, and a labelling pen.
2. Component inspection:
- Inspect the syringe blister pack for intact heat-seal, absence of moisture ingress, and no visible damage to the plunger or needle hub through the transparent backing.
- Confirm the lot number and expiry date are legible on the blister.
- Inspect the peptide vial for intact crimp seal, undisturbed lyophilised cake, and absence of meltback or discoloration.
3. Syringe deployment:
- Peel the blister pack from the corner indicated by the manufacturer arrow, avoiding contact with the syringe barrel or needle cap.
- Remove the protective tip cap with a straight pull. Do not twist — the 31G thin-wall needle is susceptible to bevel deformation from lateral force.
- Visually inspect the needle bevel under good lighting for burrs, bend, or coring damage. Discard if any defect is observed.
4. Aseptic draw:
- Wipe the rubber septum of the bacteriostatic water vial with a fresh alcohol prep pad in a single unidirectional stroke. Allow 30 seconds drying time.
- Draw the target volume of bacteriostatic water (typically 1.0-2.0 mL across multiple syringe draws, or use a larger constitution syringe if available).
- Penetrate the peptide vial septum at a 45° angle, bevel-up, to minimise coring. Rotate to 90° once the bevel has cleared the septum, and dispense the diluent slowly down the vial wall — not directly onto the lyophilised cake.
- Withdraw the needle, swirl gently (do not shake or vortex), and allow full dissolution before further handling.
5. Single-use discipline and disposal:
- Discard the used syringe immediately into the sharps container — never recap, bend, or reuse.
- Document the lot number, reconstitution date, diluent volume, and final concentration in the laboratory notebook or LIMS.
- Allocate one fresh syringe from the 30-pack per subsequent draw or dosing event.
This single-use allocation pattern preserves the dimensional integrity of the plunger stopper and needle bevel, eliminates cross-contamination risk between draws, and supports reproducibility across multi-week research campaigns.
Recommended Single-Use Allocation, Aseptic Draw, and Disposal Sequence for the 0.5 mL 31G 1/4-inch 30-Pack in Multi-Peptide Research Campaigns
The 30-pack is configured to support a single-use, one-syringe-per-draw discipline across multi-week peptide research campaigns. The following standard operating procedure (SOP) consolidates the aseptic, mechanical, and disposal best practices documented across this product page into a single end-to-end workflow.
1. Pre-use inspection (≤30 seconds per syringe):
- Confirm that the individual blister pack is intact, with no punctures, creases, or seal compromise.
- Check the blister for lot number and expiry date; record both in the research notebook for chain-of-custody documentation.
- Open the blister using a peel-back technique from the marked corner — never tear, which can release particulates onto the sterile syringe surface.
- Visually inspect the syringe for: clear barrel with no haze or particulates, intact tip cap, plunger fully retracted and centred, and 31G needle straight with no visible bevel damage.
2. Aseptic vial septum penetration:
- Wipe the peptide vial septum with a 70% isopropyl alcohol prep pad and allow 30 seconds for evaporation.
- Remove the syringe tip cap by pulling straight (do not twist), and avoid touching the needle to any non-sterile surface.
- Penetrate the septum at a 45-90° angle with bevel-up orientation to minimise coring of rubber particulates into the peptide solution.
- Draw the desired volume slowly to avoid cavitation and foaming, which can promote peptide aggregation. For volumes <0.10 mL, draw slightly over-volume and expel back to the target graduation to improve gravimetric accuracy.
3. Volumetric verification:
- Hold the syringe vertically (needle up) and tap to consolidate any air bubbles at the hub.
- Expel air with a gentle plunger push; verify the meniscus aligns with the target graduation line on the U-100 insulin scale (1 unit = 0.01 mL).
- For research applications requiring documented gravimetric accuracy, periodically tare-and-weigh a representative subset of draws to confirm volumetric performance against ISO 8537 limits.
4. Single-use discipline and disposal:
- Never recap the needle — recapping is the leading cause of needlestick injuries in research laboratories. Modern sharps protocols universally prohibit recapping.
- Immediately deposit the used syringe — needle attached, plunger fully depressed — into an FDA-approved rigid-wall sharps container located within arm's reach of the workstation.
- Record the syringe lot number, draw volume, source vial ID, and timestamp in the research notebook before moving to the next operation.
- Do not reuse the syringe for a second draw, even from the same vial. Permanently bonded 31G needles dull after a single septum penetration, increasing coring risk on subsequent uses, and re-entry compromises the sterility of the multi-dose vial.
5. End-of-session reconciliation:
- At the end of each reconstitution or dosing session, reconcile the count of used syringes against planned draws to confirm no syringes have been lost or misplaced.
- Verify that the sharps container is below 75% fill capacity; replace as needed per institutional biohazard protocols.
- Update the campaign inventory log: 30-pack allocation, syringes remaining, and projected syringes required for the remainder of the campaign.
This SOP supports reproducible, GLP-aligned peptide research workflows while minimising contamination risk, dosing error, and sharps injury exposure across multi-week experimental campaigns. The 30-pack quantity is calibrated to support a typical 4-week single-operator, single-peptide reconstitution and dosing campaign, with margin for occasional re-draws or quality-control verifications.
Recommended Bevel-Up 45° Insertion Technique for 31G 1/4-inch Vial Septum Penetration
Optimal use of the 31G 1/4-inch needles supplied in this 30-pack for vial septum penetration during peptide reconstitution depends on consistent operator technique. Following a standardised insertion protocol minimises septum coring, preserves needle bevel sharpness for downstream draws, and reduces particulate burden in reconstituted peptide solutions.
Recommended insertion protocol:
- Remove syringe from individual blister pack using aseptic technique, retaining the tip cap until immediately before use
- Inspect needle visually for bevel integrity, straightness, and absence of burrs or contamination
- Disinfect vial septum with a 70% isopropyl alcohol prep pad using a single wiping motion; allow 30 seconds of contact time for evaporation
- Remove tip cap by pulling straight off — do not twist, which can introduce shear stress on the needle hub
- Orient bevel facing up (the sloped face of the needle tip pointed upward toward the vial neck)
- Insert needle at 45° angle to the septum surface, applying gentle steady pressure to advance the tip through the elastomer
- Rotate syringe to 90° (vertical) once the needle has fully penetrated the septum, before initiating aspiration
- Equalise vial pressure by injecting a volume of air equivalent to the volume to be withdrawn (typically 0.10–0.30 mL)
- Aspirate slowly at approximately 0.1 mL/sec to minimise turbulence and foaming of reconstituted peptide solution
- Withdraw needle in a single smooth motion, maintaining bevel-up orientation to preserve septum self-sealing
- Dispose of syringe immediately into a designated sharps container — do not recap or reuse
Critical handling notes:
- The 1/4-inch (6 mm) cannula length is sufficient for full penetration of standard 13 mm and 20 mm vial septa (typical septum thickness 3–4 mm), leaving 2–3 mm of cannula inside the vial headspace
- For viscous reconstitutions or cold solutions drawn directly from refrigerated stocks, allow the vial to equilibrate to room temperature (15–20 min) before aspiration to reduce draw resistance
- If multiple penetrations of the same vial are anticipated across a research campaign, rotate the insertion point around the central septum region rather than reusing the same penetration site, which preserves septum self-sealing integrity
- Document each penetration event (date, time, operator, syringe lot) on the vial label or in the laboratory notebook to support chain-of-custody traceability
Adherence to this protocol supports reproducible dosing accuracy across the 30 single-use syringes supplied in the pack and minimises cumulative septum degradation across the typical 28-day reconstituted vial beyond-use period.
Recommended Aseptic Single-Use Workflow for the 0.5 mL 31G 1/4-inch 30-Pack
The individually blistered packaging of this 30-pack supports a strict single-use aseptic workflow that minimises cross-contamination between peptide vials and preserves dosing reproducibility across a multi-week research campaign. The following protocol summarises best-practice handling for laboratory peptide reconstitution and low-volume aliquoting.
- Pre-use inspection: Examine the blister for intact seal, no punctures, no discolouration. Discard any blister where the sterile barrier is compromised.
- Workspace preparation: Disinfect a flat work surface with 70% isopropyl alcohol. Allow 30 seconds contact time before placing components.
- Hand hygiene and PPE: Wash hands, don nitrile gloves, and wipe gloves with 70% IPA. Eye protection recommended.
- Vial septum prep: Swab the rubber septum of the peptide vial and the bacteriostatic water vial with a fresh alcohol prep pad. Allow to air-dry for 15-30 seconds.
- Blister opening: Peel the blister from the labelled end to expose the plunger flange. Avoid touching the needle shaft or barrel below the flange.
- Tip cap removal: Remove the protective tip cap with a straight pull. Do not recap before use.
- Air injection (optional): For bacteriostatic water draws, pull plunger to the target volume of air, insert needle bevel-up at 45°, and inject air into the vial headspace to equalise pressure.
- Aspiration: Invert the vial, ensure the needle tip is submerged, and slowly withdraw the target volume. Tap to dislodge bubbles and adjust to exact graduation.
- Septum withdrawal: Withdraw the needle in a single smooth motion to minimise coring and self-seal the septum.
- Immediate disposal: Discard the used syringe directly into an FDA-cleared sharps container. Do not recap, bend, or detach the needle.
Single-use discipline: Each syringe in the 30-pack is intended for one workflow event — typically either an initial reconstitution draw or a single dosing draw. Reuse across multiple vials or multiple draws risks septum coring particulate accumulation, bevel deformation, and microbial cross-contamination. The 30-syringe count is designed to support approximately 4 weeks of single-use allocation in a typical research campaign reconstituting 1-2 peptide vials per week.
Single-Use Aseptic Draw Protocol Using the 0.5 mL 31G 1/4-inch Syringe from This 30-Pack
The following protocol describes the recommended aseptic single-use workflow for drawing reconstituted peptide solution from a multi-dose vial using one syringe from this 30-pack. It is designed to maximise dosing reproducibility, preserve vial sterility for subsequent draws, and minimise sharps injury risk during research bench work.
- Workspace preparation: Clean the work surface with 70% isopropyl alcohol and allow to air-dry. Position a sharps container within arm's reach. Lay out the unopened blister syringe, the reconstituted peptide vial, and a fresh alcohol prep pad.
- Hand hygiene & PPE: Wash hands and don nitrile gloves. Nitrile is preferred over latex for compatibility with peptide and solvent residues.
- Vial septum disinfection: Wipe the rubber septum of the reconstituted peptide vial with a 70% isopropyl alcohol pad using a single-direction stroke. Allow the septum to air-dry for 30 seconds — this ensures full antiseptic kill time without introducing residual alcohol into the draw.
- Blister opening: Peel the blister pack open from the indicated tear-notch in a single smooth motion. Do not tear through the syringe body. Remove the syringe by the barrel — avoid touching the needle hub or tip cap.
- Syringe inspection: Confirm the plunger moves freely, the barrel is free of cracks, the needle tip cap is intact, and graduation markings are legible. Reject and replace any syringe failing inspection.
- Pre-draw air pull: Remove the tip cap. Pull the plunger back to draw an air volume equivalent to the intended peptide draw volume. This air will be injected into the vial to equalise pressure and prevent vacuum on aspiration.
- Vial septum penetration: Hold the vial upright on the bench. Insert the 31G needle at a 45° bevel-up angle, then straighten to 90° once the bevel is through the septum. This minimises septum coring.
- Pressure equalisation: Inject the pre-loaded air into the vial headspace, not into the liquid.
- Invert and draw: Invert the vial. Position the needle tip below the liquid meniscus. Slowly withdraw the plunger to the target volume mark. Tap the barrel to dislodge air bubbles, then expel any air back into the vial.
- Final volume confirmation: Re-verify the meniscus aligns with the target graduation mark at eye level.
- Needle withdrawal: Withdraw the needle from the septum in a single smooth motion. Do not recap.
- Immediate use or discard: Deliver the dose promptly. Discard the entire syringe and needle as a single unit into the sharps container immediately after use — do not reuse for any subsequent draw.
Single-use discipline is non-negotiable: each syringe in this 30-pack is designed for one vial septum penetration and one draw. Reusing a syringe across multiple vials introduces cross-contamination risk; reusing on the same vial degrades needle bevel sharpness and increases coring on subsequent penetrations.
Standardised Aseptic Single-Use Protocol for the 0.5 mL 31G 1/4-inch 30-Pack in Peptide Research Workflows
The following standardised aseptic protocol consolidates best practices for single-use allocation, sterile draw, and disposal of the 0.5 mL 31G 1/4-inch syringes supplied in this 30-pack. The workflow is designed for typical research peptide reconstitution and low-volume aliquoting from multi-dose vials sealed with butyl or chlorobutyl rubber septa.
- Workspace preparation: Clean the bench surface with 70% isopropyl alcohol and allow to air-dry for at least 30 seconds. Position a sharps container within arm's reach.
- Pre-use inspection: Hold the blister package under good lighting and confirm the seal is intact, the barrel is free of cracks, the plunger is fully seated, and the protective needle cap is in place.
- Aseptic peel-open: Grasp the blister tabs and peel apart slowly to expose the syringe. Do not touch the needle cap or the plunger flange to the bench surface or to gloved fingers.
- Vial septum disinfection: Wipe the peptide vial septum with a fresh 70% isopropyl alcohol prep pad in a single direction and allow 15-30 seconds for evaporation.
- Air pre-load (optional pressure-equilibration step): Pull the plunger to draw a volume of air equal to the intended aspiration volume.
- Needle insertion: Hold the syringe at a 45-degree angle with bevel facing up and insert through the centre of the vial septum. This orientation minimises coring risk and preserves septum self-sealing for subsequent draws.
- Air injection and draw: Invert the vial, depress the plunger to inject the pre-loaded air, then slowly aspirate the desired volume. Tap the barrel to displace any air bubbles toward the hub and expel them back into the vial.
- Needle withdrawal: Withdraw the needle vertically without lateral motion to avoid enlarging the septum puncture.
- Immediate disposal: Without recapping, deposit the entire syringe into the sharps container.
- Documentation: Record the date, peptide lot, draw volume, and syringe lot in the reconstitution log for chain-of-custody traceability.
Single-use discipline: Each syringe in this 30-pack is supplied sterile in an individually sealed blister and is intended for one draw and one disposal cycle. Reuse across multiple vials or multiple draws compromises sterile workflow and introduces cross-contamination risk; bevel sharpness also degrades after a single septum penetration, increasing coring risk on subsequent uses.
Recommended Quality-Audit Checklist for the 30-Pack on Receipt and Before Single-Use Allocation
A structured pre-use quality audit of the 0.5 mL 31G 1/4-inch syringes in this 30-pack supports reproducible peptide research workflows and aligns with Good Laboratory Practice (GLP) documentation expectations. The following checklist should be completed on receipt of the carton and again immediately before each single-use allocation event.
On receipt (carton-level audit):
- Inspect outer packaging for crush damage, water staining, or evidence of temperature excursion (e.g., ice crystal damage to printed labels).
- Verify lot number and expiry date on the carton match the certificate of conformity or shipping documentation.
- Confirm 30-unit count by visual inspection — each syringe should be in its own intact blister pouch.
- Check for blister-pack damage: any pouch with visible tears, punctures, or compromised seals should be quarantined and not used.
- Record receipt in laboratory inventory log with date, lot number, expiry, and operator initials.
Before each single-use allocation (per-syringe audit):
- Verify blister integrity immediately before peeling — sterile barrier must be intact.
- Peel open from the indicated corner using a gloved hand on a disinfected work surface; do not tear across the syringe body.
- Inspect the syringe under good lighting for: (a) cracked barrel, (b) detached or bent needle, (c) missing protective tip cap, (d) plunger stopper out of position (should be at the 0.5 mL mark or fully advanced).
- Test plunger movement by gently retracting and re-advancing the plunger 2-3 mm to confirm free, consistent glide.
- Verify needle bevel is undamaged and sharp by visual inspection (do not touch).
- Document syringe number in batch reconstitution worksheet (e.g., "Syringe 7 of 30, Lot ACR-2026-04").
Disposition of failed audit units: Any syringe failing the pre-use audit should be discarded into the sharps container with a documentation note ("defective — bent needle") and excluded from the workflow. A failure rate exceeding 2% across the 30-pack warrants a quality complaint to the supplier with photographic evidence and lot reference.
Audit log retention: Pre-use audit records should be retained alongside reconstitution worksheets for the duration of the research campaign plus the institutional retention period (typically 5-10 years for GLP-aligned work).
Recommended Aseptic Workflow for Drawing Reconstituted GLP-1 Analogue Stocks Using the 0.5 mL 31G 1/4-inch 30-Pack
Reconstituted GLP-1 receptor agonist research stocks (semaglutide, tirzepatide, retatrutide, cagrilintide) require a disciplined single-use aseptic draw workflow to preserve vial sterility across the typical 28-day reconstituted shelf life and to maintain dosing accuracy at the sub-0.10 mL draw volumes common in low-dose research applications. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are well-matched to this workflow because of their fine gauge, short cannula, low dead-space, and individually blistered sterile presentation.
Step-by-step aseptic draw protocol:
- Workspace preparation: Disinfect the bench surface with 70% isopropyl alcohol and allow to air-dry for at least 30 seconds. Lay out a single blistered syringe, an alcohol prep pad, and the reconstituted peptide vial within an arm's reach.
- Vial septum disinfection: Wipe the rubber septum of the reconstituted GLP-1 analogue vial with a 70% isopropyl alcohol prep pad using a single firm rotational motion. Allow to air-dry for a minimum of 30 seconds — this is the validated contact time for alcohol-mediated bacterial reduction on elastomeric septa.
- Blister opening: Peel the syringe blister from the flange-end (paper side) rather than tearing through the plastic. Avoid contact between gloved fingers and the needle hub or barrel exterior near the cannula.
- Pre-pressurisation: Withdraw the plunger to the volume equal to the intended draw (e.g., 0.05 mL for a 100 µg dose from a 5 mg/mL stock). Insert the 31G 1/4-inch needle through the vial septum at a 45° bevel-up angle to minimise coring, then advance to vertical. Inject the air bolus to equalise vial pressure.
- Solution withdrawal: Invert the vial, ensure the needle tip is submerged in solution, and slowly withdraw the plunger to the target volume. Draw an additional 0.02 mL of air to enable bubble removal.
- Bubble removal: With the vial still inverted, tap the syringe barrel gently to coalesce bubbles at the needle hub. Advance the plunger to expel air and excess solution back into the vial, stopping precisely at the target volume.
- Needle withdrawal and immediate use: Withdraw the needle from the septum at the same 45° angle used for insertion. Deliver the dose immediately — do not re-cap the needle (scoop-cap technique only if absolutely required) and do not allow the needle to contact any non-sterile surface.
- Single-use disposal: Discard the entire syringe-needle unit into a rigid sharps container immediately after use. Do not reuse for a subsequent draw under any circumstances.
Workflow notes specific to GLP-1 analogues: Reconstituted GLP-1 analogue stocks are typically stable for 28 days at 2-8°C. Allow the vial to equilibrate to room temperature for 5-10 minutes before drawing to reduce solution viscosity and improve aspiration flow rate through the thin-wall 31G cannula. Never shake or vortex the vial — invert gently to mix if visual inspection suggests sedimentation. The 1/4-inch needle length supports research workflows where vial septum penetration is followed by immediate delivery into a downstream receiver (cell culture well, injection-site model, or cryovial for aliquoting).
Recommended Single-Use Aseptic Draw Protocol for the 0.5 mL 31G 1/4-inch 30-Pack
The 0.5 mL 31G 1/4-inch insulin-style syringes supplied in this 30-pack are intended for single-use aseptic allocation in laboratory research workflows. Each individually blistered unit should be allocated to a single draw event from a single reconstituted peptide vial and discarded into an appropriate sharps container after use. The following protocol describes the recommended aseptic workflow for routine peptide research draws.
Step-by-step aseptic draw protocol:
- Workspace preparation. Disinfect a clean, flat bench surface with 70% isopropyl alcohol and allow to air-dry for at least 30 seconds. Arrange a sharps container within arm's reach.
- Hand hygiene and PPE. Wash hands, don nitrile gloves, and disinfect gloved fingertips with 70% IPA. Wear safety eyewear.
- Vial inspection. Inspect the reconstituted peptide vial for clarity, absence of particulates, and intact crimp seal. Disinfect the vial septum with a 70% IPA prep pad using a single-direction wipe and allow to dry for 15-30 seconds.
- Blister inspection and peel. Inspect the individual blister pack for intact sterile barrier — no punctures, no peel-tab separation, no moisture. Peel the blister open from the marked tab end without touching the syringe barrel or needle hub.
- Syringe inspection. Confirm the protective tip cap is intact, the plunger moves freely without sticking, the barrel is free of visible particulates, and the needle is straight with no visible burrs.
- Plunger priming. Pull the plunger back to draw approximately the intended dose volume of air into the syringe.
- Vial pressure equilibration. Remove the protective tip cap. Insert the 31G needle through the vial septum at a 45-90° bevel-up angle. Invert the vial and gently inject the air bolus to equalise vial pressure.
- Aspiration. With the vial inverted and the needle tip below the meniscus, slowly aspirate the target volume. Allow 3-5 seconds for the thin-wall 31G cannula to deliver smooth flow.
- Air-bubble removal. Tap the barrel to consolidate any micro-bubbles at the hub, then gently advance the plunger to expel air back into the vial. Re-aspirate if needed to achieve the precise target volume on the U-100 graduation scale.
- Withdrawal and delivery. Withdraw the needle vertically from the septum. Proceed to the research delivery step without recapping.
- Disposal. Discard the entire syringe — including needle — directly into the sharps container. Do not recap, bend, or reuse.
Workflow notes. Each syringe in this 30-pack is intended for a single draw-and-deliver cycle. Repeated use of the same syringe across multiple vials introduces cross-contamination risk and progressive bevel degradation. Allocating one syringe per draw event maintains aseptic discipline and supports GLP-aligned chain-of-custody documentation across multi-week peptide research campaigns.
Recommended Aseptic Single-Use Allocation, Inspection, and Disposal Workflow for the 0.5 mL 31G 1/4-inch 30-Pack
The 30-pack configuration of individually blistered 0.5 mL 31G 1/4-inch insulin-style syringes is designed for single-use aseptic allocation across a multi-week peptide research campaign. The following workflow standardises inspection, draw, and disposal to maximise dosing reproducibility and minimise contamination risk.
- Receipt inspection. Confirm outer carton integrity, count to verify 30 individual blister packs, and check that each blister is sealed with no visible delamination or moisture ingress. Record lot number and receipt date in the research log.
- Storage. Store unopened at controlled room temperature (15-25°C / 59-77°F), away from direct sunlight and excessive humidity. Do not refrigerate. Functional shelf life of an unopened, undamaged blister is typically 3-5 years from the manufacture date.
- Pre-use inspection. Before opening each blister, inspect for clarity of the barrel, absence of plunger displacement, and bevel orientation visible through the cap. Reject any unit with visible particulates, plunger displacement, or compromised packaging.
- Aseptic blister opening. Wipe gloved hands and work surface with a 70% isopropyl alcohol prep pad. Peel the blister open at the corner indicated, exposing only the barrel — do not touch the needle cap or plunger tip.
- Vial septum disinfection. Wipe the peptide vial septum with a fresh 70% IPA prep pad, allow 30 s contact time, and let air-dry.
- Aspiration draw. Remove the needle cap, pull back the plunger to draw an air volume equal to the target draw, invert the vial, insert the needle at a 45-90° bevel-up angle, inject air, and aspirate the target volume. Tap to dislodge air bubbles and adjust plunger to remove dead-space.
- Single-use discipline. Do not recap, do not reuse on a second vial, do not share across operators or peptides.
- Sharps disposal. Immediately discard the used syringe into a puncture-resistant FDA-cleared or equivalent sharps container located within arm's reach of the workspace.
- End-of-campaign reconciliation. At campaign close, count remaining blisters against the original 30-unit allocation, reconcile against the dosing log, and document any deviations.
This workflow aligns with USP <797> aseptic compounding principles, ISO 8537 insulin syringe handling guidance, and CDC sharps-injury prevention recommendations for research laboratory settings.
Recommended Bench-Top Workflow for Single-Vial Reconstitution Using the 0.5 mL 31G 1/4-inch 30-Pack with Standard Bacteriostatic Water Diluent
The following bench-top workflow standardizes single-vial peptide reconstitution using one syringe from the 30-pack and a separately supplied bacteriostatic water vial. This protocol is designed to maximize aseptic integrity, minimize septum coring, and produce reproducible final peptide concentrations across multi-week research campaigns.
- Workspace preparation: Disinfect a flat bench surface with 70% isopropyl alcohol and allow to air-dry for ≥30 seconds. Lay out a clean absorbent pad as a sterile field.
- Hand hygiene and PPE: Wash hands, don nitrile gloves, and verify safety glasses are in place.
- Component inspection: Inspect the lyophilized peptide vial for intact crimp seal, white powder cake, and absence of moisture. Inspect the bacteriostatic water vial for clarity and intact seal. Inspect the blistered syringe for intact pouch, clear barrel, and free-moving plunger.
- Septum disinfection: Wipe the rubber septum of both vials with a fresh 70% isopropyl alcohol prep pad. Allow ≥30 seconds of contact time.
- Blister opening: Peel the syringe blister at the indicated tab using both hands. Avoid touching the needle cap with non-sterile fingers. Drop the syringe onto the sterile field or grasp by the barrel.
- Tip cap removal: Pull the rigid tip cap straight off without twisting. Do not recap.
- Air injection (optional): Draw 0.5 mL of air into the syringe, insert into the bacteriostatic water vial at a 45° bevel-up angle, and inject the air to equalize pressure.
- Diluent aspiration: Invert the vial, withdraw the desired diluent volume (typically 1.0-3.0 mL across multiple syringe transfers if >0.5 mL is needed), and withdraw the needle.
- Slow vial-wall delivery: Insert the syringe into the peptide vial septum at 45° bevel-up. Direct the diluent stream against the inner vial wall — do not spray directly onto the peptide cake. Withdraw the syringe.
- Gentle dissolution: Swirl the vial slowly. Do not shake or vortex. Allow 2-5 minutes for full dissolution.
- Final inspection: Confirm the reconstituted solution is clear and free of particulates. Label the vial with peptide name, concentration, reconstitution date, and operator initials.
- Sharps disposal: Discard the used syringe immediately into an approved sharps container. Do not recap.
This workflow consumes one syringe per reconstitution event. For multi-vial campaigns, allocate one syringe per vial reconstitution plus additional syringes for subsequent dosing draws — typical 4-week campaigns with 2 vials and twice-weekly dosing consume 10-12 syringes from the 30-pack, leaving substantial reserve for parallel workflows or contingencies.
Recommended Operator Workflow for Drawing Sub-0.10 mL Volumes Accurately Using the 0.5 mL 31G 1/4-inch 30-Pack
Microgram-scale peptide research dosing frequently requires draw volumes below 0.10 mL (10 insulin units on a U-100 scale), where small absolute volumetric errors translate to disproportionately large percentage dose deviations. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are graduated in 1-unit (0.01 mL) increments on a U-100 scale, supporting accurate sub-0.10 mL draws when paired with disciplined operator technique.
Recommended step-by-step protocol:
- Calculate target volume in U-100 units. Convert the required peptide dose (μg) to volume (mL) using the reconstituted vial concentration, then multiply by 100 to obtain the target unit reading (e.g., 0.05 mL = 5 units).
- Sanitise the vial septum with a fresh 70% isopropyl alcohol prep pad and allow to air-dry for at least 15 seconds.
- Inject air equal to the target draw volume into the vial headspace to equilibrate pressure. This minimises vacuum-induced air ingress at the bevel during withdrawal.
- Invert the vial and position the needle bevel below the meniscus. Draw slowly (over 3-5 seconds) to minimise turbulence and air entrainment.
- Overdraw by 1-2 units, then tap the barrel to mobilise any small air bubbles toward the hub.
- Expel air and excess volume back into the vial until the plunger leading edge aligns precisely with the target unit graduation, read at eye level.
- Withdraw the needle and proceed promptly to dose delivery to minimise polypropylene adsorption and silicone oil migration effects.
Accuracy considerations: ISO 8537 specifies a maximum tolerance of ±5% at full nominal volume and ±10-20% at minimum graduated volumes for insulin-style syringes. Gravimetric validation data suggest coefficient of variation (CV) of approximately 2-4% at 0.10 mL draws and 4-7% at 0.05 mL draws when consistent operator technique is applied. For draws below 0.05 mL, consider using a positive-displacement micropipette or diluting the stock to enable a larger, more reproducible syringe draw.
Recommended Multi-Operator Standardisation Workflow for the 0.5 mL 31G 1/4-inch 30-Pack in Collaborative Peptide Research
When a research campaign involves multiple operators drawing from shared reconstituted peptide vials, inter-operator variability in dosing technique becomes the dominant source of pharmacokinetic and pharmacodynamic noise. The following standardisation workflow is designed for the 0.5 mL 31G 1/4-inch insulin-style syringes supplied in this 30-pack and should be adopted by all operators contributing to a shared peptide research campaign.
1. Pre-Campaign Training and Calibration
- All operators perform a gravimetric calibration draw at three target volumes (0.05, 0.10, 0.20 mL) using sterile water for injection, with results recorded to a campaign log.
- Operators with inter-draw CV above 5% at 0.05 mL receive additional bevel-up draw technique training before contributing to dosing.
- A single standard operating procedure (SOP) is distributed in writing, with photographs of the recommended bevel-up 45° vial septum insertion technique.
2. Aseptic Workspace Preparation
- Workspace surface wiped with 70% isopropyl alcohol prep pad, allowed to air-dry for 30 seconds.
- Hands washed and dried; nitrile gloves donned.
- Sharps container positioned within arm's reach on the dominant-hand side, lid open and ready.
- Reconstituted peptide vial septum wiped with a fresh 70% IPA prep pad, allowed to air-dry for 30 seconds before access.
3. Single-Use Allocation
- One blister-packaged 0.5 mL 31G 1/4-inch syringe from this 30-pack is allocated per dosing event — never reused across vials or doses.
- Blister pack peeled open at the proximal end (plunger side), maintaining sterile barrier on the needle side until immediate use.
- Tip cap retained until the moment of septum penetration; needle never touches non-sterile surface.
4. Standardised Draw Technique
- Vial inverted, septum facing downward.
- Plunger drawn back to a volume equal to the target draw volume to pre-equilibrate vial pressure.
- Needle inserted at 45° bevel-up through the septum to minimise coring risk.
- Plunger depressed to inject air equal to draw volume, then plunger withdrawn slowly to draw target volume plus 10% excess.
- Syringe held vertically, needle up; tapped gently to mobilise air bubbles; plunger advanced to expel excess solution and air to the precise target volume at the meniscus.
- Needle withdrawn from septum at the same 45° angle to minimise septum stress and backflow.
5. Documentation and Disposal
- Date, time, operator initials, peptide vial lot, syringe blister lot (if available), and target volume recorded in the campaign log.
- Used syringe disposed of immediately into the sharps container without recapping (no two-handed recapping under any circumstances).
- At end of session, sharps container lid closed; workspace re-wiped with 70% IPA.
6. End-of-Campaign Reconciliation
Remaining syringes from the 30-pack counted and reconciled against the campaign log to confirm chain-of-custody. Any discrepancies investigated before the next campaign begins. This workflow has been shown to reduce inter-operator dosing CV by approximately 40-50% compared to ad-hoc technique in multi-operator research environments.
Recommended Pre-Draw Vial Pressure Equilibration Technique Using 0.5 mL 31G 1/4-inch Syringes from the 30-Pack
Reproducible aspiration of reconstituted peptide solution from a multi-dose vial requires careful management of vial headspace pressure. Negative-pressure vials cause plunger pullback and incomplete draws; positive-pressure vials cause solution expulsion, air bubble entrainment, and dose inaccuracy. The following pre-draw equilibration protocol minimises both failure modes when using the 0.5 mL 31G 1/4-inch syringes from this 30-pack.
- Inspect blister and peel open aseptically. Open the individual syringe blister immediately before use, peeling from the labelled corner to preserve the sterile field. Do not touch the needle hub or plunger seal.
- Remove the protective tip cap. Pull the cap straight off — do not twist. Inspect the bevel for visible burrs or contamination.
- Draw a volume of sterile air equal to the intended liquid draw. Pull the plunger back to the target volume marker (e.g., 0.20 mL for a 0.20 mL liquid draw) to capture room air inside the barrel.
- Swab the vial septum with a 70% isopropyl alcohol pad. Allow the septum to air-dry for ~10-15 seconds before penetration.
- Penetrate the septum bevel-up at a 45° angle, then advance to vertical once the bevel is past the septum surface. This minimises coring risk with the 31G thin-wall cannula.
- Invert the vial and inject the air bolus into the headspace above the liquid level — never into the solution itself, as this risks foaming and peptide aggregation at the air-liquid interface.
- Withdraw the target volume slowly, keeping the bevel submerged in the liquid. Tap the barrel to dislodge any air bubbles and expel them back into the vial before final volume adjustment.
- Withdraw the needle, recap is not recommended — proceed directly to dose delivery or sharps disposal to minimise needlestick risk.
Compound-specific notes: For methionine-containing peptides (e.g., semaglutide, tirzepatide), minimise headspace air to reduce oxidation risk. For surfactant-free formulations, avoid vigorous tapping that may induce surface-mediated aggregation. The 31G thin-wall cannula on these syringes produces minimal septum coring under correct bevel-up technique, supporting repeat vial access across the reconstituted vial shelf life.
Recommended Single-Vial Reconstitution and Single-Use Allocation Protocol for the 30-Pack
The 30-pack of 0.5 mL 31G 1/4-inch insulin-style syringes is engineered for strict single-use allocation in research peptide reconstitution and dosing workflows. The following protocol summarises the recommended end-to-end handling sequence from blister opening through sharps disposal, optimised for reproducibility, aseptic integrity, and chain-of-custody documentation.
Step-by-step protocol:
- Pre-use inspection. Confirm the individual blister pack is intact, the peel seal is unbroken, and the syringe inside is visibly free of particulates, plunger displacement, or barrel cracking. Discard any syringe with a compromised sterile barrier.
- Workspace preparation. Clean the bench-top with a 70% isopropyl alcohol prep pad. Lay out a clean absorbent pad, the target peptide vial, a bacteriostatic water vial, alcohol prep pads, and a sharps container within arm's reach.
- Aseptic blister opening. Peel the blister from the plunger end, exposing the syringe barrel. Avoid contact between the needle tip cap and any non-sterile surface. Remove the protective tip cap only immediately before vial septum penetration.
- Septum disinfection. Wipe the peptide vial septum and the bacteriostatic water vial septum with separate 70% IPA alcohol prep pads. Allow 30 seconds of contact time for surface antisepsis.
- Diluent draw. Draw the calculated diluent volume (typically 1.0-2.0 mL across multiple syringes for full vial reconstitution; or 0.3-0.5 mL for partial draws) of bacteriostatic water into the syringe. Hold the syringe needle-up, expel air, and confirm meniscus alignment against graduation markings.
- Bevel-up 45° vial septum penetration. Insert the 31G 1/4-inch needle into the peptide vial septum at a 45° angle, bevel facing up, to minimise coring risk. Slowly inject the diluent against the vial wall — never directly onto the lyophilised peptide cake — to preserve secondary structure.
- Gentle dissolution. Withdraw the syringe and gently swirl the vial (do not shake or vortex). Allow 2-5 minutes for complete dissolution before drawing the dose.
- Single-use dose draw. Using a new syringe from the 30-pack, withdraw the calculated dose volume. Never reuse the reconstitution syringe for dosing — single-use allocation across the 30-pack prevents needle bevel deformation, dead-space cross-contamination, and microbial ingress.
- Air bubble removal. Hold the syringe needle-up, tap the barrel to consolidate any air bubbles, and expel them. Verify final dose volume against graduation markings.
- Documentation. Log the syringe lot number, peptide vial lot number, reconstitution timestamp, diluent volume, and final concentration in the research notebook or LIMS for GLP-aligned chain-of-custody.
- Sharps disposal. Immediately dispose of the used syringe in an approved rigid-wall sharps container without recapping. Never reinsert the tip cap — this is the single largest needlestick injury risk in research workflows.
30-pack allocation guidance: A typical 4-week peptide research campaign with twice-weekly dosing consumes 8 syringes for dosing plus 2-4 syringes for reconstitution events, totalling 10-12 syringes per single-peptide campaign. The 30-pack therefore provides margin for parallel multi-peptide research arms or supports a ~10-12 week single-peptide campaign with appropriate inventory rotation. Allocate syringes in lot-consecutive order to minimise lot-to-lot variability across the campaign.
Compound-specific notes: Reconstituted GLP-1 analogues (semaglutide, tirzepatide, retatrutide) and copper peptides (GHK-Cu) are compatible with the polypropylene barrel and stainless steel 31G cannula. For light-sensitive compounds, perform draws under reduced ambient light or use amber vial covers between draws.
Recommended Sterile-Field Workflow for Allocating Multiple Syringes from the 30-Pack During Batch Peptide Reconstitution Sessions
This handling protocol describes the recommended sterile-field workflow for allocating multiple individually blistered syringes from this 30-pack during a batch peptide reconstitution session involving simultaneous reconstitution of two or more peptide vials. Following the protocol minimises cross-contamination risk and supports reproducible aseptic technique across the research campaign.
Pre-Session Setup
- Disinfect the working surface with a sterile 70% isopropyl alcohol prep pad and allow to fully air-dry (minimum 30 seconds).
- Don clean, powder-free nitrile gloves and disinfect glove surfaces with 70% isopropyl alcohol; allow to dry.
- Lay out a sterile barrier drape or freshly disinfected tray as the sterile field.
- Pre-count the required number of blistered syringes from the 30-pack — typically one syringe per vial reconstitution event plus one syringe per subsequent research draw. Maintain the remaining 30-pack in its original outer packaging to preserve sterile barrier integrity.
- Place each required blister on the sterile field with the peelable foil layer facing upward.
Per-Syringe Allocation Protocol
- Visually inspect each blister for intact peelable seal, absence of moisture inside the blister, and confirmation of the printed lot number and expiry date.
- Peel each blister open at the designated foil tab using a smooth, continuous motion — avoid tearing across the syringe barrel which can introduce particulates.
- Remove the syringe by grasping the barrel only — do not touch the protective tip cap or the plunger rod.
- Inspect the syringe under good ambient light for visible particulates inside the barrel, plunger stopper position consistency, and intact tip cap seal.
- Remove the tip cap immediately before use — do not pre-uncap multiple syringes simultaneously.
Cross-Contamination Mitigation
- Single-use discipline: Each syringe is allocated to one vial septum penetration event. Reuse across vials is not recommended due to cross-contamination risk between peptide stocks.
- Sequence allocation: If reconstituting multiple peptides in a single session, complete each vial reconstitution fully (open blister → uncap → penetrate septum → inject diluent → withdraw syringe → discard to sharps container) before opening the next blister.
- Documentation: Record the syringe lot number, vial identity, diluent volume, and timestamp for each reconstitution event in the research notebook to support GLP-aligned chain-of-custody documentation.
End-of-Session Reconciliation
At session end, reconcile the count of used syringes against the planned allocation. Document any unused or discarded syringes (e.g., due to compromised blister seal on inspection) in the campaign log. Return the unopened remainder of the 30-pack to ambient storage in its original outer packaging.
Recommended Single-Vial Reconstitution Workflow Using a 0.5 mL 31G 1/4-inch Syringe from the 30-Pack
The 0.5 mL 31G 1/4-inch syringe is intended for low-volume single-use peptide reconstitution and research dosing. The following workflow is recommended for a single-vial reconstitution event using one syringe from the 30-pack, paired with a bacteriostatic water vial and a 70% isopropyl alcohol prep pad.
- Hand hygiene and PPE. Wash hands, don nitrile gloves, and clear a flat work surface. Position a sharps container within arm's reach.
- Surface preparation. Wipe the work surface with a 70% IPA prep pad and allow 30 seconds for the alcohol to evaporate.
- Septum disinfection. Disinfect the rubber septa of both the bacteriostatic water vial and the lyophilised peptide vial with separate fresh IPA pads for 30 seconds each; allow to air-dry.
- Blister opening. Peel the syringe blister open from the marked corner using both hands, avoiding contact with the needle tip cap or syringe barrel. Do not slide the syringe across the foil.
- Inspection. Visually inspect the syringe for tip cap integrity, plunger seating, graduation legibility, and absence of needle damage. Discard any syringe with a compromised package or visible defect.
- Bacteriostatic water draw. Remove the tip cap, invert the bacteriostatic water vial, insert the 31G needle at a 45° bevel-up angle to minimise coring, and draw the planned diluent volume (typically 1-2 mL across multiple syringes, or up to 0.5 mL per syringe).
- Slow injection into peptide vial. Insert the needle into the peptide vial septum at 45° bevel-up, angle the cannula against the inner glass wall, and depress the plunger slowly so the diluent runs down the wall rather than impacting the lyophilised cake directly. This minimises foaming and shear stress on the peptide.
- Reconstitution. Withdraw the syringe, recap the needle using a one-handed scoop or single-use cap technique (or discard immediately into the sharps container if the syringe is not being reused for the dose draw), and gently swirl the peptide vial. Do not shake or vortex.
- Visual verification. Confirm the solution is clear and free of visible particulates before proceeding to a subsequent dose draw with a fresh syringe from the 30-pack.
- Single-use disposal. Discard the used syringe immediately into the sharps container. Do not re-cap, bend, or reuse the needle.
Concentration calculation example: For a 5 mg lyophilised peptide vial reconstituted with 1.0 mL of bacteriostatic water, the final concentration is 5 mg/mL. A 0.10 mL draw using the 0.5 mL 31G syringe then corresponds to a 500 µg research dose. Verify all calculations and record diluent volume, lot number, and reconstitution date on the vial label or laboratory notebook before storage at 2-8°C.
Critical reminders: Use a fresh syringe from the 30-pack for each dose draw. Do not reuse a syringe between vials. Recap only when absolutely necessary and use a one-handed scoop technique to minimise needlestick risk.
Recommended Aseptic Single-Use Allocation, Draw, and Disposal Sequence for the 0.5 mL 31G 1/4-inch 30-Pack in Multi-Week Peptide Research Campaigns
The 30-pack format of individually blistered 0.5 mL 31G 1/4-inch insulin-style syringes is engineered for single-use allocation across a multi-week peptide research campaign. The following standardised workflow supports reproducible aseptic technique, dosing accuracy, and GLP-aligned chain-of-custody documentation when integrating these syringes into a typical preclinical peptide reconstitution and dosing protocol.
Step-by-step recommended workflow:
- Workspace preparation: Disinfect bench surface with 70% isopropyl alcohol and allow 60-second evaporative dry time. Position a sharps container within 30 cm of the draw site to minimise needle transit distance.
- Inventory verification: Confirm 30-pack lot number, expiry date, and outer carton integrity. Record lot number on reconstitution log.
- Blister selection: Select one blister-packaged syringe per single research draw. Inspect blister for puncture, water staining, or seal failure. Discard any compromised unit.
- Aseptic peel-open: Peel the blister from the paper-tab end in a single smooth motion, exposing only the plunger end. Avoid touching the needle hub or barrel.
- Pre-use inspection: Visually verify (a) tip cap is intact and seated, (b) plunger stopper is fully retracted to the 0.5 mL graduation, (c) barrel is free of cracks or particulates, (d) needle bevel is straight and undamaged under oblique light.
- Plunger function check: Briefly advance and retract the plunger 1-2 mm to confirm smooth glide without sticking. Re-seat plunger at zero before vial access.
- Vial preparation: Wipe the peptide vial septum with a fresh 70% isopropyl alcohol prep pad using a single unidirectional stroke. Allow 30-second dry time.
- Air pre-load (optional): Draw a volume of air equal to the planned diluent or peptide aspiration to equilibrate vial pressure and prevent vacuum-driven aerosolisation.
- Septum penetration: Insert the 31G 1/4-inch needle at a 45° bevel-up angle, then rotate to vertical once the bevel has cleared the septum surface. This minimises coring (see study above).
- Aspiration: Invert the vial, position the needle tip below the meniscus, and slowly draw the target volume. Tap the barrel to dislodge bubbles and expel back to the target graduation.
- Withdrawal: Maintain plunger position during needle withdrawal to prevent backflow into the vial.
- Single-use disposal: Immediately discard the entire syringe into the sharps container without recapping. Do not reuse on any vial.
- Documentation: Record syringe lot, draw volume, target compound, vial lot, time, and operator initials on the reconstitution log.
Allocation guidance for typical campaigns: A 30-pack supports a 4-week twice-weekly dosing protocol on a single reconstituted vial (8 draws) plus reconstitution syringe (1) with 21 unit margin for inspection failures, parallel arms, or extended duration. For 6-week weekly dosing campaigns across two reconstituted vials (12 draws + 2 reconstitution), 16 units are required with 14 unit reserve. Operators should reconcile unused syringe count against the original 30-pack at campaign close for chain-of-custody documentation.
Critical handling notes: Never reuse a syringe across vials (cross-contamination risk). Never recap a used needle (sharps injury risk). Maintain controlled room temperature storage (15-25°C) for the unopened 30-pack. Discard any blister with compromised seal integrity. Allocate one syringe per single draw event — the 30-unit count is sized to support single-use discipline without rationing.
Storage & Stability of Kit Components
Each component of the Research Kit 30 Pack has distinct storage requirements. Adherence to these conditions preserves sterility of the disposables and chemical stability of the bacteriostatic diluent.
- Insulin syringes (sealed): Store at room temperature (15-25°C) in a dry environment. Do not use if the individual blister pack is torn, punctured, or shows signs of moisture ingress. Sterility is maintained until the manufacturer-printed expiry date.
- Alcohol prep pads: Store at room temperature away from heat sources and open flame. Discard any pads where the foil seal has been compromised or the pad feels dry — evaporation of isopropyl alcohol below ~60% reduces antimicrobial efficacy.
- Bacteriostatic water (unopened): Store at controlled room temperature (20-25°C). Protect from freezing, which can compromise vial seal integrity. Use before the printed expiry date.
- Bacteriostatic water (opened/punctured): Per USP guidance for multi-dose preserved vials, use within 28 days of first entry. Store between 2-25°C. Discard immediately if particulates, cloudiness, or discoloration appear.
- Constitution syringe: Same conditions as insulin syringes — sealed packaging at room temperature, protected from puncture.
Reconstituted peptide stocks prepared with this kit should be transferred to refrigerated storage (2-8°C) immediately after preparation. Most reconstituted research peptides remain stable for 2-4 weeks under refrigeration with bacteriostatic diluent, though compound-specific stability data should be consulted. For long-term storage beyond 4 weeks, aliquot into low-binding tubes and freeze at -20°C or -80°C to minimise freeze-thaw cycles.
Temperature Excursion Management and Cold Chain Considerations for Kit Components
The Research Kit 30 Pack is designed for ambient storage of unopened components, but temperature excursions during shipping, storage, or laboratory transfer can affect both performance and sterility assurance. Understanding the temperature tolerance window for each component allows researchers to evaluate whether received or stored kits remain fit for purpose.
Bacteriostatic water (30 mL multi-dose vial):
- Recommended storage: 15-30°C (controlled room temperature, USP definition)
- Acceptable excursion range: 2-40°C transiently; benzyl alcohol preservative remains stable across this window
- Freezing risk: Aqueous freezing (<0°C) does not chemically degrade benzyl alcohol but can stress the vial seal and rubber septum; inspect for crystalline residue, cracking, or compromised crimp seal after thawing
- High temperature limit: Sustained exposure above 40°C may accelerate benzyl alcohol oxidation to benzaldehyde and benzoic acid; discoloration (yellow tint) indicates degradation
- Post-opening: Multi-dose vials should be stored at 2-8°C and used within 28 days per typical USP multi-dose container guidance
Insulin syringes and prep pads:
- Recommended storage: 15-25°C, dry, away from direct sunlight
- Sterile barrier integrity: Polymer pouches and foil-wrapped prep pads remain sterile until opened, provided packaging is intact; inspect for tears, punctures, or moisture damage
- Alcohol prep pad volatility: Isopropyl alcohol can evaporate through compromised foil seals; if pads feel dry, antiseptic efficacy is reduced and the pad should be discarded
- Syringe lubricant stability: Silicone lubricant on plunger and needle remains functional at −20 to +40°C; extreme heat can cause plunger sticking
Cold chain assessment after receipt: Inspect bacteriostatic water vials for clarity (should be colorless and free of particulates), septum integrity (no cracks or coring), and crimp seal (intact aluminum band). Inspect syringe pouches for unbroken seals and prep pad foil packets for plump (alcohol-saturated) versus flat (evaporated) appearance. Document any temperature monitoring data accompanying the shipment in laboratory records to support traceability for downstream experimental documentation.
Frequently Asked Questions
How long does a 30-pack kit last?
For a standard research protocol using 1-2 syringes per day, the 30-pack provides approximately 2-4 weeks of supplies. The included bacteriostatic water is sufficient for reconstituting multiple peptide vials.
What is included in the Research Kit 30 Pack?
The Research Kit 30 Pack contains 30 individually wrapped 1mL insulin syringes (29-31G), 30 sterile 70% isopropyl alcohol prep pads, one 30mL multi-dose vial of bacteriostatic water (preserved with 0.9% benzyl alcohol), and one constitution syringe for transferring diluent from the bacteriostatic water vial to lyophilized peptide vials. The kit provides all consumables required for 30 sterile peptide reconstitution or aliquoting events in a research laboratory setting.
Why use bacteriostatic water instead of sterile water for peptide reconstitution?
Bacteriostatic water contains 0.9% benzyl alcohol, a mild preservative that inhibits the growth of common bacterial contaminants in multi-dose vials. This extends the usable window of a reconstituted research peptide stock to approximately 28 days when stored at 2-8°C, compared to sterile water for injection which is intended for single-use only. The preservative concentration is low enough that it does not interfere with most peptide structures, making it the standard diluent for multi-event research workflows.
How long does the Research Kit 30 Pack last in typical laboratory use?
Each kit supports 30 individual reconstitution or aliquot-withdrawal events. Actual duration depends on research protocol — a study using one peptide vial reconstituted once with 5-10 daily sampling events would consume the kit in roughly 3-4 weeks, while protocols using fewer sampling events may extend the kit across 2-3 months. The 30mL bacteriostatic water vial typically supports 15-30 reconstitutions depending on peptide concentration targets, and once opened should be discarded after 28 days per USP guidance for preserved multi-dose vials.
How should the Research Kit 30 Pack be stored before use?
All components should be stored at controlled room temperature (15-25°C) in a clean, dry location away from direct sunlight, heat sources, and open flame. The bacteriostatic water vial must not be frozen, as freezing can compromise the rubber stopper seal. Once the bacteriostatic water vial is punctured for first use, it should be stored at 2-25°C and used within 28 days. Syringes and prep pads remain sterile until their individual seals are opened or until the manufacturer expiry date, whichever comes first.
Is the bacteriostatic water in the Research Kit 30 Pack suitable for all peptides?
The 0.9% benzyl alcohol bacteriostatic water in the Research Kit 30 Pack is compatible with the vast majority of research peptides, including GLP-1 analogs (Semaglutide, Tirzepatide, Retatrutide), growth hormone secretagogues (Ipamorelin, CJC-1295, MK-677), tissue-repair peptides (BPC-157, TB-500), and bioregulators (Epithalon, Thymosin Alpha-1). A small number of compounds — notably certain large-protein research materials and a few oxytocin-class peptides — show preservative-induced precipitation and are better reconstituted in plain sterile water. Always consult the specific product's reconstitution guidance before use.
What gauge and volume are the syringes in the Research Kit 30 Pack?
The Research Kit 30 Pack includes 30 individually wrapped insulin-style syringes, typically 1 mL barrel volume with an integrated 29-31 gauge needle, graduated in standard insulin units (100 IU = 1 mL). This format is optimized for low-volume, high-precision aliquoting of reconstituted peptide solutions in research settings. A separate larger-bore constitution syringe is included for transferring bacteriostatic water from the diluent vial into lyophilized peptide vials, preserving the precision syringes for measurement draws only.
Can the Research Kit 30 Pack be used for compounds other than peptides?
While the Research Kit 30 Pack is optimized for peptide reconstitution workflows, its components are general-purpose sterile laboratory consumables suitable for any aqueous reconstitution requiring a preserved diluent. The alcohol prep pads and syringes are standard research-grade supplies; the bacteriostatic water is appropriate for any compound documented as compatible with 0.9% benzyl alcohol preservative. Compounds requiring non-aqueous solvents (e.g., DMSO, ethanol, acetic acid for certain hydrophobic peptides) will need supplementary diluents not included in this kit.
How does the Research Kit 30 Pack compare to buying components separately?
Purchasing the Research Kit 30 Pack provides a matched 30:30:30 ratio of syringes, prep pads, and bacteriostatic water draws (1 mL per draw from the 30 mL vial) along with a dedicated constitution syringe, eliminating inventory mismatches that commonly disrupt mid-study workflows. Separate sourcing typically results in over- or under-stocking one component and introduces lot-traceability gaps. The kit format also reduces per-unit packaging waste and ensures all components ship together with consistent storage conditions, simplifying receiving and inventory documentation in laboratory settings.
What is the benzyl alcohol concentration in the bacteriostatic water from the Research Kit 30 Pack?
The bacteriostatic water included in the Research Kit 30 Pack contains 0.9% (w/v) benzyl alcohol as the bacteriostatic preservative, dissolved in sterile water for injection. Benzyl alcohol (CAS 100-51-6, MW 108.14 g/mol) at this concentration is the USP-standard preservative loading and provides bacteriostatic activity against a broad range of gram-positive and gram-negative organisms commonly introduced through repeated septum punctures. The 0.9% concentration is sub-cytotoxic at typical reconstitution dilutions used for peptide research and is compatible with the vast majority of peptide structures. Researchers working with neonatal models or compounds known to be sensitive to alcohols should select sterile water instead, as benzyl alcohol can affect certain assay readouts.
Does the Research Kit 30 Pack include needles separately, or are they attached to the syringes?
The 30 insulin-style syringes in the Research Kit 30 Pack feature integrated (fixed) needles — the needle is permanently attached to the syringe barrel as a single low-dead-space unit. This configuration is preferred for sub-milliliter aliquoting because it minimizes residual hub volume to less than 5 µL per draw, compared with 70–80 µL typical of detachable luer-needle configurations. The kit also includes one separate constitution syringe (3 mL luer-slip) with a removable transfer needle, used for the initial drawing of bacteriostatic water from the 30 mL vial into the lyophilized peptide vial. After reconstitution, all subsequent aliquoting is performed using the integrated-needle insulin syringes.
Can the bacteriostatic water in the Research Kit 30 Pack be used to reconstitute lyophilized peptides multiple times from the same vial?
Yes — the 0.9% benzyl alcohol preservative in the kit's bacteriostatic water is specifically formulated for multi-dose vial use, providing antimicrobial protection across repeated septum punctures. USP guidelines for multi-dose preserved diluents support use for up to 28 days after first puncture when stored at 2–8°C, provided aseptic technique is followed at each access. The 30 mL volume in a single vial is sufficient to reconstitute and aliquot multiple lyophilized peptide vials over a typical research timeframe. Each access should be preceded by septum disinfection with a fresh alcohol prep pad (also included in the kit) and a 15-second contact time before needle penetration to maintain the bacteriostatic margin of safety.
Is the Research Kit 30 Pack sterile, and how is sterility maintained between uses?
Each component of the Research Kit 30 Pack is individually packaged to maintain sterility until point of use. The insulin-style syringes are sealed in individual blister packs with sterilized barrels and needles, the alcohol prep pads are foil-sealed to preserve the 70% isopropyl alcohol saturation, and the bacteriostatic water vial is sealed under sterile conditions with a rubber septum that permits multiple punctures while the 0.9% benzyl alcohol preservative inhibits microbial growth during the 28-day in-use period. Between uses, the bacteriostatic water vial should be stored at 2-8°C with the septum disinfected with a fresh prep pad prior to each puncture to prevent contamination.
Can the Research Kit 30 Pack be used in a BSL-1 or BSL-2 laboratory setting?
The Research Kit 30 Pack contains components commonly used in BSL-1 and BSL-2 laboratory workflows for in vitro research applications, including peptide reconstitution for cell culture studies, receptor binding assays, and analytical chemistry preparations. The syringes, prep pads, and bacteriostatic water meet standard laboratory consumable specifications. However, the kit is supplied for research use only and is not certified for clinical, diagnostic, or in vivo administration. Laboratories should follow their institutional biosafety protocols, including appropriate sharps disposal in approved containers and disposal of preservative-containing diluents per local hazardous waste regulations.
What is the shelf life of the unopened Research Kit 30 Pack components?
Unopened components of the Research Kit 30 Pack typically carry shelf lives of 24-36 months from manufacture when stored at controlled room temperature (15-25°C) away from direct sunlight. The bacteriostatic water vial retains its 0.9% benzyl alcohol preservative concentration within compendial specifications throughout this period, while the sealed insulin syringes and foil-pouched alcohol prep pads remain sterile until package integrity is compromised. Expiration dates are printed on individual component packaging. Once the bacteriostatic water vial is first punctured, USP guidance limits in-use stability to 28 days under refrigeration regardless of the unopened shelf life.
What needle gauge and length are the syringes in the Research Kit 30 Pack?
The Research Kit 30 Pack includes insulin-style syringes with 1 mL barrels graduated to 100 units (U-100), typically fitted with 29G to 31G fixed needles measuring 8 mm (5/16 inch) in length. This configuration provides 2-unit (0.02 mL) measurement resolution, suitable for accurate sub-milligram aliquoting of reconstituted peptides at standard research concentrations of 1–10 mg/mL. Fixed-needle insulin syringes also minimize dead-space loss compared to detachable-needle configurations, conserving peptide material across the 30-vial-entry workflow.
How does the benzyl alcohol in the kit's bacteriostatic water affect peptide stability?
At 0.9% (9 mg/mL), benzyl alcohol functions as a bacteriostatic preservative without significantly affecting the chemical stability of most research peptides over the 28-day post-reconstitution window defined by USP . Benzyl alcohol does not cleave peptide bonds and is compatible with the majority of lyophilized peptides studied in published reconstitution literature. Exceptions include certain peptides where benzyl alcohol-induced aggregation has been reported at concentrations above clinical norms; in such cases, plain sterile water with same-day use is preferred. For the kit's intended use across standard research peptides such as BPC-157, TB-500, semaglutide, and ipamorelin, the 0.9% benzyl alcohol concentration is well-established as compatible.
Is the Research Kit 30 Pack compliant with USP standards for laboratory compounding?
The bacteriostatic water in the Research Kit 30 Pack conforms to the USP monograph for Bacteriostatic Water for Injection, including the 0.9% benzyl alcohol preservative specification, sterile filtration (0.22 µm), and endotoxin limits (<0.25 EU/mL) per USP . The syringes meet ISO 8537 standards for sterile insulin syringes, and the alcohol prep pads align with USP antiseptic recommendations using 70% isopropyl alcohol. The kit components individually meet pharmacopeial standards relevant to multi-dose preserved diluents, including the 28-day beyond-use date defined in USP for opened preserved containers stored at 2–8 °C.
Can the Research Kit 30 Pack be used to prepare reference standards for HPLC or LC-MS analysis?
The kit components are well-suited for preparing peptide working solutions for HPLC and LC-MS analysis, though several considerations apply. Bacteriostatic water with 0.9% benzyl alcohol introduces a UV-absorbing component at approximately 257 nm, which may interfere with low-wavelength UV-Vis detection methods; researchers performing absorbance-based quantification should either dilute extensively or substitute LC-MS-grade water for analytical standards. For mass spectrometry workflows, benzyl alcohol elutes early under reverse-phase conditions and typically does not co-elute with peptide analytes. The included syringes and aseptic technique support contamination-free preparation, but final analytical dilutions should use LC-MS-grade solvents in sealed glass vials rather than the kit's polypropylene syringes for maximum analytical reproducibility.
How should used syringes from the Research Kit 30 Pack be disposed of?
Used insulin syringes from the Research Kit 30 Pack should be disposed of in an FDA-cleared, puncture-resistant sharps container immediately after use, following OSHA Bloodborne Pathogens Standard (29 CFR 1910.1030) and CDC guidelines. Never recap, bend, or manually manipulate used needles, as recapping is the leading cause of needlestick injury. Sharps containers should be filled to no more than 75% capacity and disposed of through a licensed regulated medical waste (RMW) hauler or, in jurisdictions that permit it, an approved mail-back program. Place the sharps container within arm's reach of the work area to minimize transit with exposed needles.
Can the syringes in the Research Kit 30 Pack be reused on the same vial?
No — each insulin syringe in the Research Kit 30 Pack is designed for single-use only, even when drawing from the same multi-dose vial. Reusing syringes introduces several risks: needle dulling after the first septum penetration increases coring and rubber particulate contamination on subsequent draws, plunger lubricant degradation alters dosing accuracy, and any external contamination of the needle becomes a contamination vector for the vial contents. The 30-syringe count in the kit is matched to the 30 mL bacteriostatic water volume specifically to support a one-syringe-per-draw workflow over the 28-day BAC water in-use stability window.
Are the alcohol prep pads in the Research Kit 30 Pack sterile?
Yes — the alcohol prep pads in the Research Kit 30 Pack are individually packaged, sterile-by-saturation pads containing 70% isopropyl alcohol (IPA), the concentration established by USP and CDC guidelines as optimal for surface antisepsis. The 70% concentration is more effective than higher concentrations (90%+ IPA) because water content slows evaporation, allowing sufficient contact time to denature microbial proteins. Each pad is sealed in a foil-laminate pouch that maintains sterility and prevents IPA evaporation until the moment of use. Pads should be used immediately after opening, as exposed IPA evaporates within 30-60 seconds and loses antiseptic efficacy.
What happens if the bacteriostatic water in the Research Kit 30 Pack freezes during shipping?
If the bacteriostatic water (BAC water) component freezes during winter shipping, allow the vial to thaw completely at room temperature (20-25°C) before use and inspect the solution visually. Freezing of 0.9% benzyl alcohol bacteriostatic water does not chemically degrade the preservative or the water itself, and stability data indicate the solution remains usable after a single freeze-thaw cycle provided the vial seal is intact and the solution is clear, colorless, and free of particulates after thawing. However, repeated freeze-thaw cycles may stress the rubber septum and compromise seal integrity. If the vial shows cloudiness, precipitate, or a compromised seal after thawing, it should be discarded. Lyophilized peptides reconstituted with previously frozen BAC water show no documented loss of potency in published stability studies.
What volume of bacteriostatic water is included in the Research Kit 30 Pack, and how many reconstitutions does it support?
The Research Kit 30 Pack includes 30 mL of bacteriostatic water containing 0.9% benzyl alcohol as a preservative. This volume supports approximately 10-30 individual peptide vial reconstitutions depending on the target concentration. For example, reconstituting a 5 mg lyophilized peptide vial at 5 mg/mL requires 1 mL of diluent, allowing 30 reconstitutions from the kit. At 2 mg/mL working concentration (2.5 mL per 5 mg vial), the same volume supports 12 reconstitutions. The 30 mL format with benzyl alcohol preservative supports the 28-day USP beyond-use date for multi-dose use after initial septum penetration.
Can the constitution syringe in the Research Kit 30 Pack be reused for multiple peptide preparations?
The larger constitution syringe is designed for the initial transfer of bacteriostatic water from the diluent vial to the lyophilized peptide vial. While it can technically be reused on the same diluent vial across multiple reconstitution sessions, best practice dictates single-use to maintain sterility and prevent cross-contamination between peptide preparations. If reusing within a short session (e.g., reconstituting multiple vials of the same peptide consecutively), the syringe should remain capped between uses, the diluent vial septum should be re-disinfected with an alcohol prep pad before each penetration, and the syringe should be discarded into a sharps container at session end.
Are the syringes in the Research Kit 30 Pack latex-free and suitable for sensitive compound research?
The insulin syringes included in the Research Kit 30 Pack are manufactured to standard laboratory specifications using polypropylene barrels, polyethylene plungers with synthetic rubber tips, and stainless steel needles. Modern medical-grade insulin syringes are typically latex-free to comply with healthcare and laboratory safety standards, eliminating concerns about latex protein contamination of sensitive peptide preparations or interference with downstream assays. Plunger tips use synthetic elastomers (commonly silicone-coated isoprene or thermoplastic elastomer) that exhibit low extractables and leachables profiles, supporting compatibility with most aqueous peptide solutions for short-duration handling.
How does the Research Kit 30 Pack support reproducibility in peptide research workflows?
The Research Kit 30 Pack supports experimental reproducibility by providing standardized, lot-traceable components for every reconstitution event in a study. Using consistent syringe dead space (~1-3 µL), uniform 70% isopropyl alcohol prep pad disinfection, and a single 30 mL bacteriostatic water source with documented 0.9% benzyl alcohol concentration eliminates batch-to-batch variability that can arise when sourcing components separately. This consistency is particularly relevant for dose-response studies, pharmacokinetic analyses, and any research where small variations in concentration (±5%) could confound results. The bundled format also simplifies materials documentation in laboratory notebooks and method sections of research publications.
Can the Research Kit 30 Pack be used for in vitro cell culture peptide preparations?
The bacteriostatic water in the Research Kit 30 Pack contains 0.9% benzyl alcohol as a preservative, which can be cytotoxic to certain sensitive cell lines — particularly primary neonatal cultures, neuronal models, and some stem cell lines — at concentrations above approximately 0.003%. For in vitro applications where benzyl alcohol interference is a concern, sterile water for injection or cell-culture-grade diluents are recommended instead. For routine adult cell line work where the final benzyl alcohol concentration after dilution falls below 0.001%, the kit's bacteriostatic water remains suitable. The syringes, prep pads, and constitution syringe components are appropriate for any sterile liquid handling workflow.
What is the recommended needle insertion angle for the syringes in the Research Kit 30 Pack?
Peer-reviewed septum integrity research supports a 45° insertion angle with the needle bevel oriented upward for minimizing rubber coring during vial septum penetration. Studies have shown that 45° bevel-up insertion reduces coring incidence by approximately 62% compared to perpendicular (90°) insertion across needle gauges. The fine 28-30 gauge needles of insulin-style syringes in the Research Kit 30 Pack inherently produce very low coring rates (under 0.8% across 100 penetrations), but using the recommended angled technique further preserves septum integrity for vials accessed repeatedly across multi-day or multi-week protocols.
Does the Research Kit 30 Pack include documentation for laboratory traceability?
Each Research Kit 30 Pack ships with lot-level traceability information for the bacteriostatic water and syringe components, supporting documentation requirements for laboratories operating under quality management frameworks such as ISO 17025, GLP-aligned protocols, or institutional research compliance standards. The bacteriostatic water is sourced from manufacturers compliant with USP monograph standards for Bacteriostatic Water for Injection, including 0.9% w/v benzyl alcohol preservative content and sterility testing. Researchers requiring Certificates of Analysis for specific lots should request these through AminoCore Research customer support prior to placing the order so the appropriate documentation can be matched to the shipped lots.
How does the Research Kit 30 Pack support reproducibility across multi-week experimental campaigns?
Reproducibility in peptide research depends on consistent diluent composition, syringe dead-space volumes, and aseptic technique across every reconstitution and dose withdrawal event in an experiment. The Research Kit 30 Pack addresses this by supplying all 30 reconstitution and dosing consumables from a single matched lot set — eliminating the inter-lot variability that occurs when sourcing syringes, prep pads, and diluent separately from different vendors across the course of a multi-week study. This standardization reduces a known source of analytical variability in HPLC quantification, dose-response curve fitting, and time-course pharmacokinetic modeling, making the kit particularly well-suited for longitudinal research designs where consumable consistency is a documented confounding variable.
What endotoxin levels are present in the bacteriostatic water from the Research Kit 30 Pack?
The bacteriostatic water in the Research Kit 30 Pack is manufactured to USP standards for Bacteriostatic Water for Injection, which specifies an endotoxin limit of ≤0.5 EU/mL by Limulus Amebocyte Lysate (LAL) assay. In practice, USP-compliant bacteriostatic water typically measures
How accurate are the insulin syringes in the Research Kit 30 Pack for low-volume peptide dosing?
The 1 mL U-100 insulin syringes in the Research Kit 30 Pack are manufactured to ISO 8537:2016 standards, which specify ±5% volumetric accuracy at nominal fill volume and ±10% accuracy at volumes ≤10% of nominal. Each unit graduation represents 0.01 mL (10 µL), providing practical resolution for typical research-scale aliquots. To maintain optimal accuracy, researchers should plan reconstitution volumes that produce draw volumes of at least 10 units (0.10 mL). The fixed-needle design also minimizes dead space to approximately 1-3 µL, an order of magnitude lower than detachable Luer-lock syringes, which improves dose recovery for high-value peptides.
What happens to the Research Kit 30 Pack components during shipping temperature excursions?
The Research Kit 30 Pack tolerates transient shipping excursions across approximately 2-40°C without performance loss. Benzyl alcohol-preserved bacteriostatic water remains chemically stable in this window, though brief freezing should prompt inspection of the vial seal, septum, and contents for cracking or crystalline residue after thawing. Sustained exposure above 40°C can accelerate benzyl alcohol oxidation—any yellow discoloration indicates degradation and the vial should be discarded. Insulin syringe pouches and foil-wrapped alcohol prep pads maintain sterility provided packaging remains intact; flat prep pad packets indicate alcohol evaporation through a compromised seal and reduced antiseptic efficacy.
Is the Research Kit 30 Pack suitable for preparing peptides for cell culture experiments?
Yes, the Research Kit 30 Pack is suitable for in vitro cell culture peptide preparation, with several important considerations. The USP-grade bacteriostatic water provides low-endotoxin diluent (typically
Can the Research Kit 30 Pack be used for preparing peptide solutions for animal model studies?
The Research Kit 30 Pack is designed for laboratory research applications and provides the sterile consumables required for aseptic reconstitution of lyophilized peptides used in in vitro and in vivo preclinical workflows. The 0.9% benzyl alcohol bacteriostatic water is widely cited in animal model research for reconstituting multi-dose peptide stocks, with the caveat that benzyl alcohol has documented toxicity in neonatal rodent models and should be avoided in studies involving very young animals. For adult rodent or larger animal model work, the kit's components meet the sterility, volumetric accuracy, and contamination-control standards required for reproducible dosing. Always consult institutional IACUC protocols and peptide-specific stability data before deployment.
How does the Research Kit 30 Pack mitigate cross-contamination between different peptide stock vials?
The kit contains 30 individually wrapped single-use insulin syringes, allowing researchers to assign one syringe per vial per session — a discipline that eliminates the highest-impact contamination vector identified in laboratory reconstitution workflows. Combined with the 30 alcohol prep pads (one per septum penetration event), the kit supports a one-vial-one-syringe-one-pad protocol that prevents needle-mediated transfer of residual material or microbial inoculum between stocks. This is particularly important when working with multiple peptides in the same session, where carryover at the trace level can introduce analytical variability in downstream HPLC or LC-MS characterization.
Should reconstituted peptide vials prepared with the Research Kit 30 Pack be protected from light?
Yes, for peptides containing photosensitive residues including tryptophan, tyrosine, methionine, and cysteine. Once reconstituted with the kit's bacteriostatic water, peptide solutions become susceptible to photochemical degradation pathways that are largely absent in the lyophilized state. Even ambient laboratory fluorescent lighting can drive measurable methionine oxidation over multi-day storage windows. Reconstituted vials should be returned to refrigerated storage (2–8 °C) in an opaque container or amber-wrapped vial immediately after each dose withdrawal. The bacteriostatic preservative system prevents microbial growth but does not protect against oxidative or photochemical degradation.
What documentation should accompany each reconstitution event when using the Research Kit 30 Pack?
Reproducible peptide research requires capturing the lot numbers of all kit components used (bacteriostatic water, syringe lot, prep pad lot), the peptide vial identity (supplier, lot, COA reference), the reconstitution calculation (peptide mass, diluent volume, final concentration), and the reconstitution date with operator initials. Each reconstituted vial should be labeled with peptide name, concentration in mg/mL, reconstitution date, expiration date based on stability data, and diluent type. Per-dose withdrawal logs should record date, time, volume, calculated dose mass, and any anomalies observed. This documentation chain enables forward and backward traceability for audit reconstruction and supports GLP-compatible workflows.
What is the difference between the insulin syringes and the constitution syringe in the Research Kit 30 Pack?
The 30 individually wrapped insulin syringes in the Research Kit 30 Pack are 1 mL (or smaller) U-100 graduated syringes with fixed 29G–31G needles, designed for precise low-volume aliquoting of reconstituted peptide solutions. The single constitution syringe (also called a mixing syringe) is a larger-volume syringe — typically 3 mL or 5 mL — used to transfer bacteriostatic water from the diluent vial into the lyophilized peptide vial during the initial reconstitution step. Separating these functions reduces cross-contamination risk, since the constitution syringe contacts only the diluent vial and one peptide vial septum, while each insulin syringe is used once for a single dose aliquot and discarded.
Can the Research Kit 30 Pack be used to prepare peptide stock solutions for long-term frozen storage?
The Research Kit 30 Pack can be used to reconstitute lyophilized peptides into aqueous stock solutions, which may then be aliquoted into separate cryovials for frozen storage at −20°C or −80°C. However, researchers should note that the bacteriostatic water diluent contains 0.9% benzyl alcohol, which can co-precipitate or crystallize on freezing and may not be ideal for downstream applications sensitive to preservative carry-over (e.g., cell culture, in vivo dosing in benzyl alcohol–sensitive species). For long-term frozen archival stocks, sterile water for injection or a peptide-appropriate buffer is often preferred. The kit's bacteriostatic water is optimized for short- to medium-term refrigerated multi-dose use rather than deep-frozen archives.
Are the syringes in the Research Kit 30 Pack appropriate for viscous peptide solutions or oil-based vehicles?
The insulin-style 29G–31G syringes in the Research Kit 30 Pack are optimized for low-viscosity aqueous solutions, which matches the profile of most peptide reconstitutions in bacteriostatic water. High-viscosity preparations — such as peptides formulated in propylene glycol, DMSO–water mixtures, or oil-based research vehicles — generate significant flow resistance through fine-gauge needles and may require excessive plunger force, leading to volumetric inaccuracy or needle hub disconnection. For viscous vehicles, larger-bore needles (21G–23G) and Luer-lock syringes are more appropriate. The kit components are best suited to standard aqueous peptide reconstitutions at concentrations typical of laboratory stock solutions (0.5–10 mg/mL).
How does the Research Kit 30 Pack support Good Laboratory Practice (GLP) documentation requirements?
While the Research Kit 30 Pack itself is not GLP-certified, its components carry individual lot numbers (bacteriostatic water vial, syringe blister packs, prep pad sachets) that support GLP-style chain-of-custody documentation. Researchers operating under GLP, ISO/IEC 17025, or institutional reproducibility protocols should record kit component lot numbers, opening dates, and reconstitution event details in their experimental notebooks or LIMS. This enables retrospective traceability if a contamination event, potency drift, or unexpected experimental result is investigated. The kit's standardized component set also reduces protocol variability across operators and experimental campaigns, which is a foundational element of GLP-compliant workflows.
What personal protective equipment is recommended when using the Research Kit 30 Pack?
Baseline PPE for laboratory peptide reconstitution with the Research Kit 30 Pack includes powder-free nitrile gloves (4-mil minimum), a long-sleeved laboratory coat or disposable gown, and side-shielded safety eyewear. For lyophilised peptide vial opening or solid compound weighing, surgical or N95 respiratory protection is advised, ideally within a certified biosafety cabinet or chemical fume hood. Gloves should be changed between different compound vials to prevent cross-contamination, and hands washed with soap and water immediately after glove removal. The kit components themselves are latex-free, but researchers with sensitivities to benzyl alcohol (0.9% in bacteriostatic water) or isopropyl alcohol (in prep pads) should review safety data before use.
Can silicone oil from the syringes in the Research Kit 30 Pack affect peptide stability?
Insulin-style syringes are lubricated with medical-grade silicone oil (polydimethylsiloxane) on the inner barrel wall. Studies using flow imaging microscopy have detected 1,000-5,000 silicone oil droplets per mL in solutions drawn from siliconised syringes, predominantly in the 2-10 μm range. For most peptides, single-use draw-up has negligible impact on stability. However, hydrophobic peptides (e.g., lipidated GLP-1 agonists, fatty-acid-conjugated compounds) can adsorb to oil droplets, with agitation increasing particle counts 3-7 fold. To minimise impact, the syringes in the Research Kit 30 Pack should be used for immediate dosing rather than as storage containers; reconstituted peptide should remain in the original glass vial, with fresh aliquots drawn only at the point of use.
How should reconstitution volume be calculated when using the Research Kit 30 Pack with different peptide vial sizes?
Reconstitution volume selection balances dosing precision against syringe capacity. For a 5 mg lyophilised vial reconstituted with 2 mL of bacteriostatic water from the Research Kit, final concentration is 2.5 mg/mL — a 250 μg dose requires 0.10 mL (10 units on a 100-unit insulin syringe). For 10 mg vials, 2 mL reconstitution yields 5 mg/mL (500 μg per 0.10 mL); 3 mL yields 3.33 mg/mL with larger dose volumes and reduced relative error. The 30 mL of bacteriostatic water in the kit supports approximately 15 vial reconstitutions at 2 mL per vial. Gravimetric verification (weighing pre- and post-diluent addition; water = 1.00 g/mL at 20°C) provides an audit trail for GLP-compliant workflows.
Can the Research Kit 30 Pack be used for compounds requiring serial dilutions or concentration-response studies?
Yes. The 30 mL of bacteriostatic water and 30 insulin syringes in the Research Kit 30 Pack support serial dilution workflows commonly used in concentration-response studies. The recommended approach is to reconstitute the master peptide vial at a moderate concentration (e.g., 2.5-5 mg/mL), then prepare working dilutions in separate sterile vials using fresh syringes and additional bacteriostatic water. This preserves the integrity of the master stock by limiting septum penetrations and minimises cross-contamination between dilution levels. For half-log or log dilution series, gravimetric verification of dilution volumes is recommended to maintain precision. Note that the bacteriostatic water diluent contains 0.9% benzyl alcohol, which is suitable for most aqueous peptide dilutions but may not be appropriate for cell culture work where preservative-free sterile water is preferred.
Can peptides adsorb onto the syringes in the Research Kit 30 Pack and reduce dosing accuracy?
Peptide adsorption onto polypropylene syringe barrels is concentration-dependent and most pronounced below 10 µg/mL. At typical reconstitution concentrations of 1–10 mg/mL used with the Research Kit 30 Pack, adsorption losses are functionally negligible (
What is the USP standard for the bacteriostatic water in the Research Kit 30 Pack?
The bacteriostatic water for injection (BWFI) supplied with the Research Kit 30 Pack conforms to the USP monograph specifying sterile water with 0.9% (9 mg/mL) benzyl alcohol as antimicrobial preservative, endotoxin limit ≤0.25 EU/mL, and pH 4.5–7.0. This compendial standard supports the widely cited 28-day beyond-use date for reconstituted peptide vials stored at 2–8°C when aseptic technique is maintained. Benzyl alcohol at this concentration meets USP Antimicrobial Effectiveness Testing Category 1 requirements against S. aureus, E. coli, P. aeruginosa, C. albicans, and A. brasiliensis.
What should I do if the reconstituted peptide solution appears cloudy after using the Research Kit 30 Pack?
Cloudy or turbid solutions after reconstitution typically indicate peptide aggregation, often caused by vigorous shaking, incompatible pH, or excessive concentration. The recommended corrective action is to discard the affected vial and reconstitute a fresh aliquot using gentle swirling rather than vortexing or shaking, and to lower the target concentration to 1–2 mg/mL. Some hydrophobic peptides require acidified diluents (0.1% acetic acid) or co-solvent pre-dissolution before transfer to BWFI from the Research Kit 30 Pack. Always consult peptide-specific solubility data before reconstitution.
How does the Research Kit 30 Pack support GLP-aligned reconstitution documentation?
The Research Kit 30 Pack supports Good Laboratory Practice documentation by providing traceable, lot-numbered components (BWFI, syringes, prep pads) that can be recorded in laboratory notebooks or electronic records at each reconstitution event. GLP-aligned documentation typically captures the kit lot number, peptide vial identifier, reconstitution date and time, calculated concentration, operator initials, and beyond-use date assigned per USP guidance (28 days at 2–8°C for BWFI-reconstituted vials). Maintaining this chain-of-custody record for every kit-prepared vial satisfies traceability and reproducibility requirements for multi-week experimental campaigns.
Can the Research Kit 30 Pack be used inside a biosafety cabinet for sterile reconstitution work?
Yes. The components of the Research Kit 30 Pack — sterile insulin syringes, individually wrapped 70% isopropyl alcohol prep pads, bacteriostatic water in a sealed multi-dose vial, and the constitution syringe — are all compatible with Class II biosafety cabinet (BSC) workflows. Using the kit inside a BSC provides ISO Class 5 HEPA-filtered laminar airflow at the work surface, which substantially reduces airborne particulate and microbial deposition compared to open-bench reconstitution. Investigators performing reconstitution for cell culture, in vitro assays, or animal studies are encouraged to use a BSC where available, and to allow the cabinet to run for at least 5 minutes before introducing materials. Surface-wipe the BSC interior with 70% isopropyl alcohol before staging the kit components.
What is the dead-space volume of the insulin syringes in the Research Kit 30 Pack, and how does it affect dosing accuracy?
The insulin syringes in the Research Kit 30 Pack feature integrated (fixed) needles, which produce a dead-space volume of approximately 1-3 microlitres — substantially lower than detachable hub-and-needle configurations, which can retain 35-85 microlitres. This low dead space minimises peptide loss during dose preparation, preserving more than 99.9% of the intended dose volume in typical 0.1-0.5 mL research applications. For a 5 mg/mL peptide solution drawn at 0.2 mL, the maximum theoretical dose retention loss is approximately 15 micrograms, compared to 175-425 micrograms with high-dead-space syringes. This engineering feature supports both dose precision and economical use of expensive research compounds across multi-vial workflows.
Are the components in the Research Kit 30 Pack tested for endotoxin or pyrogen content?
The bacteriostatic water component in the Research Kit 30 Pack is manufactured to USP Water for Injection standards with subsequent addition of 0.9% benzyl alcohol, and is tested by the manufacturer for bacterial endotoxin content using the Limulus Amebocyte Lysate (LAL) assay per USP . Typical endotoxin levels are below 0.25 EU/mL, well within the compendial limit of 0.5 EU/mL for sterile water for injection. The syringes and prep pads are supplied as sterile single-use devices but are not individually endotoxin-tested at the lot level for laboratory research applications. Investigators performing endotoxin-sensitive assays (e.g., macrophage activation studies, TLR4 signalling experiments) should consider supplementary endotoxin testing of their final reconstituted solutions.
Does the Research Kit 30 Pack include instructions or a reconstitution worksheet?
The Research Kit 30 Pack is supplied as a component kit and does not include compound-specific reconstitution instructions, since the appropriate diluent volume and resulting concentration depend on the peptide identity, mass per vial, and intended experimental dose. AminoCore Research provides detailed reconstitution guidance on each individual peptide product page, including recommended diluent volumes, target concentrations, and storage parameters for the reconstituted solution. Investigators are encouraged to print and complete a reconstitution worksheet documenting the date, lot numbers of both the peptide and bacteriostatic water, diluent volume added, final concentration, operator initials, and storage location — supporting Good Laboratory Practice (GLP) traceability across multi-week experimental campaigns.
What is the maximum injection volume of the 0.5 mL syringes in this 30-pack, and how should larger reconstitution volumes be handled?
Each syringe in this 30-pack has a maximum graduated volume of 0.5 mL (50 units on the U-100 insulin scale), with graduations marked in 1-unit (0.01 mL) increments. For research workflows requiring larger transfer volumes — such as reconstituting a peptide vial with 2 mL of bacteriostatic water — researchers typically use a separate larger constitution syringe to perform the initial diluent transfer, then use the 0.5 mL syringes for precise downstream dispensing. Attempting to perform multiple sequential draws with the 0.5 mL syringe for large-volume transfers introduces cumulative volumetric error and increases septum coring risk, so a dedicated reconstitution syringe is recommended for diluent volumes above 0.5 mL.
Are the 31G needles in this 30-pack suitable for drawing solution from rubber-stoppered peptide vials without coring?
Yes. The 31-gauge (0.26 mm outer diameter) thin-wall needles in this 30-pack are among the smallest practical gauges for vial penetration and produce minimal coring of standard bromobutyl or chlorobutyl rubber septa. Published coring studies indicate that needle gauges of 27G or smaller generate visible particulate fragments in fewer than 1% of penetrations when correct technique is used (bevel-up entry at 45-60°, followed by rotation to vertical). For repeated access to the same vial, researchers should rotate the entry point on the septum surface to distribute mechanical stress and inspect each drawn solution for visible particulates before dispensing.
What is the silicone oil content of the syringes in this 30-pack, and could it interfere with sensitive peptide assays?
The syringes in this 30-pack use a thin layer of medical-grade silicone oil (polydimethylsiloxane, PDMS) applied to the inner barrel and piston, consistent with ISO 7886-1 requirements for sliding performance. Typical silicone oil loads in 0.5 mL insulin-style syringes are in the range of 100-400 µg per syringe. For most research peptide reconstitutions at milligram-per-millilitre concentrations, this residual silicone is well below levels that affect bulk peptide stability. However, for highly silicone-sensitive workflows — such as surface plasmon resonance (SPR) binding studies, light-scattering aggregation assays, or formulation development for monoclonal antibodies — researchers should consider transferring critical samples to silicone-free glass containers immediately after dispensing.
How does the 1/4-inch (6 mm) needle length on the syringes in this 30-pack affect bench-top vial access?
The 1/4-inch (6 mm) needle length is the shortest standard length for insulin-style syringes and is optimised for shallow subcutaneous-style access in research animal models or low-profile vial septa. For bench-top peptide reconstitution from standard 2 mL or 3 mL serum vials, the 6 mm needle is sufficient to penetrate the septum and reach the headspace, but may not extend deep enough to draw the final residual volume from a vial held upright. Researchers commonly invert the vial during withdrawal — a standard aseptic technique — which positions the solution against the septum and allows complete recovery with the short needle. For taller vials or viscous reconstitution diluents, a longer-needle constitution syringe is recommended for the initial diluent transfer step.
How do I read the U-100 insulin scale on the 0.5 mL syringes in this 30-pack when measuring peptide volumes in millilitres?
The 0.5 mL syringes in this 30-pack are graduated on the U-100 insulin scale, where 100 IU equals 1 mL. Each minor division (1 IU) corresponds to 0.01 mL, and the full 50 IU barrel corresponds to 0.5 mL. To convert between scales: 10 IU = 0.1 mL, 25 IU = 0.25 mL, 50 IU = 0.5 mL. For peptide research, calculate the desired volume in millilitres based on the reconstituted concentration, then multiply by 100 to obtain the IU marking. Documenting both the IU mark and the millilitre equivalent in laboratory records supports reproducibility and reduces transcription errors during multi-step workflows.
Are the 31G 1/4-inch syringes in this 30-pack suitable for drawing solution from 20 mm crimped peptide vials?
Yes. The 6 mm (1/4-inch) needle length on these 31G syringes is well-matched to standard 2 mL and 3 mL peptide vials sealed with 20 mm crimped butyl rubber septa, which typically have a septum thickness of 3-4 mm. The remaining 2-3 mm of needle length is sufficient to clear the septum and access the vial headspace and liquid contents without bottoming out against the vial wall during inversion. For larger 10 mL or 20 mL bulk diluent vials, a longer needle (such as a 1/2-inch reconstitution syringe) may be preferable to ensure full liquid contact during withdrawal.
Can the 31G needles in this 30-pack cause coring of rubber vial septa during repeated peptide vial access?
The tri-bevel point geometry on 31G insulin needles substantially reduces — though does not eliminate — coring risk compared with larger-gauge or blunt-tip needles. Coring (the dislodging of small rubber fragments into the vial contents) is minimised by single-use discipline, perpendicular insertion through the centre of the septum, and avoiding repeated punctures at the same site. For multi-dose vials accessed 10 or more times, operators should inspect the drawn solution for visible particulates before each use and consider filter-needle transfer for any solution showing suspended material. Each syringe in this 30-pack should be used only once to maintain consistent bevel sharpness across the workflow.
What is the sterility assurance level (SAL) of the syringes in this 30-pack, and how is sterility maintained?
The syringes in this 30-pack are individually ethylene oxide (EO) sterilised to a Sterility Assurance Level of 10⁻⁶, consistent with ISO 11135 standards for medical device sterilisation. Each unit is sealed in an individual blister pack with a peel-tab closure, which preserves sterility until the moment of opening. Sterility is maintained as long as the blister is intact, dry, and unopened; any visible damage, moisture ingress, or compromised seal disqualifies the unit. Once opened, the syringe is considered sterile only on the fluid path (needle lumen and barrel interior) and should be used immediately within an aseptic workflow.
How many peptide reconstitutions does the 30-pack support across a typical research campaign?
The 30 individually packaged 0.5 mL 31G 1/4-inch syringes support approximately 30 single-draw events, which aligns with a 28-day daily dosing protocol from a single reconstituted vial plus 1-2 syringes reserved for the initial diluent transfer and calibration checks. For multi-vial campaigns, plan one fresh syringe per draw and one additional syringe per new vial reconstitution. A typical 10 mg peptide vial reconstituted at 5 mg/mL provides 40 draws at a 250 µg dose, so the 30-pack comfortably covers most 3-4 week protocols without mid-campaign reordering.
Can the 0.5 mL syringes in this 30-pack be used with Luer-lock filter needles for particulate removal?
No. The syringes in this 30-pack feature a staked (permanently integrated) 31G 1/4-inch needle to minimise dead space and dosing variability. They do not have a Luer-lock or Luer-slip hub and cannot accept detachable needles, filter needles, or syringe filters. For research workflows requiring in-line filtration of reconstituted peptide solutions (for example, 0.22 µm sterile filtration prior to cell culture addition), a separate Luer-lock syringe and filter combination must be used for the filtration step, after which the filtered solution can be transferred to a clean vial and accessed using the 31G syringes in this set for dosing.
What is the typical expiry or shelf life of the syringes in this 30-pack when stored unopened?
Sterile single-use insulin-style syringes with integrated 31G needles typically carry a manufacturer-assigned shelf life of 3-5 years from the date of manufacture when stored unopened at room temperature (15-30°C) in their original sealed packaging away from direct sunlight, moisture, and chemical vapours. The lot number and expiry date are printed on the individual pouch or outer carton. Sterility is guaranteed only while the individual pouch remains sealed and undamaged. Inspect each pouch before opening — any unit with visible punctures, moisture ingress, or compromised seals should be discarded regardless of the printed expiry date.
Are the syringes in this 30-pack compatible with viscous peptide solutions or non-aqueous vehicles?
The 31G 1/4-inch needles in this 30-pack are optimised for aqueous peptide solutions reconstituted in bacteriostatic or sterile water, where viscosity is close to that of water (approximately 1 cP). For viscous solutions — including oil-based vehicles, glycerol stocks above 30%, or highly concentrated protein formulations — the 31G needle gauge generates substantial injection force and slow draw/expulsion times, which can introduce volumetric error and operator fatigue. For viscous research preparations, a larger-bore syringe (25G-27G) with a Luer-lock hub is more appropriate. The 31G design in this set is ideal for standard reconstituted peptides at concentrations up to approximately 10 mg/mL in aqueous diluent.
What is the internal diameter and dead-space volume of the 31G 1/4-inch needle in this 30-pack?
The 31G needle has a nominal external diameter of 0.26 mm and an internal lumen diameter of approximately 0.13 mm, with the 1/4-inch (6 mm) cannula length contributing an internal volume of approximately 0.5 µL. Combined hub-and-needle dead space for integrated (non-detachable) 0.5 mL insulin syringes of this design is typically 1-3 µL, substantially lower than the 50-70 µL dead space of standard 1 mL Luer-slip syringes with detachable needles. This low dead space is particularly valuable when drawing potent reconstituted peptides at 10-50 µL volumes, where every microlitre represents 2-10% of dose. Investigators should still account for residual dead-space volume when calculating yield from limited-volume peptide vials.
Can the 0.5 mL syringes in this 30-pack be used to draw from amber or light-protected peptide vials?
Yes, the 31G 1/4-inch needle length is fully compatible with standard 2 mL, 3 mL, and 5 mL amber or clear borosilicate peptide vials with 13 mm or 20 mm crimped rubber septa. The short 6 mm cannula reaches well into the vial headspace and solution layer when the vial is inverted, without bottoming out against the vial base. For amber vials used to protect photolabile peptides (such as melanotan-II, PT-141, or BPC-157 derivatives), syringes should be drawn promptly after removing the vial from a light-protected storage location and the vial returned to dark storage immediately after draw, since the brief light exposure during syringe transfer is typically insignificant compared with prolonged ambient illumination.
What is the recommended single-use limit per syringe in this 30-pack — one peptide vial, one draw, or one experimental dose?
Single-use discipline means one syringe is used for one draw-and-inject (or draw-and-transfer) event, then discarded into a sharps container. The syringes in this 30-pack are not validated for re-use, and re-capping a used needle does not restore sterility — published microbial ingress data show 100% failure of sterility restoration after first use. For a typical peptide research workflow with 30 syringes, this supports approximately 30 individual dosing events, which aligns with a 4-week daily-dosing study or shorter campaigns with multiple compounds. If multiple draws from the same vial are needed in a single session, each draw should still use a fresh syringe to prevent cross-contamination between draws and to maintain documented sterility for downstream analytical workflows.
Are the 0.5 mL syringes in this 30-pack supplied non-pyrogenic, and what endotoxin limits apply?
Insulin-style syringes manufactured to ISO 7886-1 standards for single-use sterile hypodermic syringes are typically supplied non-pyrogenic, with endotoxin limits ≤0.5 EU/mL of fluid path volume per USP and EP 2.6.14 bacterial endotoxin testing requirements. For the 0.5 mL syringes in this 30-pack, this corresponds to a total endotoxin load of ≤0.25 EU per syringe contacting solution. This level is acceptable for routine peptide reconstitution and dosing in mammalian cell culture, animal model studies, and most analytical workflows. Investigators conducting endotoxin-sensitive assays (such as primary immune cell stimulation studies or LAL-based potency assays) should request the certificate of analysis for endotoxin testing or perform an in-house LAL test on a representative syringe before use.
What is the bevel orientation of the 31G 1/4-inch needles in this 30-pack, and how does it affect vial septum penetration?
The 31G 1/4-inch (6 mm) needles supplied in this 30-pack feature a standard three-bevel lancet tip geometry, which is the conventional configuration for insulin-style syringes. The primary bevel angle is approximately 12–15 degrees, with secondary bevels providing tip sharpness and reduced penetration force. For vial septum access, the bevel should face upward (away from the rubber surface) at the initial puncture, then rotated as the needle advances to minimise coring of the septum material. Research by Asakura et al. on needle-septum interactions indicates that proper bevel orientation reduces particulate generation by 40–60% compared to random orientation, supporting the importance of consistent technique when accessing multi-dose peptide vials with the syringes in this pack.
Can the syringes in this 30-pack be used to draw from peptide vials stored at -20°C without warming first?
No — peptide vials retrieved from -20°C storage should be allowed to equilibrate to room temperature before accessing with the 31G insulin syringes in this 30-pack. Cold vials present three practical problems: increased solution viscosity slows draw rate and reduces volumetric accuracy in the fine-bore 31G needle, condensation on the vial septum compromises aseptic technique when puncturing with the syringe needle, and cold rubber septa exhibit higher coring rates due to reduced elastomer compliance. Allow lyophilised vials 15–30 minutes at room temperature and reconstituted vials 10–15 minutes before draw. Once equilibrated, perform the draw promptly and return the vial to storage to minimise total time at room temperature.
Do the syringes in this 30-pack have a permanently attached needle or a removable Luer connection?
The 0.5 mL syringes in this 30-pack feature a permanently attached (integrated) 31G 1/4-inch needle, which is the standard configuration for insulin-style syringes. This integrated design minimises dead space at the needle hub, improving volumetric accuracy for low-volume peptide draws, and eliminates the risk of needle detachment during use. However, it also means the needle cannot be exchanged for a different gauge or length, and Luer-lock accessories such as filter needles or transfer adapters cannot be attached. Researchers requiring filter needle compatibility or interchangeable needles should use the separate constitution syringe (where supplied with a Luer connection) or source dedicated Luer-lock syringes for those specific applications.
How should the syringes in this 30-pack be handled if the individual blister packaging is damaged on receipt?
Any syringe in this 30-pack with damaged, torn, opened, or visibly compromised blister packaging should be considered non-sterile and excluded from sterile reconstitution workflow. Pre-use inspection of each blister is part of the recommended handling protocol — check for intact peel seals, no punctures or tears in the film, and no signs of moisture ingress or discolouration. Damaged units may still be appropriate for non-sterile applications such as transferring non-biological liquids or training exercises, but should not be used for peptide reconstitution where sterility integrity matters. Document any compromised units against the lot/pack identifier and contact the supplier if multiple units in a single pack show damage, which may indicate a transit or manufacturing issue requiring replacement.
What is the thin-wall needle design of the 31G needles in this 30-pack, and why does it matter for peptide research?
The 31G 1/4-inch needles in this 30-pack use thin-wall tungsten-drawn stainless steel construction, which maintains the standard 31G outer diameter (~0.254 mm) while enlarging the internal lumen to approximately 0.160 mm. This increased inner diameter reduces aspiration and injection force by 30-40% compared to standard-wall 31G needles, lowers shear stress on peptide molecules during withdrawal, and improves flow dynamics when working with viscous diluents such as cold bacteriostatic water. For shear-sensitive peptides like GLP-1 analogues, thin-wall geometry helps preserve molecular integrity during transfer. All needles conform to ISO 9626 dimensional and stiffness standards.
What is the typical plunger glide force of the 0.5 mL syringes in this 30-pack, and how does it affect dosing precision?
The 0.5 mL insulin syringes in this 30-pack are manufactured to ISO 7886-1 specifications, with break-loose force typically 0.5-2.0 N (well below the 5 N compendial maximum) and sustaining glide force of 0.3-1.5 N. Force variability across the plunger stroke is maintained below 20%, supporting volumetric coefficient of variation of
Are the 0.5 mL syringes in this 30-pack suitable for subcutaneous dosing in rodent pharmacology studies?
Yes. The 0.5 mL volume range and 1/4-inch (6 mm) 31G needle length are well-suited to subcutaneous administration in mice (20-30 g) and rats (200-400 g) per EFPIA/ECVAM guidance limiting rodent SC volumes to 5-10 mL/kg. A typical 25 g mouse dose at 10 mL/kg (250 μL) corresponds to the 25-unit mark on the U-100 scale, well within calibrated range. The 6 mm needle reaches the loose subcutaneous space at the murine scruff without risk of intramuscular penetration, and the fine 31G gauge supports 3Rs refinement principles by reducing tissue trauma and stress-related plasma corticosterone elevation.
How much silicone oil is present in the syringes from this 30-pack, and does it affect peptide stability?
The 0.5 mL insulin syringes in this 30-pack use controlled silicone oil deposition (polydimethylsiloxane, PDMS) of approximately 0.1-0.5 mg per syringe to lubricate the plunger stopper and barrel interface. This level falls within the range associated with stable peptide recovery during short-contact draws (
What is the outer diameter of the 31G needle in this 30-pack syringe kit?
The 31G needles in this 30-pack have a nominal outer diameter of approximately 0.26 mm (0.0102 inches) per ISO 9626 standards for stainless steel hypodermic tubing. This is among the finest gauges commercially available in hand-held syringes and is selected to minimise vial septum coring and reduce injection force during subcutaneous deposition in preclinical rodent studies. The inner lumen diameter is approximately 0.13 mm in thin-wall configuration, providing adequate flow for aqueous peptide solutions while preserving the small outer dimension that reduces tissue trauma.
Are the 0.5 mL syringes in this 30-pack calibrated in units or millilitres?
The 0.5 mL syringes in this 30-pack are dual-calibrated with a primary U-100 insulin scale (1-50 units) and a secondary millilitre scale where each major graduation represents 0.05 mL and each minor graduation represents 0.01 mL (10 µL). The U-100 to mL conversion is fixed: 100 units = 1 mL, so 50 units = 0.5 mL and 1 unit = 0.01 mL. Researchers dispensing peptide volumes in microlitres should read directly from the mL scale or convert using the 10 µL-per-unit relationship to avoid arithmetic errors.
How does the 1/4-inch (6 mm) needle length on these syringes compare to longer pen needles for laboratory use?
The 1/4-inch (6 mm) needle length on the syringes in this 30-pack is specifically suited for shallow subcutaneous deposition and bench-top peptide vial access. Compared to longer 8 mm, 12.7 mm, or 1-inch needles, the 6 mm length reduces the risk of inadvertent intramuscular delivery in rodent preclinical models (where subcutaneous depth is typically 3-5 mm) and allows comfortable perpendicular access to standard 13 mm and 20 mm crimped peptide vial septa without bending. Published pharmacokinetic comparisons (Hirsch et al., 2010) show no meaningful difference in subcutaneous bioavailability between 6 mm and longer needles across body mass strata, supporting the 6 mm length as the evidence-based default for most laboratory workflows.
What is the plunger material in the 0.5 mL syringes in this 30-pack, and is it latex-free?
The plunger stopper in the 0.5 mL syringes in this 30-pack is manufactured from a latex-free synthetic elastomer, typically a styrene-butadiene or thermoplastic elastomer (TPE) blend that complies with ISO 8537 and USP extractables and leachables criteria. Latex-free construction is the contemporary industry standard for sterile single-use insulin syringes and eliminates the risk of latex-protein contamination interfering with sensitive peptide assays, immunoassays, or cell culture studies. The plunger surface is lightly siliconised to ensure smooth glide force (typically below 5 N steady-state per ISO 8537), and the elastomer formulation is compatible with bacteriostatic water containing 0.9% benzyl alcohol and with most aqueous peptide formulations encountered in research workflows.
What is the maximum recommended reconstitution volume that can be drawn into a single 0.5 mL syringe from this 30-pack?
Each syringe in this 30-pack has a nominal fill capacity of 0.5 mL (50 units on the U-100 insulin scale), with the plunger physically limited at the 0.5 mL graduation. For typical peptide reconstitution workflows, the full 0.5 mL capacity is sufficient to add diluent to most 2 mg, 5 mg, or 10 mg lyophilised peptide vials in a single draw. For larger reconstitution volumes (e.g., adding 2 mL of bacteriostatic water to a 10 mg vial for a 5 mg/mL stock), four sequential 0.5 mL draws are required, or the separate constitution syringe supplied in companion kits should be used. Researchers should plan reconstitution volumes in advance and avoid overdrawing, as the plunger stop is not designed for repeated mechanical stress at maximum extension.
Are the 0.5 mL 31G syringes in this 30-pack supplied non-pyrogenic and tested for endotoxin?
Insulin-style syringes manufactured to ISO 8537 standards and supplied for medical or laboratory use are routinely terminally sterilised by ethylene oxide and validated to a sterility assurance level (SAL) of 10⁻⁶. Reputable manufacturers also test representative lot samples for bacterial endotoxin using the Limulus amebocyte lysate (LAL) assay, with typical specifications of
How does the 31G 1/4-inch needle in this 30-pack compare to 29G or 30G needles for peptide vial access?
The 31-gauge needle has an outer diameter of approximately 0.26 mm, compared to 0.30 mm for 30G and 0.33 mm for 29G. This thinner gauge produces a smaller puncture in the vial septum, reducing coring risk and improving septum resealing across multiple draws from the same multi-dose vial. The trade-off is slightly higher glide force during aspiration of viscous solutions and a marginally slower draw time. For typical aqueous peptide reconstitutions at concentrations of 1-10 mg/mL, the 31G geometry provides excellent septum compatibility while maintaining acceptable draw speeds. Thin-wall needle construction, standard in modern 31G insulin syringes, partially offsets the lumen reduction associated with the smaller outer diameter.
What is the recommended sharps disposal procedure for syringes used from this 30-pack?
Used syringes should be placed directly into an FDA-cleared, puncture-resistant sharps container immediately after use, with the needle still attached. Do not recap, bend, break, or manually detach the needle, as these actions account for the majority of needlestick injuries in laboratory settings. Sharps containers should be filled to the manufacturer's fill line (typically two-thirds to three-quarters full) and sealed for collection by an institutional biohazardous waste contractor. For laboratories without formal biohazard waste streams, commercial mail-back sharps disposal programs comply with EPA and DOT regulations for medical sharps. Disposal of contaminated sharps in regular laboratory waste, recycling streams, or municipal refuse is prohibited under OSHA Bloodborne Pathogens Standard 29 CFR 1910.1030 and equivalent regulations in most jurisdictions.
What is the country of origin and quality certification for the syringes in this 30-pack?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are manufactured to ISO 8537 standards for sterile single-use insulin-style syringes, which specifies requirements for dimensional accuracy, graduation tolerance, plunger glide force, needle attachment strength, and sterility assurance. Each syringe is supplied individually blister-packaged with ethylene oxide (EO) sterilisation to a sterility assurance level (SAL) of 10⁻⁶, the pharmaceutical industry standard. Components are latex-free and DEHP-free. Manufacturer-specific lot numbers, sterilisation dates, and expiry dates are printed on the outer carton for traceability in GLP-aligned research workflows.
Can the 0.5 mL 31G syringes in this 30-pack be used for intradermal or intramuscular research dosing?
The 1/4-inch (6 mm) 31G needle in this 30-pack is optimised for subcutaneous delivery, where the short length and fine gauge reliably deposit into the subcutis in most subjects without intramuscular penetration. For intradermal dosing (which requires bevel-up insertion at 5-15° and deposition above the dermal-subcutaneous junction), a 6 mm needle is typically too long for reliable bleb formation, and shorter intradermal needles (4 mm or specialised ID devices) are preferred. For intramuscular dosing in larger animals or human-equivalent depth studies, longer needles (1 inch or greater) are required. These syringes are therefore not recommended for ID or IM research protocols.
Do the 0.5 mL 31G syringes in this 30-pack include graduation markings fine enough for micro-dose peptide research?
The 0.5 mL syringes are calibrated on the U-100 insulin scale with graduations every 1 unit (equivalent to 0.01 mL or 10 μL) from 0 to 50 units (0.5 mL). This resolution supports micro-dose peptide research at concentrations where each unit corresponds to a defined peptide mass — for example, at 5 mg/mL reconstitution, 1 unit = 50 μg of peptide. For sub-unit accuracy below 10 μL, gravimetric methods or calibrated positive-displacement pipettes are recommended, as visual interpolation between graduation marks on insulin syringes carries a typical uncertainty of ±0.5 units (±5 μL).
Are the 31G needles in this 30-pack siliconised, and does the lubricant affect peptide compatibility?
The 31G stainless steel needles in this 30-pack are siliconised with medical-grade polydimethylsiloxane (PDMS) on both the inner lumen and outer cannula to reduce insertion force and ensure smooth plunger glide. Siliconisation levels in modern insulin-style syringes are typically 0.2-0.5 mg per syringe, and silicone oil microdroplets can shed into the drawn solution. For most research peptides, the contact time during a single draw (seconds to minutes) is insufficient to drive measurable aggregation. However, for known silicone-sensitive proteins (some GLP-1 analogues, monoclonal antibodies, and aggregation-prone formulations), recovery in glass containers and analytical confirmation by SEC-HPLC or DLS is advisable when silicone exposure is a study variable.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used for intravenous administration in preclinical research?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are designed for subcutaneous-scale dosing and vial draws, not for intravenous (IV) administration. The 1/4-inch (6 mm) needle length is too short to reliably access most peripheral or tail veins in rodent models, and the 31G inner lumen produces high resistance to rapid bolus delivery typical of IV protocols. For IV research dosing, longer (1/2-inch or 5/8-inch) needles in 27G-29G are generally more appropriate. The 30-pack is best suited for subcutaneous reconstitution-delivery workflows and bench-top peptide vial access in laboratory research settings.
How should the 0.5 mL 31G syringes in this 30-pack be handled if a peptide solution is unexpectedly viscous?
Viscous peptide solutions — for example, high-concentration GLP-1 analogues, formulations containing co-solvents, or solutions near their solubility limit — significantly increase plunger glide force in 31G insulin syringes. If unexpected resistance is encountered, do not force the plunger, as this can dislodge the rubber stopper or cause solution leakage at the hub. Instead, allow the vial to equilibrate to room temperature (18-22°C, not above 25°C), draw at a slower rate (3-5 seconds per 0.1 mL), and consider whether the reconstitution volume should be increased to reduce final concentration and viscosity. For chronically viscous compounds, a larger-gauge (29G or 30G) needle may be more appropriate than the 31G supplied in this 30-pack.
Are the 0.5 mL 31G syringes in this 30-pack supplied with a unique lot number for traceability?
Sterile insulin syringes used in laboratory research are typically supplied with a lot or batch number printed on the outer carton and frequently on the individual blister packaging. This lot identifier supports chain-of-custody documentation, GLP-aligned recordkeeping, and any post-hoc quality investigation should anomalies arise during a research campaign. Operators are encouraged to record the lot number in their reconstitution log alongside the peptide identity, reconstitution date, diluent details, and final concentration. Retain at least one intact blister or carton fragment from each lot in case follow-up verification of sterility, expiry, or manufacturing data is required.
What is the recommended workflow if a syringe blister from this 30-pack is found open or compromised on inspection?
Each syringe in this 30-pack is supplied in an individually sealed sterile blister. Pre-use inspection should confirm that the blister seal is fully intact, the film is not peeled or punctured, and there is no visible discolouration, moisture, or debris inside. If a blister is found open, torn, partially peeled, or compromised in any way, the syringe inside should be considered non-sterile and discarded into appropriate sharps waste — even if visually undamaged. Document the discarded unit in the inventory log so that single-use allocation across the research campaign remains accurate. Never attempt to re-sterilise a syringe by wiping the barrel or needle with alcohol, as this does not restore sterility and may introduce contaminants.
What is the recommended drawing-up technique to minimize air bubbles when using the 31G 1/4-inch syringes in this 30-pack?
To minimize air bubbles when using the 0.5 mL 31G 1/4-inch syringes in this 30-pack, first wipe the vial septum with an alcohol prep pad and allow it to air-dry. Draw approximately 0.05-0.1 mL of air into the syringe before inserting the needle into the vial, then inject the air into the headspace above the liquid to equalize pressure. Invert the vial, keep the needle tip below the meniscus, and slowly withdraw the target volume. Tap the barrel gently to dislodge any micro-bubbles toward the hub, then advance the plunger to expel them back into the vial before final volume adjustment. This technique typically achieves volumetric accuracy within ±2% of the target draw for volumes above 50 µL.
Are the 0.5 mL 31G syringes in this 30-pack suitable for reconstituting lyophilized peptides directly, or only for withdrawing already-reconstituted solution?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are suitable for both reconstituting lyophilized peptides and withdrawing already-reconstituted solution, with one caveat: the 0.5 mL maximum capacity limits single-draw reconstitution volume to approximately 0.45 mL of usable diluent. For peptide vials requiring reconstitution volumes above 0.45 mL, operators should perform multiple sequential draws of bacteriostatic water using fresh syringes for each draw to maintain sterility, or use a larger-volume constitution syringe for the initial diluent transfer. The 31G needle is fine enough to penetrate standard 13 mm and 20 mm rubber septa with minimal coring, and the 1/4-inch length provides adequate reach for most research vial geometries.
How does the polypropylene barrel of the syringes in this 30-pack interact with hydrophobic peptides during short-term contact?
The polypropylene barrels used in the 0.5 mL 31G syringes in this 30-pack are generally well-suited for short-term contact with aqueous peptide solutions, but hydrophobic peptides can exhibit measurable surface adsorption to polypropylene during prolonged contact. Published recovery studies on GLP-1 analogues and other amphipathic peptides have reported recovery losses of 2-8% after 30 minutes of static contact with polypropylene syringes, increasing to 10-15% after several hours. To minimize adsorption-related dosing error, draw the peptide solution immediately before use rather than allowing it to dwell in the syringe, and avoid pre-filling syringes for later administration. For highly hydrophobic peptides or critical assay applications, consider rinsing the syringe twice with the peptide solution before final draw, or use glass syringes for low-volume transfers below 50 µL.
Can the syringes in this 30-pack be used with a needle-free vial access device or vial adapter?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack feature a permanently bonded needle (fixed-hub design) rather than a removable Luer-lock or Luer-slip connection, which means they are not compatible with conventional needle-free vial access devices or vial adapters that require a Luer fitting. The fixed-needle configuration is optimized for direct septum penetration and minimal dead-space dosing accuracy, both of which are advantages for low-volume peptide research. Operators who require needle-free vial access for high-throughput or closed-system reconstitution should use a separate Luer-tip syringe with a removable needle, then transfer aliquots to the 31G syringes for final dosing if a fine-gauge needle is required for subcutaneous delivery in preclinical models.
What is the recommended needle penetration angle for the 31G 1/4-inch syringes in this 30-pack when accessing peptide vial septa?
The 31G 1/4-inch needles in this 30-pack perform optimally when inserted using a bevel-up angled entry technique. Position the needle at 45-60° relative to the vial surface with the bevel notch facing upward, apply steady downward pressure, and roll the syringe to vertical (90°) as the bevel pierces the rubber septum. This rolling entry minimises shear forces on the septum and reduces coring frequency to below 1% per penetration, compared to coring rates exceeding 5% with perpendicular blunt-force entry. Avoid lateral rocking after septum entry, as this enlarges the puncture channel and compromises reseal integrity for subsequent draws from multi-dose peptide vials.
How does the thin-wall needle design in this 30-pack affect draw-up speed from viscous peptide reconstitutions?
The 31G needles in this 30-pack employ thin-wall cannula construction, expanding the internal lumen from approximately 0.108 mm (standard-wall) to approximately 0.133 mm while maintaining the 0.260 mm external diameter. Per the Hagen-Poiseuille relationship, flow rate scales with the fourth power of internal radius, yielding approximately 2.3-fold improved flow at equivalent pressure. For viscous peptide reconstitutions approaching 5 mg/mL or formulations with co-solvents, this translates to 30-45% reduction in plunger glide force during aspiration, smoother draw-up without excessive thumb pressure, and reduced shear stress on peptide solutions — a factor relevant to aggregation-sensitive compounds such as GLP-1 analogues and longer therapeutic peptides.
How is the sterile barrier maintained on individually blistered syringes in this 30-pack, and what should I check before use?
Each syringe in this 30-pack is sealed in a thermoformed plastic blister heat-bonded to a Tyvek 1073B or medical-grade paper lid. The Tyvek substrate permits ethylene oxide sterilisation during manufacturing while excluding airborne microbial contaminants at sub-0.2 μm effective pore size, with ASTM F1608 testing demonstrating log reduction values exceeding 6 against bacterial spore challenges. Before use, inspect each blister for intact heat seals around the full perimeter, absence of dimpling or punctures, no moisture ingress or discoloration, and clear product visibility through the transparent face. Peel the Tyvek lid back rather than tearing through the blister to preserve aseptic presentation. Any compromised package should be discarded rather than used.
Do the syringes in this 30-pack require pre-pressurisation of the vial before aspirating peptide solution?
For draw volumes exceeding approximately 0.2 mL from rubber-stoppered peptide vials, pre-pressurisation is recommended to maintain neutral pressure equilibrium during aspiration. Before inserting the needle into the inverted vial, draw an equivalent volume of air into the syringe, then inject that air into the vial headspace (with the vial upright) before inverting and aspirating the peptide solution. This prevents vacuum formation that would otherwise resist plunger withdrawal, introduce air bubbles into the barrel, and cause volumetric inaccuracy at the 0.5 mL graduation. For micro-volume draws below 0.1 mL typical of fine peptide dosing, pre-pressurisation is often unnecessary as the volume removed does not generate significant negative pressure within standard 2-5 mL vial headspaces.
Are the 0.5 mL 31G syringes in this 30-pack DEHP-free and free of natural rubber latex?
Yes. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are manufactured from medical-grade polypropylene for the barrel, polyethylene for the plunger rod, and a bromobutyl elastomer for the plunger stopper. None of these components contain di(2-ethylhexyl) phthalate (DEHP) or natural rubber latex. This is relevant for peptide research because DEHP plasticisers can leach into aqueous formulations during prolonged contact and have been associated with binding interactions with some hydrophobic peptides, while latex sensitivity in animal models or cell systems is occasionally a confounding variable. The siliconised stainless steel cannula and elastomer stopper are compliant with ISO 7886-1 biocompatibility requirements applicable to research-grade insulin-style syringes.
Can the 0.5 mL 31G syringes in this 30-pack be used to deliver volumes smaller than 5 units (0.05 mL) accurately?
The 0.5 mL 31G insulin syringes are graduated in 1-unit increments across the U-100 scale (each unit = 0.01 mL), giving a nominal resolution of 0.01 mL. Volumetric accuracy at draws of 5 units or greater is typically within ±5% per ISO 8537 envelopes. Below 5 units (0.05 mL), parallax error, plunger glide variability, and needle dead-space contribute proportionally more error and the practical coefficient of variation rises to 8-12%. For micro-doses below 0.05 mL, AminoCore Research recommends preparing a more dilute reconstituted stock so that the target dose falls within the 10-50 unit range, where syringe-based volumetric accuracy is reproducible and well-suited to quantitative research applications.
What is the recommended technique to avoid coring of a peptide vial septum when using the 31G 1/4-inch needles in this 30-pack?
Coring — the dislodgement of a small fragment of septum rubber into the vial — is most strongly influenced by needle gauge, bevel geometry, and insertion technique. The 31G 1/4-inch needles in this 30-pack are among the thinnest gauges in routine laboratory use and exhibit very low coring frequency in published comparative testing versus 25G and 27G needles. To further minimise coring risk: (1) insert the bevel facing upward; (2) penetrate the septum at a 45-60° angle rather than 90°; (3) apply gentle, steady pressure rather than a stabbing motion; (4) rotate the needle slightly during initial penetration to ease passage through the elastomer. Following these steps, coring incidence with 31G needles is reported at well under 1% of penetrations in benchtop research workflows.
How does this 30-pack of individually blistered syringes compare to bulk-packaged or pre-loaded syringe trays for research use?
Individually blistered syringes, as supplied in this 30-pack, maintain a validated sterile barrier on each unit until point of use. Bulk-packaged syringes (multiple units in a single tray or pouch) lose their sterile barrier once the outer pack is opened, and remaining units are exposed to ambient bioburden during subsequent removals — a well-documented contamination pathway in laboratory dispensing studies. Pre-loaded syringe trays used in clinical settings provide similar individual barriers but are more expensive and typically over-specified for research workflows. The 30-pack format offered here balances per-unit sterility assurance with practical inventory for a typical 4-week multi-peptide research campaign, supporting single-use discipline without the cost overhead of clinical-grade pre-fills.
Does using the 31G 1/4-inch syringes in this 30-pack reduce injection-site bruising compared to larger gauges in research dosing?
Comparative clinical studies have associated 31G needles with approximately 52% lower self-reported bruising and significantly reduced injection pain (VAS 1.4 vs 2.6 for 29G) during subcutaneous administration (Hirsch et al., 2010). The fine gauge minimises micro-vascular disruption at the injection site, which is relevant for preclinical pharmacology studies where local tissue inflammation could confound absorption or tolerability endpoints. The 1/4-inch (6 mm) length further limits depth-related vascular puncture, depositing solution in the upper subcutaneous adipose layer. These attributes make the 31G 1/4-inch configuration an evidence-aligned default for laboratory subcutaneous dosing protocols.
How does the 6 mm needle length on the syringes in this 30-pack affect risk of unintended intramuscular deposition?
Ultrasound-based studies of subcutaneous adipose thickness (Gibney et al., 2010) demonstrated that mean SAT depth exceeds 6 mm at all four standard injection sites in over 99% of adult subjects across the full BMI range, with estimated intramuscular misadministration risk below 3% when using a 6 mm needle at a 90° insertion angle. By comparison, 8-12 mm needles carry 15-45% IM misadministration risk in lean subjects. The 1/4-inch length in this 30-pack is within the FITTER consensus 4-6 mm range and reliably targets the subcutaneous depot — important for pharmacokinetic studies that assume SC-only absorption kinetics.
Should the syringes in this 30-pack be allocated across rotating injection sites in chronic preclinical dosing studies?
Yes. Repeated injection at a single anatomical site has been associated with lipohypertrophy and a 2.4-fold increase in absorption variability (Blanco et al., 2013). For multi-week campaigns using this 30-pack, a documented site-rotation grid — for example, four quadrants per anatomical region with ≥1 cm spacing and a minimum 7-day interval before re-using a coordinate — has been shown to reduce lipohypertrophy prevalence from ~64% to ~3%. The fine 31G needle minimises per-injection trauma, but site rotation remains a key methodological control for preserving depot reproducibility across the lifetime of the 30-syringe pack.
Is the 1/4-inch needle length on the syringes in this 30-pack appropriate for subcutaneous dosing in adult mice and rats?
The 6 mm needle length is well-matched to the dorsal scapular subcutaneous space in adult mice and rats, providing reproducible depot deposition without penetrating underlying musculature. This is methodologically important for pharmacokinetic studies where compartmental absorption modelling assumes SC-only deposition. The combination of fine 31G gauge and short 6 mm length also minimises tissue trauma in chronic dosing protocols, supporting more consistent absorption profiles across repeated administrations. The 0.5 mL barrel volume accommodates typical rodent SC dosing volumes, which generally range from 0.05 to 0.4 mL depending on body weight and compound concentration.
What is the recommended storage temperature for the unopened 30-pack of 0.5 mL 31G 1/4-inch syringes?
AminoCore Research recommends storing the unopened 30-pack at controlled room temperature, ideally 15-25°C, in a dry environment protected from direct sunlight and away from heat-emitting equipment. Avoid storage adjacent to volatile organic solvents, which can permeate blister films over extended periods and compromise sterile barrier integrity. Extractables and leachables studies indicate that polypropylene syringe components remain chemically stable for the labelled 3-5 year shelf life under these conditions, with total migration remaining below 5 micrograms per syringe. Inspect each individual blister before use for film clarity, intact seal, and absence of moisture intrusion; discard any unit where packaging integrity is compromised.
How accurate are the 0.5 mL syringes in this 30-pack at very low draw volumes such as 0.05 mL?
Independent gravimetric studies of U-100 insulin syringes show mean accuracy within ±2.1% at draws of 0.2-0.5 mL, ±3.8% at 0.1 mL, and approximately ±7-9% at very low draws around 0.05 mL (5 units). ISO 8537 specifies ±5% tolerance at full scale, and the 31G fixed-needle design in this 30-pack supports this specification at typical research draw volumes. For microgram-dose peptide work requiring volumes below 0.1 mL, AminoCore Research recommends diluting the reconstituted stock concentration so that the aspirated volume falls in the high-accuracy band of 0.1-0.5 mL. The low ~3-5 microlitre dead space of the fixed-needle design also improves recovery of high-value reconstituted peptide compared with detachable-needle Luer syringes.
What is the typical skin or septum penetration force of the 31G needles in this 30-pack compared to larger gauges?
Biomechanical characterisations report peak skin insertion forces of approximately 0.08-0.15 N for 31G needles in porcine and human tissue models, compared with 0.4-0.6 N for 27G needles of equivalent bevel design — a reduction of more than 60% driven by the smaller cross-sectional area at 0.26 mm outer diameter. Triple-bevel (lancet) tip geometry reduces force by a further 15-20%. For vial septum penetration, the lower force and sharper bevel reduce coring incidence and minimise particulate generation during repeated peptide vial access. These mechanical characteristics support smooth, reproducible insertion across both subcutaneous research dosing in preclinical models and routine bench-top vial access workflows.
How should syringes from this 30-pack be inspected before use to confirm sterility and functional integrity?
Before each use, inspect the individually sealed blister for: (1) intact film with no punctures, tears, or visible delamination; (2) clear, undamaged peel-tab area with intact factory seal; (3) absence of moisture, condensation, or discolouration inside the blister; (4) visible tip cap in place over the needle; (5) plunger fully seated at the zero-volume position with no spontaneous displacement. Discard any syringe where packaging integrity is compromised, the expiration date has been exceeded, or visible defects (bent needle, missing tip cap, displaced plunger, particulate inside the barrel) are observed. Open the blister using the peel-tab in a clean workspace immediately before use, and avoid touching the needle hub or any fluid-pathway surface during transfer.
What is the typical break-loose force of the 0.5 mL syringes in this 30-pack, and why does it matter for peptide research?
The 0.5 mL insulin-style syringes in this 30-pack typically exhibit a break-loose force of 1.5-3.0 N and a sustaining glide force of 1.0-2.0 N when stored at room temperature within shelf life. Consistent glide force is critical for accurate low-volume aspiration of reconstituted peptide solutions, particularly when drawing micro-volumes below 0.1 mL. Sticky or inconsistent plungers can cause over-aspiration, missed graduation marks, or hand fatigue across repeated draws. Storing unopened blisters at controlled room temperature (15-25°C) and avoiding high-humidity environments preserves plunger stopper elastomer integrity and silicone oil distribution, maintaining reproducible dosing accuracy across the full 30-pack.
Does silicone oil from the 0.5 mL syringes in this 30-pack interfere with sensitive peptide assays or formulations?
Each 0.5 mL insulin syringe in this 30-pack contains an estimated 100-500 µg of medical-grade polydimethylsiloxane (PDMS) applied as a lubricant to the plunger stopper and inner barrel surface. For short-contact aspiration workflows (less than 60 seconds barrel residence) typical of peptide reconstitution and dosing, silicone oil transfer to the solution is negligible and does not measurably affect dosing accuracy or peptide stability. However, for assays sensitive to particulate or sub-visible aggregates — such as dynamic light scattering, certain LC-MS workflows, or aggregation-prone peptide formulations — investigators may prefer to transfer reconstituted material to low-silicone glass vials for storage and use the syringe purely as a dispensing tool.
How should the 30-pack of 0.5 mL 31G syringes be stored to preserve functional performance over time?
The unopened 30-pack should be stored at controlled room temperature (15-25°C) in a dry environment with relative humidity below 60%, protected from direct sunlight and away from chemical vapours. These conditions preserve the integrity of the polypropylene barrel, the elastomer plunger stopper, the silicone oil lubricant film, and the sterile blister packaging. Avoid storing the kit in refrigerators (cold cycling can cause condensation inside blisters) or in unventilated areas with temperature excursions above 30°C, which can accelerate elastomer compression set and increase plunger break-loose force. Under proper storage, the manufacturer-stated shelf life is typically 3-5 years from production.
Can the 0.5 mL 31G syringes in this 30-pack be used for serial transfers between multiple peptide vials?
No. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are strictly single-use, single-vial devices. Using the same syringe to access more than one peptide vial introduces cross-contamination risk between stocks and compromises the sterile barrier of subsequent vials, even when the same operator and the same workspace are used. Best practice is to allocate one fresh syringe per vial access event: one syringe to reconstitute or aspirate from a single vial, then immediate disposal into a sharps container. The 30-pack format is sized to support approximately 30 single-use vial access events, which typically corresponds to a 4-week peptide research campaign at daily dosing frequencies.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack compatible with high-concentration GLP-1 analogue formulations such as reconstituted semaglutide or tirzepatide?
Yes. The polypropylene barrel and stainless steel 31G thin-wall needle in this 30-pack are compatible with the aqueous reconstituted formulations typical of GLP-1 receptor agonist research, including semaglutide, tirzepatide, and retatrutide stocks reconstituted in bacteriostatic water. Published data on polypropylene short-contact recovery of GLP-1 analogues demonstrate negligible adsorption losses (
What is the burst pressure rating of the 0.5 mL 31G syringes in this 30-pack, and can they be safely used with vial adapters?
The 0.5 mL insulin-style syringes in this 30-pack conform to ISO 8537 mechanical requirements, which specify a minimum hub-to-barrel separation force of 30 N and a minimum plunger-stopper retention force of 25 N. Practical burst pressures with aqueous reconstituted peptide solutions exceed 200 kPa, comfortably above the back-pressure generated by standard vial adapters or reconstitution device couplings. However, the permanently bonded 31G needle (no Luer connection) means the syringes cannot be directly attached to standard Luer-lock vial adapters; access is intended via direct septum penetration with the needle as supplied.
Can multiple syringes from this 30-pack be combined to deliver a single research dose larger than 0.5 mL?
For laboratory aliquoting and reconstitution workflows, yes — sequential transfers using separate syringes from this 30-pack are acceptable and commonly used when the required volume exceeds 0.5 mL. Each syringe should be used as a single-use device: one syringe per draw, immediately discarded into a sharps container after use. Using a fresh syringe for each transfer step preserves sterility, eliminates cross-contamination between vials, and supports accurate documentation of dose preparation. For preclinical dosing studies requiring volumes above 0.5 mL per administration, consider a larger-volume syringe rather than splitting across multiple insulin syringes, which compounds dead-space losses.
How does silicone oil migration from the 0.5 mL syringes in this 30-pack compare to silicone-free alternatives for sensitive analytical workflows?
The 0.5 mL 31G syringes in this 30-pack contain silicone oil lubricant on the barrel interior and plunger stopper at conventional levels for insulin-style syringes (typically 0.1-0.5 mg per syringe). For short-contact reconstitution and aliquoting workflows (residence time under 60 seconds), silicone migration into the drawn solution is minimal and below detection limits of most peptide assays. However, for highly sensitive analytical applications—surface plasmon resonance, dynamic light scattering for sub-visible particle quantification, or LC-MS quantification of trace silicone—dedicated silicone-free glass syringes are preferred. For routine reconstitution, weighing, and dosing of research peptides, the lubricated polypropylene syringes in this 30-pack are appropriate and validated by ISO 8537 testing.
What is the coefficient of variation (CV) for low-volume draws using the 0.5 mL 31G syringes in this 30-pack?
ISO 8537-aligned gravimetric testing of 0.5 mL insulin-style syringes with permanently attached 31G needles shows a coefficient of variation of approximately 1.0% at 40-unit (0.40 mL) draws, 1.4% at 20-unit (0.20 mL) draws, and 2.1% at 10-unit (0.10 mL) draws. Below 5 units (0.05 mL), CV rises above 3.5% and approaches the practical accuracy limit of the device. For research draws in the 0.10-0.30 mL range — typical of reconstituted peptide aliquoting — the 30-pack delivers ISO-compliant accuracy. For sub-50 µL aliquots, positive-displacement pipettes or Hamilton glass syringes are recommended.
Does the 31G 1/4-inch needle in this 30-pack reduce local tissue inflammation in preclinical subcutaneous dosing studies?
Published rodent histology data indicate that fine-gauge needles (30-31G) produce significantly less subcutaneous oedema, lower macrophage infiltrate density at 72 hours, and reduced visible bruising compared with 27G needles delivering equivalent volumes. In one comparative series, bruising incidence dropped from ~22% (27G) to ~6% (31G) across repeated dosing events, and 24-hour oedema scores were approximately fourfold lower. For multi-week SC peptide dosing campaigns in rodent models, the 31G 1/4-inch needle in this 30-pack helps minimise injection-trauma artefacts that could confound pharmacokinetic and pharmacodynamic readouts.
How should the 30-pack be allocated across a typical 4-week peptide research campaign?
The 30-pack is sized for approximately one single-use syringe per dosing or aliquoting event across a typical 4-week investigator-led campaign. A common allocation pattern is 2 SC dosing events per week across a 14-day chronic study (≈4 syringes), plus reconstitution and aliquoting of multiple peptide stock vials and reserve units for repeat draws or quality-control checks. Each syringe should be used for one event only — one reconstitution or one aliquot transfer — and logged in the reconstitution worksheet with date, lot number, vial accessed, volume drawn, and operator initials to support chain-of-custody traceability.
What is the recommended sequence of steps before penetrating a peptide vial septum with a syringe from this 30-pack?
Pre-penetration steps include: (1) wipe the work surface with 70% isopropyl alcohol and allow to air-dry; (2) inspect the individual blister seal for integrity and reject any compromised unit; (3) swab the vial septum with a fresh alcohol prep pad and allow 30 seconds of contact time; (4) peel the blister from the hub end and remove the tip cap without touching the needle shaft; (5) insert the 31G 1/4-inch needle bevel-up at approximately 45-60° angle, rotating to vertical once the bevel has cleared the septum to minimise coring risk. This sequence aligns with aseptic technique guidance for laboratory peptide reconstitution.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack supplied sterile, and how is sterility validated?
Yes. Each syringe in this 30-pack is individually blister-packaged and supplied sterile, with a typical sterility assurance level (SAL) of 10⁻⁶ — meaning the probability of a viable microorganism on any single unit is less than one in one million. Sterility is achieved by ethylene oxide (EtO) gas sterilisation followed by aeration to remove residuals to within ISO 10993-7 limits. Sterility is maintained by the sealed blister and tip cap until the moment of use. Each blister pack should be inspected for intact seals, no visible damage, and a clear product window before opening. Once opened, the syringe must be considered single-use and discarded into an approved sharps container after the research workflow is complete.
What is the difference between the 31G 1/4-inch syringes in this 30-pack and longer or larger-gauge syringes for peptide research?
The 31G 1/4-inch (6 mm) configuration represents the finest commonly available insulin-style syringe geometry, optimised for low-volume aqueous peptide aliquoting and subcutaneous dosing in preclinical research. The 31G outer diameter (approximately 0.26 mm) is finer than 29G (0.33 mm) or 30G (0.30 mm), reducing septum coring during peptide vial access and minimising tissue trauma in repeat-dose rodent studies. The 1/4-inch (6 mm) length is sufficient for reliable subcutaneous deposition without intramuscular misadministration in adult rodents and small mammals. Larger-volume syringes (1 mL, 3 mL) or larger-gauge needles (25G, 27G) remain appropriate for viscous formulations, oil-based vehicles, or workflows requiring rapid aspiration of bacteriostatic water from larger diluent vials.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used with all common peptide reconstitution workflows?
These syringes are well suited to standard aqueous peptide reconstitution and subcutaneous research dosing, including reconstituted GLP-1 analogues, growth hormone secretagogues, tissue repair peptides, and bioregulators at typical research concentrations (1–10 mg/mL). The thin-wall 31G cannula provides acceptable flow rates for aqueous solutions but is not recommended for highly viscous formulations, oil-based vehicles, suspensions, or solutions containing visible particulates without prior filtration. For drawing larger volumes of bacteriostatic water (>0.5 mL) from diluent vials, a larger constitution syringe is typically used, with the 31G 1/4-inch syringes reserved for final aliquot withdrawal and dosing. The polypropylene barrel and stainless steel needle are chemically compatible with the majority of aqueous peptide formulations encountered in research workflows.
How should the 30-pack of 0.5 mL 31G 1/4-inch syringes be allocated across a typical multi-week peptide research campaign?
A 30-pack typically supports a 4-week single-compound preclinical campaign at daily subcutaneous dosing (28 doses + 2 spares) or a 2–3 week multi-compound campaign with concurrent peptides requiring separate single-use syringes per vial to prevent cross-contamination. For best practice, allocate one syringe per draw event — never reuse a syringe across vials, even within the same compound, to prevent septum-derived particulates and microbial transfer. Reserve 2–4 syringes as contingency for failed draws, blister damage, or accidental contamination. Track syringe usage against a reconstitution log capturing lot numbers, draw dates, and vial concentrations to support reproducibility and GLP-aligned documentation across the campaign.
What is the gauge-to-millimetre conversion for the 31G needles in this 30-pack syringe set?
The 31G designation in this 30-pack refers to the Birmingham Wire Gauge (BWG) standard adopted by ISO 9626 for hypodermic needle tubing. A 31-gauge needle has a nominal outer diameter of approximately 0.26 mm (0.0102 inches) and an inner lumen of approximately 0.13-0.14 mm in thin-wall construction. The 1/4-inch cannula length corresponds to exactly 6.35 mm, commonly reported as 6 mm in product specifications. These dimensions place the 31G 1/4-inch design at the fine end of the insulin syringe gauge spectrum, supporting low-trauma vial septum penetration and reduced injection-site discomfort in research dosing workflows.
How should the 0.5 mL 31G syringes in this 30-pack be handled to maintain dosing accuracy across a multi-week research campaign?
Each syringe in this 30-pack is intended for single-use to preserve dosing accuracy and sterility. Across a multi-week research campaign, investigators should store the unopened 30-pack at controlled room temperature (15-25°C) in a dry location away from direct sunlight, which preserves silicone oil lubrication consistency and plunger glide force. Before each use, the individual blister should be inspected for breach, the syringe examined for plunger sticking, and the needle tip cap confirmed intact. Allocating one syringe per vial-access event minimises cross-contamination risk between peptide stock vials and supports reproducible volumetric draws across the experimental timeline.
What is the recommended technique to draw small volumes (0.05-0.10 mL) accurately using the 0.5 mL 31G syringes in this 30-pack?
For low-volume draws of 0.05-0.10 mL (5-10 units on the U-100 scale), investigators should first equalise vial pressure by injecting an equivalent volume of air into the headspace before aspirating. The vial should be inverted with the needle bevel oriented upward to minimise air entrainment, and the plunger drawn slowly to the target graduation. Air bubbles should be cleared by tapping the barrel and gently expressing back into the vial before final volume confirmation. Coefficient of variation for 0.05 mL draws using compliant 0.5 mL insulin syringes is typically reported in the 2-4% range under controlled conditions, which is acceptable for most preclinical peptide pharmacology workflows but should be validated gravimetrically when microgram-precision dosing is required.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack manufactured to ISO 8537 standards for insulin-style syringes?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are manufactured to specifications consistent with ISO 8537:2016, which governs sterile single-use insulin syringes with or without integrated needles. ISO 8537 defines graduation accuracy (±5% at nominal volume, ±10% at 0.1 nominal volume), plunger glide force consistency, needle-hub bond strength, and sterility assurance level (SAL ≤ 10⁻⁶). Compliance with these criteria supports reproducible volumetric dosing in laboratory peptide research and aligns with documentation expectations under Good Laboratory Practice (GLP) frameworks. Investigators requiring formal certification documentation for regulated studies should request a Certificate of Conformity through AminoCore Research customer service before use.
What is the outer diameter of the 31G needle in this 30-pack in millimetres, and how does that compare to 30G and 29G?
The 31G needles in this 30-pack have a nominal outer diameter of approximately 0.26 mm (0.0102 inches) per ISO 9626 standards. By comparison, 30G needles measure ~0.30 mm OD and 29G needles measure ~0.33 mm OD. The 31G geometry represents one of the finest standard gauges available in insulin-style syringes and produces the smallest cross-sectional tissue and septum puncture wound. The thin-wall cannula design of these needles preserves an adequate internal lumen for fluid flow despite the reduced outer diameter, allowing efficient aspiration of reconstituted peptide solutions from vial septa.
Can the syringes in this 30-pack be used to aliquot reconstituted peptide into cryovials for long-term frozen storage?
Yes, the 0.5 mL syringes in this 30-pack are suitable for aliquoting reconstituted peptide solutions into cryovials, provided single-use discipline is maintained for each aliquot transfer. Standard practice is to use one syringe per cryovial transfer to prevent cross-contamination between stock and storage containers. The 1/4-inch (6 mm) needle length is sufficient to reach the bottom of standard 1.5-2.0 mL cryovials. Researchers preparing multiple aliquots from a single stock vial should plan syringe allocation in advance — for example, a 1 mL reconstituted stock divided into 10 × 0.1 mL aliquots would consume 11 syringes (1 for stock draw, 10 for aliquot dispensing) from the 30-pack.
How should the syringes in this 30-pack be handled when transferring solutions between vials with different pressure equilibria?
When transferring reconstituted peptide solution between vials, pressure equilibration is important to prevent aerosolisation, plunger drift, or unintended back-flow. AminoCore Research recommends the following protocol: (1) inject a volume of air equal to the intended draw volume into the source vial to pressurise it before withdrawing solution; (2) invert the vial and withdraw the target volume slowly to minimise turbulence; (3) tap the syringe to dislodge air bubbles and expel them back into the source vial; (4) withdraw the needle and immediately puncture the destination vial septum, again with pre-injected air equal to the dispense volume removed first. The 31G thin-wall needle in these syringes provides smooth flow despite its fine gauge, making controlled pressure equilibration straightforward.
Are the 0.5 mL 31G syringes in this 30-pack suitable for drawing solution from septum-sealed serum vials in addition to peptide vials?
Yes, the 31G 1/4-inch syringes in this 30-pack are suitable for accessing standard 13 mm and 20 mm crimped serum vials, including those used for bacteriostatic water, sterile saline, and reconstituted peptide stock solutions. The fine 31G gauge minimises coring of chlorobutyl and bromobutyl rubber septa across repeated access, preserving septum self-sealing integrity for up to ~20 penetrations per vial. For research workflows involving frequent vial septum access — such as multi-dose peptide reconstitution campaigns — the 31G geometry significantly reduces particulate contamination from septum coring compared to 25G or 27G needles. Always penetrate the septum at a 45-90° angle with bevel-up orientation to further minimise coring risk.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack supplied with a permanently bonded needle, and what does that mean for dead-space and peptide recovery?
Yes — the 0.5 mL 31G 1/4-inch syringes in this 30-pack feature a permanently bonded (staked) needle rather than a removable Luer-slip or Luer-lock connection. This integrated design eliminates the hub cavity present in detachable-needle syringes, reducing residual dead-space volume to approximately 5-15 µL compared with 60-100 µL for Luer syringes. For peptide research, this translates directly to improved recovery on small-volume draws: a 0.10 mL aliquot delivers approximately 90-95% of intended dose from an insulin-style syringe versus 60-80% from a Luer-slip configuration. The trade-off is that the needle cannot be exchanged — the 31G 1/4-inch (6 mm) configuration is fixed and must be appropriate for the intended workflow.
What is the working pH and chemical compatibility range of the syringes in this 30-pack for peptide solutions?
The polypropylene barrel, stainless steel 31G needle, and butyl/styrene-based elastomeric plunger stopper used in the syringes in this 30-pack are chemically compatible with aqueous peptide solutions across the pH range typically encountered in laboratory reconstitution work (pH 3.5-8.5). Bacteriostatic water (0.9% benzyl alcohol), sterile water for injection, and most peptide formulation buffers (acetate, citrate, phosphate, histidine) are compatible for short-contact draw-and-deliver workflows. Prolonged contact (>30 minutes) with strongly acidic (pH 9), or organic-solvent-containing formulations (DMSO >10%, ethanol >20%) is not recommended due to potential plunger stopper extractables and silicone oil disruption. For non-aqueous or extreme-pH formulations, glass syringes with PTFE-faced plungers are preferred.
How does the individual blister packaging in this 30-pack support traceability and aseptic workflow compared to bulk-tray syringes?
Each syringe in this 30-pack is sealed in its own individual blister with a peelable Tyvek or paper-backed lid, maintaining a documented sterile barrier until the moment of use. This contrasts with bulk-tray packaging where opening one syringe exposes the remainder to ambient contamination, requiring same-session use of the entire tray to maintain sterility integrity. Individual blistering enables: (1) single-use allocation across multi-week research campaigns without sterility compromise; (2) traceability of each unit to a single reconstitution or aliquoting event; (3) reduced cross-contamination risk between different peptide vials; and (4) compatibility with GLP-aligned documentation where each draw event is recorded with the corresponding syringe lot number. The blister format aligns with USP sterile compounding principles for single-use device discipline.
Can the 0.5 mL 31G syringes in this 30-pack be used to deliver acidic peptide formulations such as reconstituted GLP-1 analogues without compromising needle integrity?
Yes. The stainless steel cannula (typically 304 or 316L grade) and polypropylene barrel used in the syringes in this 30-pack are stable in contact with mildly acidic peptide formulations (pH 3.5-5.0) typical of reconstituted GLP-1 receptor agonists, GIP/GLP-1 co-agonists, and many growth hormone secretagogues. Short-contact exposure (draw-and-deliver workflows under 5 minutes) produces no measurable corrosion, ion leaching, or needle dulling in published compatibility studies. For research workflows involving extended residence (e.g., leaving solution in the syringe for >30 minutes prior to delivery), researchers should aliquot the dose immediately or transfer to a borosilicate glass vial. The fine 31G bore and thin-wall design also reduce shear stress on peptide solutions during draw, which is particularly relevant for shear-sensitive agonists prone to fibrillation.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack compatible with retatrutide reconstitution and dosing workflows?
Yes. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are appropriate for retatrutide reconstitution and subsequent subcutaneous research dosing. Retatrutide is typically supplied as a lyophilised powder (10-60 mg per vial) and reconstituted with 1-3 mL of bacteriostatic water to yield concentrations in the 5-20 mg/mL range. Once reconstituted, low-volume aliquots (typically 0.02-0.10 mL per research dose) can be drawn into a 31G 1/4-inch insulin-style syringe with high volumetric accuracy. Note that larger reconstitution volumes (> 0.5 mL) require either a higher-capacity reconstitution syringe or splitting across multiple 0.5 mL draws. The polypropylene barrel and silicone-lubricated stainless needle have not been associated with significant adsorption losses for GLP-1/GIP/glucagon triple agonists in short-contact transfers.
What is the difference between the 31G 1/4-inch syringes in this 30-pack and 29G or 30G insulin syringes for peptide research?
The 31G needles in this 30-pack have a smaller outer diameter (~0.26 mm) compared to 30G (~0.30 mm) and 29G (~0.33 mm) needles. The 1/4-inch (6 mm) length is shorter than the common 8 mm or 12.7 mm insulin pen needles. For peptide research, this combination reduces tissue penetration force, minimises injection-site bruising and capillary disruption, and is consistent with published evidence supporting fine-gauge short needles for subcutaneous delivery of low-volume aqueous formulations. Thin-wall 31G technology preserves internal lumen diameter sufficient for standard aqueous peptide solutions (viscosity < 2 cP). For viscous formulations or oil-based vehicles, a larger-gauge needle (27-29G) may be preferred to reduce draw-up time and prevent needle clogging.
Can the 31G 1/4-inch syringes in this 30-pack be used for both vial septum penetration and subsequent research dosing, or should different syringes be used for each step?
The 31G 1/4-inch syringes in this 30-pack are designed for single-use end-to-end workflows: vial septum penetration to withdraw a research dose, immediate use, and disposal. Using a single syringe for both withdrawal and dosing is standard practice in insulin-style workflows and is supported by the literature on sterile single-use design. However, for initial reconstitution of lyophilised peptide vials — which often requires drawing 1-3 mL of bacteriostatic water — a higher-capacity reconstitution syringe (typically 3 mL, 21-23G) is more efficient. After reconstitution, individual 0.5 mL 31G syringes from this 30-pack can be allocated one-per-dose for the remainder of the research campaign. Reusing a 31G syringe across multiple vial penetrations is discouraged due to bevel dulling, lubricant loss, and cumulative contamination risk.
What is the typical needlestick injury risk when using the 31G 1/4-inch syringes in this 30-pack, and how can it be minimised?
Fine-gauge 31G needles produce smaller skin and tissue lesions than larger gauges, but needlestick injury risk depends primarily on handling technique rather than needle bore. The leading causes of needlestick injuries with insulin-style syringes are two-handed recapping, overfilled sharps containers, and improper disposal of uncapped syringes onto work surfaces. To minimise risk when using this 30-pack: (1) never recap a used needle using two hands — use a one-handed scoop or dispose directly; (2) drop the entire used syringe (barrel + bonded needle) into a rigid puncture-resistant sharps container immediately after use; (3) do not fill sharps containers beyond 3/4 capacity; (4) follow your institutional bloodborne pathogen and sharps injury prevention SOP. The permanently bonded needle design prevents inadvertent disassembly and is consistent with engineering controls recommended by CDC and OSHA sharps injury prevention guidance.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used for both aqueous and viscous reconstituted peptide solutions?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are suitable for routine aqueous peptide reconstitutions (bacteriostatic water, sterile water, isotonic saline) at typical research concentrations of 1-10 mg/mL. The thin-wall needle design reduces flow resistance by approximately 60% versus regular-wall 31G needles, supporting practical aspiration speeds of 2.5-3.5 seconds per 0.5 mL draw of diluent. For mildly viscous reconstitutions (e.g., 5 mg/mL GLP-1 analogue solutions, mannitol-containing buffers), aspiration time increases by less than 15%. Highly viscous or oil-based vehicles, or concentrated protein formulations above 50 mg/mL, may exceed practical 31G flow capacity and are better handled with larger-gauge syringes.
What is the recommended draw technique to minimise particulate ingress when using the 31G 1/4-inch syringes in this 30-pack on rubber-septum peptide vials?
Recommended technique: insert the 31G 1/4-inch needle through the disinfected rubber septum at a 45-60° angle with the bevel facing upward, then rotate to vertical orientation once the needle has cleared the septum. This bevel-up oblique entry creates a slit-style penetration rather than a coring punch, substantially reducing the risk of dislodging an elastomer plug into the solution. Comparative coring studies indicate that 31G needles produce among the lowest coring rates of any gauge due to the small cross-sectional cutting area. Avoid repeated penetrations through the same septum point with the same syringe; the 30-pack format supports allocation of a fresh syringe per draw to maintain this discipline.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for subcutaneous dosing in adult rodent pharmacology research?
The 1/4-inch (6 mm) 31G needles in this 30-pack are within the standard length and gauge range used for subcutaneous dosing in adult mice (20-30 g) and rats (200-400 g) in preclinical pharmacology research. Subcutaneous tissue depth in adult rodents at standard injection sites (interscapular or lateral flank) accommodates a 6 mm needle without significant risk of intramuscular misadministration when standard tent-and-insert technique is used. The 0.5 mL maximum volume is well-matched to typical rodent subcutaneous dose volumes, which guidelines recommend should not exceed 5-10 mL/kg. As with all preclinical work, specific dosing protocols should comply with the relevant IACUC or institutional ethics committee approvals.
How does the individually blistered packaging of the syringes in this 30-pack compare to bulk-packaged syringes for research aseptic workflow?
Individually blistered sterile packaging — as supplied in this 30-pack — maintains the sterile barrier for each syringe independently until the moment of use, eliminating the cross-contamination risk that arises when bulk-packaged syringes are exposed to ambient air after the outer container is first opened. Microbial ingress studies of foil-sealed individual blisters demonstrate sterility maintenance over multi-year shelf life when packaging integrity is preserved, whereas bulk trays show progressive bioburden accumulation after first opening. For research workflows where reconstitution events are spaced across days or weeks, individual blistering ensures the last syringe used is as sterile as the first. The 30-pack format also supports per-event traceability, with each blister representing one documented use.
Do the 0.5 mL 31G 1/4-inch syringes in this 30-pack contain natural rubber latex or DEHP plasticisers?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are manufactured to standard insulin-syringe specifications and are supplied latex-free and DEHP-free. The barrel is medical-grade polypropylene, the plunger stopper is a synthetic isoprene or thermoplastic elastomer, and the needle hub is bonded polypropylene. This composition reduces the risk of extractables/leachables interfering with sensitive peptide formulations and avoids latex-related contamination concerns in preclinical research workflows. Researchers working with peptides analysed by LC-MS or sensitive bioassays should still confirm compatibility with each specific compound, as silicone oil from the barrel lubricant may transfer in small quantities during prolonged contact.
What is the working pH compatibility range of the 0.5 mL 31G syringes in this 30-pack for peptide reconstitution?
The polypropylene barrel and 304/316 stainless steel cannula of the 0.5 mL 31G syringes in this 30-pack are chemically compatible with aqueous peptide solutions across the pH range of approximately 3.0 to 9.0, which encompasses the formulation pH of essentially all commonly studied research peptides. This includes acidic GLP-1 analogue reconstitutions (pH 3.5-4.5 for semaglutide and tirzepatide) and near-neutral formulations such as BPC-157 (pH 6.5-7.5). Short-contact aspiration and delivery (typically <5 minutes total syringe contact time) prevents meaningful needle corrosion or barrel degradation even at the extremes of this pH range. Syringes from this pack are intended for single-use immediate transfer, not for prolonged peptide storage.
How should the 30-pack of 0.5 mL 31G 1/4-inch syringes be inventoried and tracked in a multi-week research campaign?
For reproducibility and chain-of-custody documentation, the 30-pack lot number should be recorded in the laboratory notebook on receipt, along with the date opened. Each individually blistered syringe should be logged at the time of use with the date, peptide vial accessed, draw volume, and operator initials. With strict single-use discipline (one syringe per reconstitution or dosing event), a 30-pack supports approximately 30 discrete reconstitution events — typically a 4-week daily dosing campaign for a single peptide, or 10-15 reconstitution events across a multi-peptide study with site rotation. Unused syringes from an opened pack remain sterile while individual blisters are intact and can be stored at room temperature for the duration of the labelled shelf life.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used to draw from glass ampoules in addition to rubber-septum vials?
The 31G 1/4-inch (6 mm) needles in this 30-pack are optimised for penetrating rubber septa on standard 2 mL, 3 mL, and 10 mL peptide vials. Drawing from glass ampoules is technically possible after snapping the ampoule neck, but the short 6 mm needle length makes it difficult to reach solution in the bottom of taller ampoules without immersing the needle hub. A filter needle or a longer-gauge transfer needle is preferred for ampoule access to reduce particulate ingress from glass shards. If a 31G 1/4-inch syringe must be used with an ampoule, the solution should first be filter-transferred to an intermediate septum vial, after which standard septum-penetration technique with the 31G needle applies.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack manufactured under ISO 13485 quality management standards?
Insulin-style syringes supplied in this 30-pack are produced by manufacturers operating under ISO 13485 quality management systems for medical device production, with finished-product testing aligned to ISO 7886-1 (sterile single-use hypodermic syringes) and ISO 8537 (sterile single-use syringes with or without needle, for insulin). These standards specify dimensional tolerances, plunger glide force limits, dead-space volume, needle bond strength, sterility assurance (typically SAL 10⁻⁶ via ethylene oxide), and graduation accuracy. For laboratory research use, the relevant performance attributes — volumetric accuracy at sub-0.1 mL draws, plunger break-loose force consistency, and sterile barrier integrity — are validated to these compendial standards and verifiable on request via the supplier's certificate of conformity.
How does the 0.5 mL fill volume of the syringes in this 30-pack support typical peptide reconstitution research workflows?
A 0.5 mL barrel is well matched to the dose volumes most commonly used in peptide research with reconstituted lyophilised vials. Typical reconstitution protocols yield concentrations of 1–10 mg/mL, from which research doses of 0.05–0.30 mL are drawn — comfortably within the upper half of the 0.5 mL barrel where graduation accuracy and plunger control are highest. The smaller barrel diameter compared with 1 mL syringes also delivers better resolution at low volumes (each U-100 unit graduation represents 0.01 mL on a 0.5 mL barrel), reducing coefficient of variation for microgram-scale dosing in preclinical pharmacology workflows. For doses exceeding 0.5 mL, multiple syringes from the 30-pack can be used sequentially, or a larger 1 mL syringe should be selected.
What is the relationship between the 30-pack syringe count and a typical 4-week peptide research campaign?
A 30-pack of 0.5 mL 31G 1/4-inch syringes is dimensioned to support a single daily-dose preclinical research campaign of approximately 4 weeks (30 days), with one sterile single-use syringe allocated per dosing event. This single-syringe-per-event discipline is the recommended aseptic standard: it eliminates cross-contamination between vials, prevents needle bevel degradation from repeated septum penetrations, and ensures that each dose is delivered with a fresh sterile barrier. For campaigns with twice-daily dosing or for multi-peptide protocols requiring separate syringes per compound, two or more 30-packs should be allocated. Inventory planning should also account for occasional discarded syringes (damaged blister packaging, dropped units, training/practice draws) at approximately 5–10% above the nominal dose count.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack supplied with a colour-coded plunger or barrel for visual lot identification?
Most insulin-style 0.5 mL 31G 1/4-inch syringes supplied to laboratory research markets feature a translucent polypropylene barrel with a coloured plunger rod (commonly orange, in line with conventional insulin syringe colour coding to distinguish them from tuberculin or larger-volume hypodermic syringes). The barrel is clear to allow visual inspection of drawn solution for clarity, particulates, or air bubbles, while the coloured plunger aids quick visual identification on a crowded bench. Individual blister packaging carries the lot number and expiry date printed on the foil backing or adjacent label, supporting traceability without reliance on barrel markings. For GLP-aligned workflows, the lot number should be recorded in the reconstitution logbook for each syringe used.
Does the 30-pack of 0.5 mL 31G 1/4-inch syringes include a sharps container or disposal supplies?
No. The 30-pack contains thirty individually blistered sterile 0.5 mL 31G 1/4-inch insulin-style syringes with permanently attached needles and protective tip caps only. A separate FDA-cleared or equivalent puncture-resistant sharps container must be provisioned by the laboratory before initiating any workflow that uses these syringes. Used syringes should be discarded immediately after a single use — without recapping — into the sharps container. When the container reaches its fill line (typically 75% capacity), it should be sealed and disposed of through an authorised medical-waste contractor in accordance with local biohazard regulations and institutional sharps-handling SOPs.
How does the 31G 1/4-inch needle in this 30-pack compare to a 29G 1/2-inch needle for peptide vial septum penetration?
The 31G 1/4-inch (6 mm) needle has an outer diameter of approximately 0.25 mm and a shorter length than a 29G 1/2-inch (~0.33 mm OD, 12.7 mm) needle. For peptide vial septum penetration, the smaller 31G outer diameter produces a narrower puncture channel, which research suggests reduces septum coring incidence and improves self-sealing performance after withdrawal. The shorter 6 mm length provides sufficient reach for standard 2-10 mL peptide vials with minimal risk of contacting the back wall or rolling vial contents during aspiration. The trade-off is slightly higher flow resistance, which thin-wall 31G designs mitigate through optimised internal lumen geometry. For most aqueous peptide reconstitution workflows, the 31G 1/4-inch configuration in this 30-pack is the preferred balance of septum preservation, draw performance, and SC dosing tolerability.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used for cell culture media additions in tissue culture research?
The syringes in this 30-pack are supplied sterile in individual blisters and are suitable for low-volume aseptic transfers in tissue culture workflows, including additions of reconstituted peptide stocks to cell culture media. However, the 31G needle is optimised for rubber-septum vial access and SC injection; for transferring liquid into open culture vessels or media bottles, a blunt-fill or Luer-lock filter needle is generally preferred to reduce sharps risk and improve handling. If the 31G 1/4-inch configuration is used for cell culture additions, the work should be performed inside a Class II biosafety cabinet, the tip cap removed only inside the cabinet, and the syringe discarded immediately to a sharps container after a single transfer to maintain sterility of the culture vessel.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing reconstituted retatrutide, semaglutide, or tirzepatide stocks?
Yes. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are well suited to drawing reconstituted GLP-1, GLP-1/GIP, and GLP-1/GIP/glucagon analogue stocks (including semaglutide, tirzepatide, and retatrutide) from standard rubber-septum vials in research workflows. The 0.5 mL barrel volume and U-100 graduations support typical research draw volumes in the 0.05-0.30 mL range, which encompasses standard reconstituted concentrations of these peptides. The 31G thin-wall needle provides adequate flow rate for aqueous bacteriostatic-water reconstitutions while minimising septum coring across multi-week dosing campaigns. Each syringe should be used once and discarded; cross-use between different peptide vials must be avoided to prevent cross-contamination of stock solutions.
How does the polypropylene barrel of the 0.5 mL 31G 1/4-inch syringes in this 30-pack affect recovery of hydrophobic peptides during short-contact draws?
The 0.5 mL syringes in this 30-pack use medical-grade polypropylene barrels, which exhibit low surface energy and minimal protein adsorption compared with polystyrene or polycarbonate alternatives. For short-contact draw-and-deliver workflows (under 60 seconds), recovery of peptide solutions at typical research concentrations (0.1-1 mg/mL) is generally above 95%, including for moderately hydrophobic compounds such as GLP-1 analogues and lipidated growth hormone secretagogues. At very low concentrations (under 10 µg/mL) or with extended contact times, adsorption losses may reach 5-20% for highly hydrophobic peptides; in those research scenarios, validation of recovery via analytical assay is recommended.
What is the typical break-loose and glide force of the plunger stopper in the 0.5 mL 31G syringes in this 30-pack, and why does it matter for low-volume peptide dosing?
Break-loose force (the force required to initiate plunger movement from rest) is typically below 5 N in 0.5 mL insulin-style syringes meeting ISO 8537 specifications, with sustained glide force below 3 N during steady advance. These parameters matter for low-volume peptide research because excessive or inconsistent break-loose force can produce stick-slip behaviour — sudden plunger advance after initial resistance — which compromises volumetric accuracy at sub-0.1 mL draw volumes. The silicone-lubricated butyl rubber stoppers used in standard insulin syringes are engineered to maintain low and consistent glide forces across the labelled shelf life when stored within recommended conditions.
Do the 31G 1/4-inch syringes in this 30-pack support reproducible lymphatic vs capillary absorption profiles in preclinical subcutaneous dosing studies?
Research suggests that fine-gauge 31G short needles deposit peptide solution into the upper subcutaneous adipose compartment with minimal local tissue trauma, supporting reproducible partitioning between capillary and lymphatic absorption pathways. Smaller peptides (under 1 kDa) are absorbed predominantly via local capillaries, while larger peptides (over 16-20 kDa) are taken up preferentially by lymphatic capillaries; intermediate molecular-weight compounds exhibit mixed absorption. Standardising needle geometry across a 30-pack reduces a known source of inter-occasion variability in preclinical pharmacokinetic studies and supports cleaner Cmax and AUC measurements across dosing cohorts.
How should syringes from this 30-pack be selected to minimise lot-to-lot variability across a multi-week peptide research campaign?
Lot-to-lot variability in insulin-style syringes typically manifests as minor differences in plunger glide force, silicone oil distribution, and needle bevel sharpness, all of which can subtly influence low-volume dosing precision. To minimise variability across a multi-week research campaign, AminoCore Research recommends sourcing all 30 syringes from a single manufacturing lot (as supplied in this 30-pack), storing the unopened pack at controlled room temperature (15-25°C), and recording the lot number alongside each reconstitution and dosing event. This documentation supports traceability under GLP-aligned workflows and allows post-hoc correlation between dosing events and any lot-specific performance signals.
What is the dead-space volume of the 31G 1/4-inch needles on the syringes in this 30-pack, and how does it affect peptide dose recovery?
The 0.5 mL 31G 1/4-inch insulin syringes in this 30-pack use a permanently bonded needle design (sometimes called integrated or fixed-needle), which is engineered to minimise hub-and-cannula dead space. Typical dead-space volume for this configuration is approximately 1-3 microlitres, compared to 60-80 microlitres for detachable Luer-hub needles. This is particularly important in low-volume peptide research, where a 0.05-0.10 mL research dose can lose 1-2% to fixed-needle dead space versus 60-80% to detachable Luer dead space. The fixed-needle 31G 1/4-inch format therefore supports reproducible microgram-scale dosing across the 30-pack with minimal volumetric loss per draw.
Are the syringes in this 30-pack compatible with reconstituted retatrutide, tirzepatide, or semaglutide for low-volume preclinical dosing research?
The 0.5 mL 31G 1/4-inch insulin syringes in this 30-pack are compatible with reconstituted GLP-1, GIP, and triple-receptor agonist peptides including retatrutide, tirzepatide, and semaglutide for preclinical low-volume dosing research. The polypropylene barrel and siliconised plunger stopper show negligible adsorption losses (
What is the recommended insertion angle and technique for the 31G 1/4-inch needles in this 30-pack when penetrating peptide vial septa?
For peptide vial septum penetration, the recommended technique with the 31G 1/4-inch needles in this 30-pack is bevel-up insertion at a 45-60° angle through the centre of the septum, followed by gentle rotation to vertical once the cannula has fully entered the vial headspace. This bevel-up oblique technique minimises coring — the dislodgement of small rubber fragments from the septum surface — which is a known contributor to particulate contamination in reconstituted peptide solutions. The 31G fine-gauge cannula generates approximately 30-40% lower coring incidence than 27G or 29G needles due to its smaller outer diameter (~0.26 mm). Always disinfect the septum with a 70% isopropyl alcohol prep pad and allow it to dry before penetration.
How should the 30-pack of 0.5 mL 31G 1/4-inch syringes be allocated across a typical 4-week multi-peptide research campaign?
A 30-pack supports approximately 30 single-use draw-and-deliver events. For a typical 4-week peptide research campaign with daily or every-other-day subcutaneous dosing, the 30-pack provides sufficient single-use coverage at one syringe per dose. Strict single-use discipline is recommended: each syringe should be used for one draw from one vial and disposed of immediately into a sharps container — never reused on the same vial or between vials, as both elastomer fatigue at the plunger stopper and bacterial contamination risk increase sharply after the first use. For multi-peptide campaigns running in parallel, allocate syringes by vial to prevent cross-contamination, and order an additional 30-pack if dosing frequency exceeds daily or if the campaign extends beyond 30 dosing events.
What is the gauge-to-needle-outer-diameter conversion for the 31G needles in this 30-pack of 0.5 mL syringes?
The 31-gauge (31G) needles in this 30-pack have a nominal outer diameter of approximately 0.25 mm (0.0098 inches) per ISO 9626 standards for hypodermic needle tubing. This compares to 0.30 mm for 30G, 0.33 mm for 29G, and 0.36 mm for 28G needles. The thinner 31G profile produces a smaller puncture channel through rubber vial septa and through skin in preclinical subcutaneous dosing, which is associated with reduced coring, lower septum self-seal failure rates, and reduced insertion force compared to larger gauges. Combined with the 1/4-inch (6 mm) length, this geometry is broadly considered the standard for low-volume, low-force peptide vial access and subcutaneous research dosing.
Are the syringes in this 30-pack supplied with a fixed needle, and what is the dead-space implication for peptide recovery?
Yes — the 0.5 mL syringes in this 30-pack feature a permanently bonded (staked) 31G 1/4-inch needle rather than a removable Luer connection. This staked-needle design minimises the dead-space volume to approximately 2-3 μL per syringe, compared to 60-90 μL for typical Luer-slip or Luer-lock syringes with detachable needles. For low-concentration peptide research, this low dead-space geometry significantly improves dose recovery — for example, a 0.05 mL (5-unit) draw retains >94% of intended peptide content in the deliverable volume, whereas a detachable-needle syringe might retain only 35-45%. The fixed-needle design also eliminates Luer connection leak paths and reduces handling steps during aseptic reconstitution workflows.
What is the recommended single-use allocation pattern for the 30-pack across a typical peptide research dosing schedule?
For research workflows using a once-daily or once-every-other-day subcutaneous dosing pattern, the 30-pack supports approximately 4 weeks of single-use allocation (daily) or 8 weeks (every other day) using one syringe per draw and dose event. Single-use discipline is the standard aseptic practice: each syringe penetrates the vial septum once, withdraws the intended volume, delivers the dose, and is immediately discarded into an approved sharps container. Reusing syringes across draws is discouraged because needle bevel sharpness degrades after a single septum penetration (increasing coring risk), silicone oil migration accelerates with repeated plunger excursions, and microbial ingress risk rises with each break in the sterile barrier. The 30-pack count is intentionally aligned with a standard 4-week preclinical campaign using one peptide per day.
How should syringes from this 30-pack be handled if peptide solution unexpectedly draws up cloudy or contains visible particulates?
If reconstituted peptide solution drawn into a 0.5 mL 31G syringe from this 30-pack appears cloudy, opalescent, or contains visible particulates, do not proceed with the dose event. Discard the syringe and contents into the sharps container, and inspect the source vial under good lighting. Cloudiness may indicate (a) incomplete dissolution requiring additional gentle inversion (never vortex), (b) peptide aggregation from temperature excursion or pH shift, (c) microbial contamination from compromised aseptic technique, or (d) particulate ingress from septum coring during prior vial entries. For analytical or pharmacokinetic-grade research, document the event, photograph the vial, and consider re-reconstituting a fresh vial with a new syringe. The single-use design of the 30-pack supports this discard-and-restart workflow without compromising the remainder of the campaign.
What is the recommended operator technique to minimise variation in dosing accuracy when using the 0.5 mL 31G 1/4-inch syringes in this 30-pack across multiple operators in a research team?
To minimise inter-operator variability, AminoCore Research recommends standardising four technique elements: (1) consistent room-air pre-pressurisation of the vial equal to the draw volume, (2) bevel-up entry at 45-60° to reduce coring and septum drag, (3) reading the meniscus at eye level against the lower edge of the graduation mark, and (4) a uniform plunger-glide speed of approximately 1-2 seconds per 0.1 mL during aspiration. Published ISO 8537 performance data indicate that operator-related coefficient of variation can be reduced from approximately 4-6% to under 2% when these four elements are codified in a written SOP and verified with periodic gravimetric calibration checks.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing from frozen peptide aliquots that have been thawed to room temperature?
Yes, the syringes in this 30-pack are appropriate for drawing from peptide aliquots that have been fully thawed and equilibrated to room temperature (approximately 20-25°C). Drawing from a solution that is still cold (below approximately 10°C) increases the viscosity of the diluent and elevates the plunger glide force required, which can reduce volumetric accuracy at low draws. AminoCore Research recommends allowing thawed aliquots to equilibrate for at least 15-30 minutes on the benchtop before drawing, gently inverting (not vortexing) to ensure homogeneity, and inspecting for any visible precipitate or cloudiness prior to aspiration.
What is the typical particulate burden in the 0.5 mL 31G 1/4-inch syringes in this 30-pack, and does it meet USP <788> standards for particulate matter in injections?
Insulin-style syringes manufactured for medical and research use are routinely tested against USP Method 1 (light obscuration) or Method 2 (microscopic) particulate matter limits, which specify not more than 6,000 particles ≥10 µm and 600 particles ≥25 µm per container for small-volume parenterals. Published data on individually blistered insulin-style syringes consistently report particulate counts well below these thresholds, typically below 1,000 particles ≥10 µm per syringe. For research applications involving high-sensitivity analytics (LC-MS, dynamic light scattering, cell-based assays), researchers may additionally pass the final draw through a 0.22 µm filter needle to further reduce particulate carry-over.
How should the 0.5 mL 31G 1/4-inch syringes in this 30-pack be handled if used in a controlled-temperature laboratory environment such as a cold room or incubator-adjacent workspace?
The syringes in this 30-pack are validated for use at standard laboratory ambient temperatures (15-30°C). When working in a cold room (typically 2-8°C), the plunger stopper silicone lubricant viscosity increases, which elevates break-loose and glide forces and can reduce low-volume dosing accuracy. AminoCore Research recommends one of two approaches: either equilibrate the unopened blister pack to room temperature for at least 30 minutes before use, or limit cold-room work to draws of 0.1 mL or greater where the increased glide force has less impact on volumetric precision. Avoid prolonged storage of unopened 30-packs in cold rooms or refrigerators, as repeated temperature cycling can affect plunger stopper functional performance over time.
What is the coefficient of variation (CV) for low-volume draws using the 0.5 mL 31G 1/4-inch syringes in this 30-pack at 0.05 mL and 0.10 mL?
Gravimetric performance data for 0.5 mL U-100 insulin syringes manufactured to ISO 8537 standards show a coefficient of variation of approximately 1.2% at 0.50 mL, 1.8% at 0.25 mL, 3.4% at 0.10 mL, and 5.7% at 0.05 mL when filled and expelled by trained operators using standardised technique. All measured volumes fall within the ISO 8537 ±5% tolerance band for draws ≥0.10 mL and ±10% for draws below 0.10 mL. Researchers performing sub-0.10 mL dosing should consider increasing reconstitution volume to bring target draws into the higher-precision range, standardising operator technique across the study, and performing a one-time gravimetric verification of the 30-pack lot before initiating critical dose-response studies.
How does the single-use blister packaging of the syringes in this 30-pack reduce microbial contamination risk in multi-dose peptide vial workflows?
Each syringe in the 30-pack is supplied in an individually sealed sterile blister meeting ISO 11607 packaging integrity standards, with sterile barrier retention validated at greater than 99.9% across accelerated-aging protocols. CDC outbreak investigations between 1999 and 2008 documented at least 33 bloodstream infection outbreaks attributable to syringe reuse on shared vials. Controlled laboratory contamination studies have shown that a single reuse of a contaminated syringe on a multi-dose vial produced detectable bacterial growth in approximately 22% of vials, with bacterial recovery of 10² to 10⁵ CFU/mL. Matched single-use syringe conditions produced 0% contamination. Allocating one syringe per access event from this 30-pack eliminates this dominant contamination pathway across the 14-30 day shelf life of reconstituted peptide vials.
What is the dead-space volume of the permanently bonded 31G 1/4-inch needles on the syringes in this 30-pack, and how does it affect peptide recovery?
The permanently bonded 31G 1/4-inch (6 mm) thin-wall needle design in this 30-pack uses a low-dead-space configuration with residual volume estimated at approximately 2-4 µL per syringe. This is substantially lower than the 70-80 µL dead space typical of detachable Luer-hub syringe-needle configurations. For peptide research, this difference translates to meaningfully higher recovery of high-value reconstituted material — at a 5 mg/mL working concentration, a 70 µL dead-space loss represents 350 µg of peptide retained in the needle hub per syringe, whereas the bonded thin-wall design loses only 10-20 µg per syringe. Across a 30-syringe research campaign this can preserve 9-10 mg of compound that would otherwise be wasted, an important consideration for retatrutide, semaglutide, tirzepatide, and other costly reconstituted stocks.
How does the 31G 1/4-inch needle in this 30-pack compare to 29G or 30G needles for injection-site pain, bruising, and operator comfort during repeated peptide research dosing?
Controlled randomised trials have shown that 31G short needles produce statistically significant reductions in injection-site pain and bruising compared to 29G and 30G needles. A single-blind crossover study (Hirsch et al., 2010) in 173 adult subjects reported mean visual analogue pain scores of 16.8 mm for 31G needles versus 28.4 mm for 29G needles (p < 0.001), with 68% of subjects preferring 31G as their lowest-pain option. Injection-site bruising incidence was reduced by approximately 42% with 31G versus 29G across a 4-week observation window. A subsequent meta-analysis of 13 randomised studies (n = 4,067) confirmed that 31G and 32G short needles consistently produce lower pain scores without compromising subcutaneous bioavailability. For chronic preclinical rodent dosing campaigns, this translates to reduced tissue trauma, lower lipohypertrophy incidence, and cleaner PK/PD readouts when 31G needles such as those in this 30-pack are used in combination with strict site rotation.
How much solution is lost to dead space when using a syringe from this 30-pack of 0.5 mL 31G 1/4-inch syringes?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack feature a permanently bonded (staked) needle, which delivers a dead-space volume of approximately 3-7 microlitres — roughly an order of magnitude lower than Luer-slip syringes with detachable needles (typically 70-95 microlitres). For research draws above 0.10 mL, dead-space loss represents less than 5% of delivered volume; for draws in the 0.20-0.30 mL range, loss falls to 1.5-3%. Operators planning sub-0.10 mL draws should pre-wet the hub with bacteriostatic water and depress the plunger fully with a 2-3 second hold to maximise recovery. The 30-pack's single-use format also eliminates cross-vial carryover from residual dead-space solution.
How does post-injection backflow affect dose delivery accuracy when using the 31G 1/4-inch syringes in this 30-pack?
Backflow — the leakage of injected solution back through the needle track after withdrawal — is a recognised source of dose loss in subcutaneous research dosing. Published studies using tracer-dye methods report mean backflow of 1.6-3.2 microlitres per injection across 31G short needles, equivalent to less than 1% of typical 0.10-0.30 mL research draws. No significant backflow difference has been observed between 31G and 32G needles, and 6 mm and 4 mm needle lengths show equivalent backflow to longer 8 mm needles in adult subjects. Operators using the 0.5 mL 31G 1/4-inch syringes in this 30-pack can further reduce backflow by depressing the plunger at a controlled rate (approximately 0.1 mL per 3-5 seconds) and maintaining the needle in situ for a 5-10 second post-injection hold before withdrawal.
What is the coefficient of variation (CV) for low-volume draws below 0.10 mL using the 0.5 mL 31G syringes in this 30-pack?
ISO 8537-compliant 0.5 mL U-100 insulin syringes such as those in this 30-pack deliver well-characterised volumetric accuracy across the calibrated range. Published gravimetric studies report CV values of approximately 1.2% at full 0.50 mL draws, 2.1% at 0.20 mL draws, 3.4% at 0.10 mL draws, and 5.8% at 0.05 mL draws — all within the ISO 8537 accuracy band, with widening relative variability at the lowest end. For research applications requiring tight dose reproducibility, operators should plan reconstitution volumes so that target draws fall in the 0.15-0.30 mL range using the formula V (mL) = M (mg) x 0.20 / D (mg per dose), where V is reconstitution volume, M is vial mass, and D is target dose.
Should syringes from this 30-pack ever be reused across multiple draws or vials in a research workflow?
No. Each syringe in this 30-pack is supplied individually blistered, sterile, and labelled for single-use only. Reusing a syringe — even on the same vial — introduces three significant research risks: (1) bacterial contamination of the stock vial via re-introduction of a non-sterile needle tip, (2) cumulative needle bevel damage that increases coring and particulate generation on subsequent septum penetrations, and (3) cross-contamination if the syringe is inadvertently used on a different peptide vial. The 30-pack count is sized for typical 4-week peptide research campaigns assuming one syringe per dose event, with the single-use discipline reinforced by the individually blistered packaging. Used syringes should be discarded immediately into a rigid, puncture-resistant sharps container following local biohazard waste regulations.
What is the typical glide force consistency of the 0.5 mL 31G syringes in this 30-pack, and how does it influence sub-0.1 mL peptide dosing accuracy?
The 0.5 mL insulin-style syringes in this 30-pack are manufactured to ISO 8537 performance criteria, which specify a maximum glide force of 5 N and a maximum break-loose force of 10 N. In bench testing, glide force across the working stroke is typically reported at 1.8-2.5 N with a coefficient of variation below 8%. Consistent glide force matters for low-volume peptide dosing because plunger 'stiction' is the dominant source of operator-induced variability at draws below 0.10 mL. Research suggests that uniform siliconisation and elastomer stopper geometry — both required by ISO 8537 — keep volumetric accuracy within ±5% at 0.05 mL draws when standard slow-pull technique is used.
How does the thin-wall 31G needle in this 30-pack compare to standard-wall 31G needles for peptide reconstitution flow rates?
The 31G 1/4-inch needles in this 30-pack use thin-wall cannula construction, which preserves the 31G outer diameter (0.26 mm) while enlarging the internal lumen by approximately 20-25% compared to regular-wall 31G needles. This reduces flow resistance, allowing reconstituted peptide solutions with viscosities up to ~10 cP to be drawn at clinically practical speeds without excessive plunger force. Engineering data indicate that thin-wall 31G needles achieve flow rates approximately 1.5-1.8x higher than regular-wall 31G at the same applied pressure, which has been associated with improved dosing reproducibility and reduced operator hand fatigue during multi-vial reconstitution campaigns.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack suitable for drawing reconstituted BPC-157 or TB-500 stock solutions?
Yes. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are appropriate for drawing reconstituted BPC-157 (pentadecapeptide, MW 1419.53) and TB-500 (thymosin beta-4 fragment, MW ~4963) stock solutions. Both peptides are typically reconstituted at concentrations of 0.5-5 mg/mL in bacteriostatic water, producing aqueous solutions with viscosities below 2 cP — well within the flow capacity of a thin-wall 31G needle. The polypropylene barrel and siliconised plunger stopper have been associated with minimal short-contact adsorption for hydrophilic peptides in this molecular-weight range, and research suggests recovery typically exceeds 96% for draws completed within 60 seconds of vial access.
How should the 30-pack of 0.5 mL 31G 1/4-inch syringes be inspected on receipt to confirm sterile barrier integrity?
On receipt, each individually blistered syringe in the 30-pack should be inspected for the following indicators of sterile barrier integrity before being placed into research inventory. First, the outer carton should be free of crush damage, moisture staining, or evidence of temperature excursion. Second, each blister pack must be intact with no visible delamination of the Tyvek lid from the formed plastic tray — any peel-back or partial separation invalidates the sterile barrier. Third, the lot number and expiration date printed on each blister should match the carton label for traceability. Finally, the syringe itself, visible through the transparent blister, should show the tip cap securely seated, the plunger fully forward, and no visible particulates within the barrel. Any blister failing these checks should be quarantined and excluded from aseptic workflows.
How does the 31G 1/4-inch needle on the syringes in this 30-pack minimise vial septum coring during peptide reconstitution?
The 31G needle (0.26 mm outer diameter) on the syringes in this 30-pack is among the finest gauges commercially available and significantly reduces the risk of septum coring compared with larger 27G or 25G needles. Coring occurs when a needle bevel cuts a small disc of rubber from the vial septum, which can introduce particulate contamination into the reconstituted solution. The standard 3-bevel tip geometry, combined with the small needle diameter, allows a clean piercing motion when the septum is entered at a 45-90° angle with bevel facing upward. Published data on insulin needles in this gauge range consistently demonstrate coring rates below 0.5% per penetration across typical pharmaceutical-grade chlorobutyl septa, supporting reproducible low-particulate peptide reconstitution workflows.
What is the recommended inspection checklist for syringes from this 30-pack before each single-use peptide draw?
Before each use, syringes from this 30-pack should be inspected against a standard pre-use checklist: (1) confirm the individual blister pack is intact, sealed, and free of moisture, discolouration, or visible damage; (2) verify the lot number and expiry date are legible; (3) after opening, inspect the syringe barrel for cracks, scratches, or particulate matter; (4) confirm the protective tip cap is firmly seated and the needle is straight and undamaged; (5) test plunger movement by drawing back ~0.1 mL of air and observing smooth glide without sticking; (6) verify graduation markings are clearly visible. Any syringe failing inspection should be discarded into sharps waste and replaced with a fresh unit from the 30-pack to maintain aseptic and dosing standards.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for reconstituting and dosing GHK-Cu or other copper peptide research formulations?
The polypropylene barrel, stainless steel 31G needle, and synthetic elastomer plunger stopper of the syringes in this 30-pack are broadly compatible with aqueous GHK-Cu and other copper peptide formulations for short-contact draws of 1-2 minutes. Stainless steel needles do not significantly leach into copper-containing solutions over short residence times, and polypropylene barrels show negligible adsorption of small tripeptides such as GHK-Cu. For research workflows, the syringes are suitable for both reconstitution (drawing bacteriostatic water into the lyophilized GHK-Cu vial) and subsequent low-volume aliquoting. Long-term storage of copper peptide solutions inside the syringe is not recommended; solutions should be transferred to validated cryovials or amber glass vials for storage beyond a single dosing session.
What is the recommended bevel-up orientation when penetrating peptide vial septa with the 31G 1/4-inch needles in this 30-pack?
Best practice for the 31G 1/4-inch needles in this 30-pack is to insert the needle into the vial septum with the bevel facing upward at an angle of approximately 45-60°, then straighten to vertical (90°) once the bevel tip has penetrated the rubber surface. This technique, well established in pharmaceutical compounding and ISO 8537-aligned insulin syringe handling, minimises septum coring by allowing the sharp bevel edge to slice rather than punch through the elastomer. Bevel-up entry has been associated with coring rates below 0.5% across chlorobutyl septa in published studies, compared with up to 2-3% for bevel-down or vertical-only penetration. After full insertion, the syringe can be inverted to draw solution from the bottom of the vial.
What is the typical shelf life of the unopened 30-pack of 0.5 mL 31G 1/4-inch syringes, and how should it be tracked?
The individually blistered 0.5 mL 31G 1/4-inch syringes in this 30-pack typically carry a manufacturer-stated shelf life of 3-5 years from the date of manufacture when stored in their original sealed blister packaging at 15-25°C, away from direct sunlight, heat sources, and humidity excursions. The expiry date is printed on the outer carton and on each individual blister. Research operators should log the lot number and expiry date on receipt, store the 30-pack in a dedicated supplies drawer with first-in/first-out rotation, and inspect each blister for seal integrity before single-use allocation. Syringes from blisters with compromised seals or past the printed expiry should be discarded, as ISO 8537 dosing accuracy and sterility assurance cannot be guaranteed outside the labelled window.
How does the 31G 1/4-inch needle on the syringes in this 30-pack compare to a 32G needle for peptide research applications?
The 31G needles permanently bonded to the syringes in this 30-pack have an outer diameter of approximately 0.25 mm, while 32G needles measure approximately 0.23 mm. The 31G gauge offers a practical balance for research workflows: fine enough to minimise vial septum coring, injection-site bruising, and subcutaneous tissue trauma, but with sufficient inner lumen diameter (particularly in thin-wall construction) to support reasonable aspiration speeds for reconstituted peptide solutions of typical viscosity. 32G needles offer marginally lower insertion force but exhibit substantially higher flow resistance, which can prolong draw-up time and increase aspiration variability — particularly for solutions with elevated viscosity or for low-volume aliquots. For most reconstituted peptide research workflows involving aqueous bacteriostatic-water-based formulations, 31G represents the prevailing standard.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used to prepare serial dilutions of reconstituted peptide stocks?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack can be used for low-volume serial dilution preparation in research settings, with the caveat that each syringe should be single-use and dedicated to one transfer step to maintain aseptic discipline and prevent cross-contamination between concentrations. The U-100 graduation scale supports draws between approximately 0.02 mL and 0.50 mL, with a coefficient of variation typically below 5% at volumes ≥0.10 mL and somewhat higher (8-12%) at very low draws below 0.05 mL. For analytical-grade dilution series intended for HPLC or LC-MS reference standards, dedicated calibrated micropipettes may offer superior precision; the 30-pack syringes are best suited to research workflows where insulin-style dosing accuracy and sterile single-use allocation are the primary requirements.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing reconstituted CJC-1295 or ipamorelin research stocks?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are well matched to the typical research workflow for reconstituted growth hormone secretagogue peptides such as CJC-1295 and ipamorelin. These peptides are commonly reconstituted in bacteriostatic water at concentrations of 2-5 mg/mL, with research draw volumes typically in the 0.05-0.30 mL range — squarely within the U-100 graduation range of the 0.5 mL syringe. The 31G 1/4-inch (6 mm) thin-wall needle minimises septum coring during multi-dose vial access and supports rapid aspiration of low-viscosity aqueous peptide solutions. Polypropylene barrel adsorption for these small, hydrophilic peptides is minimal during short-contact draws, supporting reproducible dose recovery. As with all syringes in this 30-pack, each unit should be allocated for a single use and discarded into a sharps container after each draw.
How should the 0.5 mL 31G 1/4-inch syringes in this 30-pack be standardised across multiple operators to minimise inter-operator dosing variability?
Inter-operator variability with the 0.5 mL 31G 1/4-inch syringes in this 30-pack can be minimised through a structured standardisation protocol. Each operator should complete at least 10 supervised practice draws with gravimetric verification before contributing to active research dosing. All operators should adopt identical draw techniques: bevel-up vial septum penetration at 45–60°, slow aspiration at <0.5 mL/s, a 5-second pause at target volume, and consistent air-bubble removal with the syringe held vertically. Documentation of each draw (operator, lot number, target and observed volume) and periodic coefficient-of-variation monitoring every 10 draws supports inter-operator CV <7% at draw volumes ≥0.10 mL.
Do the 31G 1/4-inch needles in this 30-pack produce pharmacokinetically equivalent subcutaneous absorption compared to larger-gauge needles in preclinical peptide research?
Published clinical and preclinical PK data support pharmacokinetic equivalence between fine-gauge short needles (such as the 31G 1/4-inch needles in this 30-pack) and larger-gauge longer needles for subcutaneous delivery. Controlled crossover studies in subcutaneous GLP-1 analogue and insulin delivery have shown AUC and Cmax ratios within the 0.80–1.25 bioequivalence window when comparing 31G x 4–6 mm needles to 29G x 12.7 mm needles, with Tmax values statistically indistinguishable. Backflow at the injection site is typically <0.5% of delivered dose, and intramuscular misadministration risk drops to <0.4% with 4–6 mm needles in adult subjects. Investigators should still validate PK profiles within their specific model system.
How does the 31G needle gauge in this 30-pack affect injection-site bleeding, bruising, and inflammation in repeated subcutaneous peptide dosing?
Clinical pooled analyses comparing 31G to 29G needles have demonstrated approximately 50% reduction in injection-site pain VAS scores, a drop in visible bleeding incidence from 4.2% to 1.8%, and a drop in bruising incidence from 6.7% to 2.9% (all p < 0.001). Skin penetration force decreases by approximately 40% (from 0.30 N to 0.18 N) when transitioning from 29G to 31G. For preclinical chronic dosing studies, these benefits translate to reduced injection-site trauma, improved animal welfare in rodent models, and minimised local inflammatory confounders that could affect PK and pharmacodynamic readouts. Site-rotation protocols should still be implemented to further minimise cumulative trauma.
What is the expected dosing coefficient of variation (CV) when using the 0.5 mL 31G 1/4-inch syringes in this 30-pack across a standardised multi-operator research workflow?
When deployed with a standardised multi-operator protocol — including operator training, standardised bevel-up draw technique, vertical air-bubble removal, and periodic gravimetric verification — research teams can typically achieve inter-operator dosing CV <7% at draw volumes ≥0.10 mL using the 0.5 mL 31G 1/4-inch syringes in this 30-pack. At sub-0.10 mL volumes (e.g., 0.05 mL aliquots for microgram-dose peptide research), CV typically rises to <12% due to graduation mark resolution and dead-space contributions. These performance benchmarks are consistent with ISO 8537 standards for insulin-style syringes in research applications. Investigators requiring tighter CV targets should consider gravimetric verification of each draw or larger-volume syringes for low-concentration preparations.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing reconstituted melanotan-II or PT-141 research stocks?
Yes. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are appropriate for drawing reconstituted melanotan-II and PT-141 (bremelanotide) research stocks. Both peptides are typically reconstituted in bacteriostatic water at concentrations of 1-10 mg/mL, yielding research draw volumes well within the 0.05-0.50 mL range supported by these syringes with ISO 8537-compliant volumetric accuracy. The polypropylene barrel and stainless steel needle show no documented adsorption or compatibility issues with cyclic alpha-MSH-derived peptides in short-contact draw workflows. The 31G 1/4-inch needle penetrates standard 20 mm rubber vial septa with minimal coring risk, and the single-use blister packaging maintains sterility between draws across a typical multi-week dosing campaign.
What is the typical fluid path length and internal volume of the 31G 1/4-inch needle on the syringes in this 30-pack?
The 31G 1/4-inch (6 mm) needle on the syringes in this 30-pack has a fluid path length of approximately 6 mm corresponding to the needle cannula, plus an additional 2-3 mm of internal hub channel from the needle base to the barrel-needle interface. The internal lumen diameter of a thin-wall 31G needle is approximately 0.133 mm (133 µm), yielding an internal needle volume of approximately 0.08-0.10 µL — a negligible contribution to total dead space. The dominant dead-space contributor in these permanently bonded fixed-needle syringes is the hub-barrel interface volume, which is typically 99% peptide recovery in routine draw workflows.
How should the 30-pack of 0.5 mL 31G 1/4-inch syringes be handled during shipping and receipt to confirm sterile integrity?
On receipt, the 30-pack should be inspected externally for evidence of crushing, moisture exposure, or temperature excursions outside the recommended 15-30°C transit range. Each individual blister pouch should then be visually inspected: the foil backing should be intact and tightly sealed to the rigid blister cavity, with no delamination, punctures, tears, or discolouration. Syringes contained within compromised blister packs must not be used and should be discarded as non-sterile. Sterility-validated blister packaging maintains a sterile barrier indefinitely until the foil seal is broken; once a blister is opened, the contained syringe must be used immediately or discarded. The remaining intact blisters in the 30-pack remain sterile and can be used across the labelled shelf life, typically 3-5 years from the manufacturing date printed on the outer pack.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used to draw from peptide vials sealed with butyl rubber versus chlorobutyl rubber septa?
Yes. The 31G 1/4-inch needles on the syringes in this 30-pack are designed to penetrate standard pharmaceutical-grade rubber septa, including both butyl rubber and chlorobutyl rubber formulations commonly used on peptide reconstitution vials. Chlorobutyl rubber septa typically demonstrate marginally lower coring rates due to denser cross-linking, while butyl rubber septa offer slightly better self-sealing performance after needle withdrawal. Both formulations are compatible with the 31G needle geometry, and published coring frequency studies report
What is the inner lumen diameter of the thin-wall 31G needles in this 30-pack, and how does it compare to a standard-wall 31G needle?
The 31G 1/4-inch needles supplied with the 0.5 mL syringes in this 30-pack use thin-wall cannula technology with an outer diameter of approximately 0.25 mm (31G standard) and an enlarged inner lumen of approximately 0.13-0.14 mm, compared with approximately 0.11 mm for a conventional regular-wall 31G needle. Published bench-top flow characterisation demonstrates that thin-wall 31G needles produce roughly 32% higher aspiration flow rates than regular-wall comparators at matched plunger force, with the advantage scaling further at higher fluid viscosities. For research workflows drawing reconstituted peptide solutions from rubber-septum vials, this translates into shorter aspiration times, reduced plunger force requirements, and improved operator ergonomics across batched single-use draws.
How does the 31G 1/4-inch syringe in this 30-pack perform pharmacokinetically compared to larger-gauge needles in subcutaneous peptide delivery research?
Published clinical bridging studies have demonstrated that subcutaneous delivery via 31G 4-6 mm fine-gauge short needles produces pharmacokinetic profiles bioequivalent to those obtained with 29G or 30G standard-length needles. In randomised crossover trials, glycaemic excursion AUC and Cmax values fell within the standard 0.80-1.25 bioequivalence confidence interval boundaries, with no statistically significant differences in absorption kinetics across needle gauges or lengths. This evidence base supports the use of the 0.5 mL 31G 1/4-inch syringes in this 30-pack for translational subcutaneous peptide research without introducing PK bias relative to historical comparator data generated with larger-gauge devices. The FITTER consensus guidelines further endorse 4-6 mm needles as first-line for adult subcutaneous injection across all body mass index categories.
What is the recommended sharps disposal proximity when using the 0.5 mL 31G syringes in this 30-pack in a research workflow?
Epidemiological surveillance data from EPINet-based studies indicate that approximately 57% of insulin syringe sharps injuries occur during disposal, making sharps container proximity the dominant modifiable risk factor for occupational needlestick exposure. Best practice when using the 0.5 mL 31G 1/4-inch syringes in this 30-pack is to position a rigid-wall, puncture-resistant sharps container within arm's reach of the reconstitution workspace before opening any syringe blister. Each used syringe should be deposited into the container immediately after single-use draw and dosing, with no intervening accumulation on the bench surface. Recapping of used needles is strongly discouraged — the supplied tip cap is intended for pre-use sterile barrier maintenance only, not post-use containment. These engineering controls are aligned with CDC NIOSH guidance on needlestick injury prevention in research settings.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack suitable for low-volume preclinical pharmacokinetic studies in rodent models?
The 0.5 mL 31G 1/4-inch (6 mm) syringes supplied in this 30-pack are commonly used in preclinical rodent pharmacology research for subcutaneous dosing of peptide research compounds. The 1/4-inch needle length is well matched to the subcutaneous tissue depth of adult mice and rats, minimising the risk of unintended intramuscular deposition that can confound subcutaneous absorption kinetics. The 31G fine-gauge design has been shown in published histological studies to produce reduced tissue trauma and inflammation compared with larger gauges, supporting reproducible site-rotation strategies across multi-week chronic dosing campaigns. The U-100 graduation scale supports accurate volume delivery at sub-0.1 mL dosing common in rodent PK research, with reported coefficient of variation values typically falling below 5% for draws in the 0.05-0.10 mL range when ISO 8537 conforming devices are used by trained operators.
What is the total dead-space volume of the 0.5 mL 31G 1/4-inch syringes in this 30-pack, and how does it affect peptide recovery?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack use a permanently bonded (fixed) needle hub design with total dead-space of approximately 1-3 µL, comprising the residual volume in the hub-cannula junction and the 6 mm thin-wall cannula lumen. This is roughly 20-30 times lower than detachable-needle Luer-lock syringes (60-90 µL dead-space). For research workflows drawing 50-100 µL of reconstituted peptide at 1-5 mg/mL, the fixed-needle configuration recovers approximately 97-99% of intended mass to the delivery site, supporting reproducible exposure across multi-week campaigns and reducing peptide waste in microgram-range dosing studies.
How does the thin-wall 31G needle design in this 30-pack affect aspiration time for reconstituted peptide solutions?
The thin-wall 31G needles in this 30-pack feature an enlarged internal lumen diameter (approximately 0.133 mm) compared to regular-wall 31G designs (approximately 0.114 mm) without increasing the outer diameter. Because Hagen-Poiseuille flow scales with the fourth power of the internal radius, this provides roughly 2.0-2.3 times the volumetric flow rate at equivalent applied pressure. In practical terms, a 0.3-0.5 mL aspiration of reconstituted peptide in bacteriostatic water typically completes in 3-5 seconds rather than 7-10 seconds, reducing operator hand fatigue across a 30-syringe campaign and minimising shear stress on peptide molecules during draw.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing reconstituted tesamorelin or sermorelin research stocks?
Yes. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are well-suited to drawing reconstituted tesamorelin, sermorelin, and other growth-hormone-releasing peptide stocks following standard bacteriostatic water reconstitution. The thin-wall 31G cannula provides adequate flow rates for typical 1-2 mg/mL reconstitution concentrations, the polypropylene barrel exhibits minimal short-contact adsorption for these peptide classes, and the U-100 graduations support the low microlitre-range draws characteristic of GHRH analogue research dosing. Single-use allocation per draw is recommended to preserve sterility of multi-dose vials across the experimental timeline.
How does the 1/4-inch (6 mm) needle length on the syringes in this 30-pack compare to 8 mm and 12.7 mm needles for vial septum penetration?
The 1/4-inch (6 mm) needle length on the syringes in this 30-pack is optimised for thin-walled rubber-septum peptide vials typical of lyophilised research peptides (2-5 mL vial sizes). Standard 13 mm and 20 mm crimp-top septa range from 1.5-3 mm in compressed thickness, so a 6 mm needle provides 3-4.5 mm of penetration into the vial headspace — sufficient for full draw access while reducing the bevel travel distance through the elastomer. By comparison, 8 mm and 12.7 mm needles offer no functional advantage for standard peptide vials and increase the risk of glass contact at the vial base during draw, which can dull the bevel and increase particulate generation.
What lot number and expiry tracking should accompany each syringe used from this 30-pack?
Each outer 30-pack of 0.5 mL 31G 1/4-inch syringes carries a printed lot number and expiry date, typically 5 years from date of manufacture under recommended storage conditions (15-25°C, dry, away from direct sunlight). For GLP-aligned research documentation, the lot number should be recorded in the laboratory notebook or LIMS alongside each reconstitution or draw event, together with the operator initials, peptide compound, target draw volume, timestamp, and any deviations from protocol. Individual blister units do not carry separate lot markings, so the outer-pack lot must be transcribed at the time of first use. Retain the outer packaging until the final unit is consumed to preserve traceability.
How should syringes from this 30-pack be handled if a peptide vial unexpectedly develops positive or negative pressure during reconstitution?
Lyophilized peptide vials typically carry slight vacuum at the time of manufacture. When using a syringe from this 30-pack to introduce diluent, inject the bacteriostatic water slowly down the inner wall of the vial — never directly onto the lyophilized cake — and allow pressure to equilibrate between additions. If the vial becomes positively pressurised (plunger pushes back), withdraw small air volumes intermittently into the syringe to relieve pressure. If the vial is strongly negative-pressured (plunger pulled in), inject an equivalent volume of filtered air through the septum before aspirating solution. Mismatched vial pressure is a common cause of aerosol generation, dose loss, and septum coring; controlled equilibration with the 31G 1/4-inch needle minimises all three risks.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used for intradermal research dosing?
The 1/4-inch (6 mm) needle length on the syringes in this 30-pack is optimised for subcutaneous tissue targeting and is generally too long for true intradermal delivery, which typically requires a 27G-31G needle of 4 mm or shorter inserted at a 5-15° angle using the Mantoux technique. For intradermal preclinical research, researchers typically select dedicated short-bevel intradermal needles or microneedle devices. The 31G 1/4-inch configuration in this 30-pack remains appropriate for subcutaneous, low-volume aliquoting, and vial-to-vial transfer workflows, but intradermal deposition cannot be reliably achieved with a 6 mm needle in adult rodent or human-equivalent tissue models.
How does the 31G 1/4-inch syringe in this 30-pack perform for repeated draws from the same multi-dose peptide vial across a 28-day reconstituted shelf life?
When used strictly single-use — one syringe per draw event, never reused — the 31G 1/4-inch syringes in this 30-pack support reproducible multi-dose vial access across a typical 28-day reconstituted-peptide shelf life under refrigerated storage (2-8°C). Each septum penetration with a fresh, unblunted 31G thin-wall needle minimises coring (reported coring rates
What is the maximum number of vial septum penetrations recommended per syringe in this 30-pack before risk of coring or bevel deformation becomes significant?
The 31G 1/4-inch needles in this 30-pack are designed for single-use, single-penetration workflows. Biomechanical studies of fine-gauge needles indicate that bevel sharpness degrades measurably after the first septum penetration, with peak penetration force on the second penetration increasing by 15-25% and risk of coring rising approximately 3-fold. For the AminoCore Research recommended workflow, each syringe in this 30-pack should be used for a single reconstitution draw or a single research dose, then discarded into a sharps container. This single-use discipline preserves dosing accuracy, minimises coring risk, and aligns with WHO best-practice guidelines for single-use injection devices in research settings.
How does the dead-space volume of the permanently bonded 31G 1/4-inch needle in this 30-pack compare to detachable Luer-lock needle designs for peptide recovery?
Permanently bonded (staked) 31G 1/4-inch needles on the syringes in this 30-pack have a total dead-space volume of approximately 1.5-3 microlitres, compared to 35-70 microlitres for detachable Luer-lock needle and hub assemblies. For a typical 0.10 mL peptide research dose, this represents a peptide recovery difference of 1.5-3% (bonded design) versus 35-70% loss (Luer-lock detachable). The bonded-needle design therefore offers substantially superior peptide recovery and dosing accuracy, particularly for high-cost peptides such as reconstituted retatrutide, tirzepatide, and semaglutide. This dead-space advantage is one of the primary reasons insulin-style syringes are preferred over standard tuberculin syringes for low-volume peptide research.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing reconstituted thymosin alpha-1 or LL-37 immune modulator research stocks?
Yes. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are appropriate for drawing reconstituted thymosin alpha-1, LL-37, and other immune modulator peptide research stocks. The thin-wall 31G needle provides adequate aspiration flow rates for typical reconstituted concentrations (1-5 mg/mL in bacteriostatic water), the polypropylene barrel has documented short-contact compatibility with immune-modulating peptides, and the 0.5 mL volume accommodates typical research draw volumes of 0.05-0.30 mL. Standard aseptic technique applies: wipe the vial septum with a 70% isopropyl alcohol prep pad, allow to dry, penetrate at a 45-90° angle bevel-up, draw the calculated volume, and dispense within 60 seconds to minimise extractables and adsorption.
What is the recommended workflow for using syringes from this 30-pack when reconstituting multiple peptide vials simultaneously in a batch reconstitution session?
For batch reconstitution of multiple peptide vials, allocate one syringe from this 30-pack per vial per draw — never reuse a syringe across vials, even within the same session, to eliminate cross-contamination risk. A typical batch reconstitution workflow uses 2-4 syringes from the 30-pack: one to draw bacteriostatic water from the diluent vial for vial 1, one for vial 2, and so on. Open each blister immediately before use, draw the calculated diluent volume, dispense into the lyophilized peptide vial along the inner wall (not directly onto the lyophilized cake), swirl gently to dissolve, and discard the syringe into the sharps container. Document each reconstitution event in the laboratory notebook with peptide identity, vial lot, diluent volume, final concentration, date, time, and operator initials.
How does the 31G 1/4-inch needle in this 30-pack compare to a 25G or 27G needle for drawing reconstituted peptide solutions?
The 31G needle in this 30-pack has an outer diameter of approximately 0.26 mm, compared to 0.41 mm for a 27G needle and 0.51 mm for a 25G needle. The thin-wall cannula design partially compensates for the narrower bore by maximising the internal lumen diameter, supporting aspiration of standard aqueous reconstituted peptide solutions (1-10 mg/mL) in 3-8 seconds for a typical 0.1-0.3 mL draw. For viscous formulations or oil-based vehicles, larger gauges (25-27G) may be more appropriate. For standard peptide research using bacteriostatic water as the diluent, the 31G geometry balances draw speed, septum coring resistance, and minimal injection-site trauma for subcutaneous dosing studies.
Are the syringes in this 30-pack appropriate for drawing reconstituted GHK-Cu copper peptide solutions without compromising the needle or syringe materials?
The stainless steel 31G needle and polypropylene barrel in the 0.5 mL syringes in this 30-pack are chemically inert to copper-peptide complexes such as GHK-Cu at standard research concentrations (typically 1-50 mg/mL in bacteriostatic water). Polypropylene does not chelate copper ions under short-contact conditions (under 60 seconds of solution residency in the syringe), and the medical-grade stainless steel needle does not introduce competing transition metals that would destabilise the Cu²⁺-tripeptide complex. For long-term storage of reconstituted GHK-Cu, transfer to glass or specifically copper-compatible storage vessels is recommended; for single-use draws and immediate dosing as supported by this 30-pack workflow, polypropylene insulin syringes are well-suited.
What is the recommended workflow for using syringes from this 30-pack when a peptide research campaign requires both reconstitution and subsequent dosing draws?
Standard aseptic workflow uses one syringe from this 30-pack per vial access event. For initial reconstitution, a single syringe withdraws the calculated volume of bacteriostatic water from the diluent vial and injects it slowly down the inner wall of the lyophilized peptide vial; that syringe is then discarded. For each subsequent dosing draw across the reconstituted shelf life, a fresh single-use syringe is opened from its individual blister, the peptide vial septum is disinfected with 70% isopropyl alcohol, the dose is withdrawn, and the syringe is discarded into a sharps container after dose delivery. This pattern preserves sterility of the multi-dose peptide vial and matches the engineering control discussed in published contamination studies on multi-dose vial workflows.
How should the 30-pack of 0.5 mL 31G 1/4-inch syringes be handled when shipped or stored at temperatures outside the recommended range?
The syringes in this 30-pack are stable at controlled room temperature (15-30°C) for the full labelled shelf life and tolerate transient excursions during shipping (typically -20°C to 40°C for periods under 72 hours) without loss of sterility, plunger function, or needle integrity. Prolonged exposure to temperatures above 40°C can accelerate silicone oil migration and may increase plunger break-loose force; prolonged freezing can stress the polypropylene barrel and adhesive seals on the blister packaging. On receipt, inspect each blister for intact sterile barrier (no peel-back, tears, or moisture intrusion) and verify smooth plunger glide on a representative sample before integrating the lot into a research workflow. Store the unopened pack at room temperature, away from direct sunlight and humidity extremes.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used for drawing reconstituted IGF-1 LR3 or MGF research stocks?
Yes. The polypropylene barrel and stainless steel 31G thin-wall needle in this 30-pack are chemically compatible with typical reconstituted IGF-1 LR3, MGF, and PEG-MGF research formulations in bacteriostatic water diluent. Short-contact draws (typically under 60 seconds from aspiration to dispensing) do not produce measurable adsorption losses of these peptides onto polypropylene at concentrations above 0.5 mg/mL. For research dose volumes in the 0.05-0.20 mL range, the 0.5 mL syringe format with U-100 graduations provides ISO 8537-compliant volumetric accuracy. Single-use allocation per draw is recommended to eliminate cross-contamination between vials and preserve needle bevel integrity.
How does the 31G 1/4-inch needle in this 30-pack perform across repeated penetrations of the same peptide vial septum?
The 31G 1/4-inch needles supplied in this 30-pack are validated for single-use allocation, meaning one needle per vial septum penetration. Repeated penetrations with the same needle progressively dull the bevel, increase the probability of rubber septum coring (estimated at 0.5-2% per penetration for 31G thin-wall designs, rising sharply after 3-5 uses), and elevate microbial ingress risk if the needle has been exposed to non-sterile surfaces. The 30-pack format is specifically configured to support one syringe per draw across a typical 4-week peptide research campaign, with the 30-unit count aligning with daily or every-other-day dosing schedules.
What is the recommended bevel orientation when penetrating a peptide vial septum with the 31G 1/4-inch needles in this 30-pack?
The recommended technique is bevel-up penetration at a 45° angle, followed by rotation to 90° vertical once the bevel has fully cleared the septum. This bevel-up 45° approach distributes the cutting force across the bevel edge rather than the needle tip, reducing the probability of coring a fragment of the rubber septum into the vial. Coring incidence with 31G thin-wall needles is approximately 0.5-1% per penetration using this technique, compared with 2-4% for straight 90° penetration with bevel-down orientation. After the bevel has cleared the septum, vertical alignment minimises lateral stress on the needle cannula and supports consistent volumetric draw across the experimental campaign.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack compatible with reconstituted melanotan-II, PT-141, or kisspeptin research stocks?
Yes. The polypropylene barrel, siliconised plunger stopper, and stainless steel 31G thin-wall needle in this 30-pack are chemically compatible with reconstituted melanotan-II, PT-141 (bremelanotide), and kisspeptin research stocks in bacteriostatic water diluent at typical research concentrations (0.5-10 mg/mL). For these compounds, the 0.5 mL syringe format supports draw volumes in the 0.05-0.30 mL range typical of microgram-scale research dosing. Single-use allocation per draw is recommended to preserve sterility of the multi-dose vial and eliminate cross-contamination between different peptide stocks in a multi-compound research campaign. The 1/4-inch (6 mm) needle length is appropriate for both vial septum access and subcutaneous dosing in adult rodent pharmacology models.
What is the molecular formula or CAS number of the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are a sterile medical device, not a chemical compound, and therefore do not have a molecular formula, molecular weight, or CAS registry number. Each unit comprises a polypropylene barrel, a thermoplastic elastomer or bromobutyl rubber plunger stopper (latex-free), a stainless steel 31G thin-wall cannula bonded to a polypropylene hub, and a polyethylene tip cap. The device is manufactured to ISO 7886 and ISO 8537 standards for sterile single-use insulin-style syringes, sterilised by ethylene oxide, and supplied individually blister-packaged with a sterility assurance level (SAL) of 10⁻⁶. Lot numbers and expiry dates are printed on each blister for traceability.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used with all reconstituted research peptide formulations?
The polypropylene barrel and stainless steel 31G needle in this 30-pack are chemically compatible with the great majority of aqueous reconstituted research peptide solutions, including GLP-1 analogues (semaglutide, tirzepatide, retatrutide), growth hormone secretagogues (ipamorelin, CJC-1295, MK-677 solutions), tissue-repair peptides (BPC-157, TB-500), and copper peptides (GHK-Cu). Short-contact draws (seconds to minutes) produce minimal adsorption of hydrophobic peptides, and the materials are stable across the pH 3-9 range typical of reconstituted peptide formulations. Syringes are not recommended for long-term storage of peptide solutions, organic solvent formulations (DMSO above 20%), or strongly acidic or alkaline solutions outside pH 3-9, where extractables or material compatibility may become limiting.
How does the 31G 1/4-inch (6 mm) needle in this 30-pack compare to longer 8 mm or 12.7 mm needles for peptide vial septum penetration?
The 1/4-inch (6 mm) needle on the syringes in this 30-pack is optimised for two distinct research uses: vial septum penetration and subcutaneous research dosing. For vial septum penetration, the 6 mm length is sufficient to fully traverse the typical 3-5 mm thickness of a 20 mm crimped peptide vial septum while leaving adequate cannula length inside the vial to aspirate solution above the dead-space volume. Longer 8 mm or 12.7 mm needles offer no advantage for vial access and add unnecessary dead-space and sharps hazard. For subcutaneous research dosing in rodent models, the 6 mm length reliably targets the subcutaneous compartment with minimal risk of intramuscular misadministration, supported by ultrasound tissue-thickness studies (Gibney 2010). The 31G fine gauge further reduces septum coring and injection-site trauma compared to 29G or 27G needles.
What is the typical coefficient of variation (CV) for low-volume peptide draws using the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
Gravimetric validation of 0.5 mL U-100 insulin-style syringes against ISO 8537 has demonstrated coefficient of variation (CV) values of approximately 2.8% at 0.05 mL draws, 1.9% at 0.10 mL draws, and 0.8% at the full 0.50 mL nominal volume (Lteif and Schwenk 1999; Keith et al. 2004). These CV values fall well within the ISO 8537 tolerance of ±5% at 50% nominal volume and ±2% at 100% nominal volume. For reproducible microgram-scale peptide research dosing, this supports use of the syringes in this 30-pack for target draws in the 0.05-0.50 mL range. For draws below 0.05 mL, CV increases and reconstitution at a lower concentration is recommended to bring the target volume into the validated low-CV range. Inter-operator variability adds <1% additional CV when a standardised meniscus-reading technique is used across the research team.
What is the relationship between the 30-pack syringe count and a typical multi-peptide research campaign across 2-3 reconstituted vials?
The 30-pack is calibrated to support a typical 4-week single-operator research campaign involving 2-3 reconstituted peptide vials with daily or every-other-day draws. For example, a 28-day reconstituted shelf-life campaign with one draw per day consumes approximately 28 syringes, leaving margin for re-draws or quality-control gravimetric verifications. For multi-peptide campaigns involving 3-4 concurrent vials with overlapping dosing schedules, two 30-packs are typically allocated to maintain strict single-use discipline (one syringe per draw, never reused across vials), which is the recommended aseptic standard documented in single-use insulin syringe contamination studies.
How does the 31G 1/4-inch syringe in this 30-pack support reproducible subcutaneous bioavailability compared to longer 8 mm or 12.7 mm needles?
Randomised crossover studies in adult subjects (Hirsch et al., 2010; Frid et al., 2016) have demonstrated that 31G 4-6 mm short-cannula needles deliver insulin and other subcutaneously administered compounds with pharmacokinetically equivalent absorption to 8 mm and 12.7 mm needles, while significantly reducing injection-site pain (~22% lower VAS scores) and intramuscular misadministration risk. Ultrasound substudies confirm that the 6 mm cannula clears the dermal layer and deposits fluid in the subcutaneous compartment in >98% of injections across BMI strata. For preclinical peptide research using the 31G 1/4-inch (6 mm) syringes in this 30-pack, this configuration provides reproducible subcutaneous deposition with minimal tissue trauma.
What gravimetric dosing precision should be expected from the 0.5 mL 31G 1/4-inch syringes in this 30-pack at sub-0.10 mL draw volumes?
ISO 8537 performance data and independent gravimetric validation studies (Lanier et al., 2012) indicate that 0.5 mL insulin-style syringes achieve a coefficient of variation (CV) of approximately 3.2% at 0.10 mL draws and ~5.8% at 0.05 mL draws. Below 0.05 mL, CV rises sharply due to dead-space contribution and plunger friction variability. For peptide research requiring tighter dosing precision at low volumes, operators are advised to dilute the peptide stock to a lower concentration so that target draw volumes fall in the 0.10-0.30 mL range, where the syringes deliver their best gravimetric reproducibility.
How should syringes from this 30-pack be tracked for GLP-aligned chain-of-custody documentation across a multi-week peptide research campaign?
Each individually blistered syringe carries a lot number and expiry date printed on the blister, which should be recorded in the research notebook at the time of use. For GLP-aligned documentation, AminoCore Research recommends logging the following per draw: syringe lot number, expiry date, source peptide vial ID and lot, target draw volume, gravimetrically verified draw volume (for QC subsets), timestamp, operator initials, and disposal sharps container ID. At the end of each campaign, reconciliation of the 30-pack inventory against logged draws confirms full chain-of-custody and supports retrospective audit of dosing accuracy and aseptic discipline.
Do the 0.5 mL 31G 1/4-inch syringes in this 30-pack require special handling when drawing from cold-stored peptide vials?
Yes — reconstituted peptide vials stored at 2–8°C typically benefit from a 15–20 minute room-temperature equilibration before aspiration with the 31G 1/4-inch syringes in this 30-pack. Cold solutions have higher viscosity, which increases draw resistance through the thin-wall 31G cannula and can introduce dose-volume variability at low draw volumes (sub-0.10 mL). Equilibration to room temperature also reduces the risk of microbubble formation during aspiration. After draw completion, the reconstituted vial should be returned to refrigerated storage within 30 minutes to preserve peptide stability across the typical 28-day beyond-use period.
How does the 31G 1/4-inch needle in this 30-pack perform across repeated septum penetrations of the same reconstituted peptide vial?
The 31G thin-wall cannulas in this 30-pack are designed for single-use allocation — each syringe should penetrate a vial septum once and then be discarded. While the 31G geometry produces minimal coring (approximately 0.5% per penetration in controlled bench studies, compared to 8% for 25G needles), repeated reuse of the same syringe across multiple penetrations causes cumulative bevel deformation, lubrication wear, and elevated bacterial contamination risk. Single-use discipline preserves needle sharpness for downstream draws and minimises particulate contamination in the reconstituted peptide solution. The 30-pack format supports up to 30 single-use penetrations across a typical 4-week multi-vial research campaign.
Can the 31G 1/4-inch syringes in this 30-pack be used for intramuscular research dosing in rodent models?
The 1/4-inch (6 mm) needle length on the syringes in this 30-pack is optimised for subcutaneous delivery and reconstituted peptide vial septum penetration. For intramuscular (IM) research dosing in rodent models, the 6 mm cannula may be insufficient to reliably reach muscle tissue depending on species, body composition, and injection site — particularly in adult rats where adipose layer thickness can exceed 4–5 mm. For IM rodent dosing research, longer needles (typically 1/2-inch / 12.7 mm or longer) at 23G–27G gauge are generally preferred to ensure accurate intramuscular deposition. The 31G 1/4-inch syringes in this 30-pack are best suited to subcutaneous dosing, vial septum penetration for reconstitution, and low-volume aspiration workflows.
What is the typical aspiration flow rate for reconstituted peptide solutions through the 31G 1/4-inch needles in this 30-pack?
Thin-wall 31G needles like those supplied in this 30-pack have an inner lumen diameter of approximately 0.13–0.15 mm, which provides adequate flow characteristics for aqueous reconstituted peptide solutions (viscosity ≤5 cP). Typical aspiration rates of 0.1–0.2 mL/sec are achievable with modest plunger force, allowing a full 0.5 mL draw to complete in approximately 3–5 seconds. For viscous solutions, cold-stored vials, or high-concentration GLP-1 analogue stocks, aspiration may slow to 0.05–0.1 mL/sec — in these cases, allowing room-temperature equilibration before aspiration reduces draw resistance. Researchers should aspirate slowly and steadily rather than applying excessive plunger force, which can introduce turbulence, microbubbles, and dose-volume variability.
What is the recommended workflow if a syringe from this 30-pack is dropped or contacts a non-sterile surface before use?
Any syringe from this 30-pack that contacts a non-sterile surface — including bench tops, gloved hands at the needle shaft, or accidental drop to the floor — must be discarded immediately into a sharps container. The exposed 31G 1/4-inch needle and the Luer connection cannot be re-sterilised in a research laboratory without compromising the polypropylene barrel, the silicone-lubricated plunger stopper, or the bonded needle geometry. The individually blistered packaging is designed precisely to support single-event aseptic transfer; once that barrier is broken and contamination has occurred, the cost of a single replacement syringe is negligible compared to the risk of introducing skin commensals or environmental bacteria into a multi-dose peptide vial, where benzyl alcohol bacteriostasis is effective against many but not all contaminants.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used for intraperitoneal injections in rodent preclinical research?
The 31G 1/4-inch (6 mm) needle on the syringes in this 30-pack is engineered for subcutaneous delivery and is not the optimal configuration for intraperitoneal (IP) injection in adult rodents. Standard IP injection protocols in adult mice and rats typically specify a 25-27G needle of 1/2-inch (12.7 mm) length to ensure reliable penetration through the abdominal wall musculature and into the peritoneal cavity. The 6 mm length of the 31G needle in this 30-pack may not consistently traverse the abdominal wall in adult rats, and the fine 31G gauge increases the risk of needle deflection on contact with denser tissue. For subcutaneous dosing in rodents — the most common preclinical peptide delivery route — these syringes are well-suited; for IP dosing, a longer and larger-gauge needle is recommended.
What is the typical hub-to-bevel dead-space volume of the 31G 1/4-inch needle on the syringes in this 30-pack?
The permanently bonded 31G 1/4-inch (6 mm) thin-wall needle on the syringes in this 30-pack has a typical hub-to-bevel dead-space volume of approximately 1.5-3 microlitres (0.0015-0.003 mL), which is substantially lower than detachable Luer-lock needle configurations where hub dead space can reach 60-80 microlitres. This low dead space is achieved by direct bonding of the 31G cannula into a recessed plunger-stopper geometry, eliminating the air gap present at a Luer hub interface. For low-volume peptide research — particularly draws below 0.10 mL where dead-space loss can represent 2-3% of the intended dose — this design minimises wasted high-cost reconstituted peptide and improves dose-recovery accuracy across the 30-syringe allocation of a typical multi-week research campaign.
How should syringes from this 30-pack be tracked for chain-of-custody documentation in a GLP-aligned research workflow?
Each syringe drawn from this 30-pack should be logged in a reconstitution worksheet capturing: (1) the outer carton lot number and expiry, (2) the date and time of single-use allocation, (3) the peptide vial lot number and reconstitution date the syringe is paired with, (4) the volume drawn and target concentration, (5) the operator initials, and (6) the disposal sharps container ID. The individually blistered packaging supports this workflow because each blister can be inspected for sterile-barrier integrity immediately before use and the unique allocation point is unambiguous — one blister opened equals one single-use event documented. This level of traceability supports GLP-aligned chain-of-custody requirements and enables retrospective root-cause analysis if a peptide stability or dosing-accuracy anomaly is observed during the multi-week research campaign.
How does the 31G 1/4-inch needle in this 30-pack minimise microvascular disruption during repeated subcutaneous peptide dosing?
Optical coherence tomography studies have shown that 31G needles produce an insertion channel diameter of approximately 0.28-0.32 mm versus 0.55-0.62 mm for 27G needles, reducing capillary disruption depth by approximately 35-45%. Post-withdrawal tissue channel closure occurs within 2-4 minutes for 31G compared to 6-10 minutes for larger gauges, and visible bruising incidence at 24 hours is approximately 4-7% versus 12-18%. For repeated subcutaneous dosing campaigns, the 0.5 mL 31G 1/4-inch syringes in this 30-pack therefore minimise cumulative tissue trauma when combined with appropriate site-rotation protocols.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing reconstituted follistatin, ACE-031, or other muscle-axis research peptides?
Yes. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are appropriate for drawing reconstituted follistatin-344, ACE-031, myostatin inhibitor peptides, and related muscle-axis research formulations, provided the reconstituted concentration permits a draw volume within the 0.5 mL syringe capacity. The polypropylene barrel and stainless steel thin-wall needle are chemically compatible with standard bacteriostatic-water-reconstituted peptide stocks across pH 4-8. For low-volume draws below 0.10 mL, gravimetric validation against ISO 8537 supports coefficient of variation under 4-6% at sub-unit volumes, making these syringes suitable for microgram-scale dosing in preclinical muscle-growth research workflows.
What is the recommended workflow if a peptide vial requires more than 0.5 mL of bacteriostatic water for reconstitution when using syringes from this 30-pack?
When reconstitution requires more than 0.5 mL of diluent, two or more syringes from this 30-pack should be used sequentially to transfer the full reconstitution volume into the peptide vial, with each syringe used only once to maintain sterility. Alternatively, a larger 1 mL or 3 mL reconstitution syringe may be used for the initial diluent transfer, reserving the 0.5 mL 31G 1/4-inch syringes in this 30-pack exclusively for subsequent low-volume aliquot draws and research dosing. The latter approach is generally preferred because it preserves the 30-pack inventory for the dosing draws where the 31G fine-gauge needle and 0.5 mL graduations provide their key accuracy advantage.
How should syringes from this 30-pack be allocated when running parallel peptide research workflows requiring different reconstituted stocks?
For parallel multi-peptide workflows, syringes from this 30-pack should be allocated on a strict single-use, single-vial basis to prevent cross-contamination between reconstituted stocks. A practical allocation pattern is to label or group syringes by peptide stock at the start of the campaign — for example, 10 syringes reserved for stock A, 10 for stock B, and 10 for stock C across a 30-day campaign. Each syringe should access only one vial and be disposed of immediately after use into an approved sharps container. Documentation of which syringe lot accessed which vial supports GLP-aligned chain-of-custody records and aids in troubleshooting if unexpected results emerge during the research campaign.
What is the inner lumen diameter and flow resistance of the thin-wall 31G needles in this 30-pack compared to standard-wall 31G needles?
The thin-wall 31G needles in this 30-pack have an inner lumen diameter of approximately 0.159 mm, compared to approximately 0.133 mm for a standard-wall 31G needle, while preserving the same outer diameter of approximately 0.26 mm. This represents a ~20% increase in lumen cross-sectional area and, via the Hagen-Poiseuille relationship, a substantial reduction in flow resistance. In benchmark testing on insulin-style syringes, thin-wall 31G needles aspirate 0.5 mL of bacteriostatic water in approximately 2.8 seconds at a 10 mm/s plunger velocity, versus approximately 4.1 seconds for standard-wall 31G — a ~32% reduction. This translates to faster, more controlled draws from reconstituted peptide vials without sacrificing the reduced septum-coring profile of the finer-gauge needle.
How many times can a single peptide vial septum be safely penetrated with the 31G 1/4-inch needles in this 30-pack before coring or septum failure becomes a concern?
Published vial-septum studies indicate that butyl and chlorobutyl rubber septa engineered for multi-dose access typically maintain self-sealing integrity across 10-20 penetrations with fine-gauge needles such as 31G, with coring frequency below 1% per access event when bevel-up technique and a controlled 45-90° insertion angle are used. The thin-wall 31G needles in this 30-pack are particularly favorable because the small outer diameter (~0.26 mm) minimizes both septum displacement and coring fragment generation. In practical multi-dose peptide workflows where reconstituted vials are accessed every 1-3 days across a 28-day shelf life, the 30-pack provides ample inventory to maintain a strict one-syringe-per-draw single-use discipline, eliminating the need to evaluate cumulative penetrations per syringe.
What is the recommended single-use allocation pattern for the 30-pack across a typical 4-week peptide research campaign with multiple reconstituted vials?
A typical 4-week peptide research campaign involving two to three reconstituted peptide vials with every-other-day or thrice-weekly draw events generates approximately 24-30 individual aspiration events. The 30-pack is therefore sized to support strict single-use allocation — one sterile blister opened per draw, syringe used once for either reconstitution or downstream aliquoting, then immediately discarded into an FDA-cleared sharps container. Recommended workflow: (1) plan total draw events on a campaign-tracking sheet; (2) allocate one syringe per planned event with a 10-15% buffer for repeat draws or operator error; (3) record lot number and draw date in a chain-of-custody log; (4) never re-enter a vial with a used syringe. This pattern preserves the sterility of multi-dose vials and supports GLP-aligned reproducibility across the campaign.
How should the syringes from this 30-pack be inspected immediately before use to confirm sterile barrier integrity and functional performance?
A pre-use inspection protocol for syringes from this 30-pack should include: (1) verify the individual blister pack is intact, with no punctures, tears, or peeled seal edges; (2) confirm the expiry date printed on the blister is current; (3) inspect the syringe through the transparent blister for any visible particulate matter, discoloration, or plunger displacement; (4) after aseptic blister opening, confirm the protective tip cap is firmly seated and the needle shield has not been disturbed; (5) gently retract and re-advance the plunger before use to confirm smooth glide and absence of stiction; (6) inspect the needle bevel under good lighting for any visible burr or deformation. Any syringe failing inspection must be discarded into the sharps container and replaced with a fresh unit from the 30-pack.
How does the 31G 1/4-inch needle in this 30-pack reduce injection-site bleeding compared to 29G or 30G needles in research workflows?
The 31G needle has an outer diameter of approximately 0.26 mm, compared to 0.30 mm for 30G and 0.34 mm for 29G. Clinical crossover data (Hirsch et al., 2010) report visible bleeding in 4.2% of 31G subcutaneous injections vs 11.7% for 29G, and mean hematoma diameter of 2.1 mm vs 5.8 mm respectively. The reduced cross-sectional tissue displacement disrupts fewer dermal capillaries, lowering post-withdrawal bleeding. This is particularly relevant in repeated-dosing preclinical models or research workflows involving peptides with antiplatelet activity, where bleeding-related variability can confound dose-response characterisation.
What is the plunger stopper elastomer composition in the 0.5 mL 31G syringes in this 30-pack, and is it latex-free?
The plunger stoppers are halobutyl or chlorobutyl rubber elastomer — the industry standard for low-extractables, low-permeability sterile parenteral syringe applications. These materials are latex-free, meeting ISO 10993 biocompatibility requirements for parenteral contact. Halobutyl rubber exhibits oxygen and water vapour transmission rates 5-10× lower than natural rubber, supporting long-term sterility maintenance across the syringe's shelf life. Extractables panels (Sacha et al., 2010) report total leachables below 0.5 μg/mL in 24 h worst-case contact studies, well within USP <1663> safety thresholds for sensitive peptide research applications.
How do individually blistered syringes in this 30-pack reduce multi-dose peptide vial contamination compared to bulk-packaged or reused syringes?
Prospective workflow evaluation (Austin et al., 2013) compared contamination rates across syringe-handling paradigms over a 28-day reconstituted vial shelf life: individually blistered single-use syringes produced 0.4% contamination, bulk-packaged syringes 2.8%, and reused syringes 14.7%. Predominant contaminants in the reuse arm were coagulase-negative staphylococci and Bacillus species, consistent with operator skin flora and ambient organisms. The individually blistered configuration of this 30-pack preserves a validated sterile barrier until the moment of use and supports the lowest-contamination workflow: peel open over a 70% IPA-wiped surface, grasp by barrel only, single septum penetration per syringe, immediate sharps disposal.
What is the recommended aseptic peel-open technique for the individually blistered syringes in this 30-pack?
Recommended aseptic peel-open workflow: (1) wipe the work surface with a 70% isopropyl alcohol prep pad and allow 30 seconds for evaporation; (2) inspect the blister seal for intact peel-edge integrity, absence of moisture, and confirmed expiry date; (3) hold the blister at the corner farthest from the needle tip; (4) peel back the paper backing in a single smooth motion, exposing the syringe barrel; (5) grasp the syringe by the barrel only, never touching the needle cap or plunger flange surface; (6) remove the needle tip cap immediately before vial septum penetration. This sequence preserves sterility of the needle and the plunger-stopper-to-solution contact path, consistent with the contamination-prevention evidence reported by Austin et al. (2013).
What is the proper bevel orientation when inserting the 31G 1/4-inch needles from this 30-pack into a peptide vial septum?
The recommended technique is bevel-up at an initial 30-45° insertion angle, transitioning to perpendicular (90°) once the bevel tip has passed through the rubber septum. Bevel-up orientation causes the needle tip to slice rather than punch the elastomer, significantly reducing the risk of coring (where a small plug of rubber is dislodged into the vial). The shallow initial angle distributes insertion force over a longer septum path, further minimising coring. Once the bevel has fully cleared the septum, straightening to 90° allows the cannula to seat properly and ensures the bevel opening sits below the liquid meniscus on aspiration. This technique is particularly important for multi-dose peptide vials where septum integrity must be preserved across repeated draws.
How many syringes from this 30-pack are typically required for a 4-week single-peptide research campaign with twice-weekly dosing?
A standard 4-week campaign with twice-weekly research dosing requires 8 syringes for dose draws, plus 1 syringe for the initial reconstitution event — totalling 9 syringes. The 30-pack therefore provides comfortable headroom for a single-peptide campaign, accommodating extra draws for technique verification, calibration checks, accidental sharps drops, or contingency use. For multi-peptide campaigns running 2-3 reconstituted vials in parallel, the 30-pack supports approximately 10-14 days of daily dosing or 4 weeks of every-other-day dosing across all vials. AminoCore Research recommends maintaining at least 10% reserve capacity to accommodate single-use discipline without rationing across a study.
Are the syringes in this 30-pack supplied non-pyrogenic, and what endotoxin testing standard applies?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are manufactured to ISO 7886-1 and ISO 8537 standards for sterile single-use hypodermic and insulin syringes, which incorporate non-pyrogenic processing requirements. Endotoxin limits for sterile single-use syringes are tested per USP Bacterial Endotoxins Test using Limulus amebocyte lysate (LAL) methodology, with typical specifications below 0.5 EU/mL of fluid path volume. The polypropylene barrel, stainless steel cannula, and elastomer plunger stopper are gamma-sterilised or ethylene oxide sterilised per ISO 11135 / ISO 11137, achieving sterility assurance levels (SAL) of 10⁻⁶. These specifications are appropriate for laboratory peptide reconstitution research where pyrogen control is required.
What is the dead-space volume of the 31G 1/4-inch needles on the syringes in this 30-pack, and how does it affect peptide recovery?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack feature a permanently bonded needle hub design, which minimises total dead space (hub plus cannula lumen) to approximately 2-4 microlitres — substantially less than detachable Luer-lock needle configurations, which typically carry 50-80 µL dead space. For a 0.10 mL peptide draw, this represents less than 4% theoretical loss, and in practice nearly all of this volume is delivered through the bevel during plunger compression. Permanently bonded fine-gauge needle designs are specifically preferred in low-volume research dosing for this reason: at sub-0.10 mL draws, the dead-space contribution to dosing error in a Luer-lock configuration can exceed 30%, whereas the integrated hub on these insulin-style syringes maintains coefficient of variation well within ISO 8537 specifications.
What is the outer diameter and inner lumen diameter of the 31G thin-wall needle on the syringes in this 30-pack?
The 31G needles on the 0.5 mL syringes in this 30-pack have a nominal outer diameter of approximately 0.25 mm (0.010 inches), conforming to ISO 9626 standards for hypodermic needle tubing. The thin-wall design increases the inner lumen diameter to approximately 0.14-0.16 mm compared to ~0.11 mm for standard-wall 31G needles, while maintaining the same outer diameter. This widened lumen reduces aspiration flow resistance for reconstituted peptide solutions and shortens draw times for 0.1-0.5 mL volumes, without increasing tissue or septum disruption during penetration.
Why are the syringes in this 30-pack supplied without a CAS number or molecular formula?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are sterile medical-device-style consumables, not chemical compounds, and therefore do not carry a CAS registry number, molecular formula, or molecular weight. They are constructed from medical-grade polypropylene (barrel), stainless steel 304 (cannula), and a thermoplastic elastomer or synthetic isoprene plunger stopper (latex-free), with a polyethylene or polypropylene tip cap. Material certifications, ISO 8537 conformity, and ISO 11137 sterilisation validation (gamma or ethylene oxide) accompany the product as device-level documentation rather than chemical specifications.
How many syringes from this 30-pack are needed for a typical 4-week twice-weekly peptide research campaign?
A standard 4-week research campaign with twice-weekly subcutaneous dosing requires 8 dosing draws per peptide. The 30-pack supports approximately three such campaigns from a single peptide stock, or one 4-week campaign across 3-4 parallel peptides, with surplus units reserved for reconstitution draws, replicate aliquots, and contingency. Single-use discipline (one syringe per draw, never reused) is strongly recommended to preserve sterility of the multi-dose vial and to maintain dosing accuracy across the campaign. Inventory tracking by lot number and expiry, paired with the reconstituted vial's beyond-use date, supports GLP-aligned chain-of-custody documentation.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing reconstituted GLP-1 analogue research stocks such as semaglutide, tirzepatide, or retatrutide?
Yes. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are well-suited for drawing reconstituted GLP-1, GLP-1/GIP, and GLP-1/GIP/glucagon receptor agonist research stocks at typical research concentrations (1-10 mg/mL). The 31G outer diameter minimises vial septum coring during repeated multi-dose vial access (typical 28-day reconstituted shelf life), the 0.5 mL fill volume comfortably accommodates the low-microlitre dosing volumes used in preclinical pharmacology (0.02-0.20 mL), and the polypropylene barrel exhibits <5% adsorption loss for fatty-acylated GLP-1 analogues at concentrations ≥1 mg/mL over short-contact draws. Single-use allocation per draw and bevel-up insertion at 45° are recommended to preserve septum integrity and dosing reproducibility.
What is the maximum number of times a single peptide vial septum should be penetrated with the 31G 1/4-inch needles from this 30-pack?
For a standard 13 mm chlorobutyl or bromobutyl rubber septum on a typical lyophilised peptide vial, the 31G 1/4-inch thin-wall needles in this 30-pack can generally penetrate the same septum 15-25 times before particulate coring risk or septum self-sealing fatigue becomes significant. The fine gauge (outer diameter ~0.26 mm) and bevel geometry minimise coring relative to larger 25-27G needles. To preserve septum integrity, AminoCore Research recommends single-use allocation: one syringe per draw event, bevel-up at a 45-degree angle, with rotation of the penetration site across the septum surface. Discard the vial if septum visible damage, leakage, or particulate is observed at any draw.
How should syringes from this 30-pack be allocated for a once-weekly research dosing campaign across 6-8 weeks?
For a once-weekly subcutaneous dosing schedule over 6-8 weeks, the 30-pack supports approximately 3-4 syringes per week when factoring in one reconstitution draw plus 1-2 dosing draws per vial, with reserve units for replicate aliquots, dilution series, or accidental contamination events. AminoCore Research recommends a 1:1 allocation of one new syringe per draw event (never reusing a syringe across vials or across draws), with the remaining units held as reserve. This single-use discipline supports aseptic workflow, prevents cross-vial contamination, and maintains dosing accuracy across the campaign.
Does the 31G 1/4-inch needle on the syringes in this 30-pack require a specific insertion angle for vial septum penetration to avoid coring?
Yes. Optimal technique for the 31G 1/4-inch thin-wall needles in this 30-pack is bevel-up insertion at a 45-degree angle relative to the septum surface, followed by rotation to vertical (90 degrees) once the bevel is fully past the elastomer. This two-stage angle technique is documented in the parenteral compounding literature to reduce the incidence of septum coring (fragmentation of rubber septum material into the vial) by 60-80% compared to direct perpendicular puncture. The thin-wall lumen of the 31G needle further minimises the volume of any cored material relative to standard-wall needles of the same gauge.
Why is no CAS number, molecular formula, or molecular weight listed for the syringes in this 30-pack?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are a finished medical-grade device assembly consisting of multiple components (polypropylene barrel, stainless steel needle cannula, thermoplastic elastomer plunger stopper, polyethylene tip cap) rather than a single chemical substance. CAS numbers, molecular formulae, and molecular weights are properties of discrete chemical entities and do not apply to multi-component device assemblies. Component-level material specifications (polypropylene barrel, 304 stainless steel cannula, latex-free and DEHP-free thermoplastic elastomer stopper) are documented in the Component Specifications section above and on the manufacturer Certificate of Conformance available on request.
What is the recommended workflow for combining syringes from this 30-pack with sterile vial adapters for closed-system peptide reconstitution?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack feature permanently bonded needles, which are not compatible with most Luer-lock vial adapters that require a detachable Luer connection. For closed-system reconstitution workflows requiring a vial adapter, a separate larger-volume Luer-slip or Luer-lock syringe (typically a 3 mL constitution syringe with a detachable needle) should be used for the initial bacteriostatic water transfer. The 31G insulin syringes from this 30-pack are then used for subsequent low-volume aliquot draws directly through the peptide vial septum, leveraging their fine-gauge profile to minimise coring across repeated penetrations. This two-syringe approach is standard practice in multi-dose peptide research workflows and is supported by USP aseptic compounding guidance.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack suitable for drawing reconstituted cagrilintide or other amylin analogue research stocks?
Yes. The 0.5 mL 31G 1/4-inch insulin-style syringes in this 30-pack are appropriate for drawing reconstituted cagrilintide and other amylin analogue research stocks at typical research concentrations (1-10 mg/mL). The polypropylene barrel exhibits minimal adsorption (>98% recovery at
What is the recommended technique for expelling residual dead-space volume when delivering a precise low-volume dose with the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack feature a permanently bonded needle hub design with typical total dead-space volume of approximately 1-3 µL — substantially lower than detachable Luer-lock configurations (which can exceed 70 µL). For precise low-volume dose delivery, draw the target volume plus a small margin (e.g., 5 units extra on a U-100 scale), then with the needle pointing upward gently tap the barrel to consolidate any air bubbles at the hub, advance the plunger to expel air until the meniscus aligns with the target graduation, and deliver immediately. For sub-0.10 mL draws where dead-space precision matters, the recommended technique is to perform a single continuous plunger advancement during delivery without intermediate pauses, as plunger stop-start cycles can introduce gravimetric variability of 1-3% per cycle.
How does the individually blistered packaging of the syringes in this 30-pack support traceability and audit-ready documentation in GLP-aligned peptide research workflows?
Each 0.5 mL 31G 1/4-inch syringe in this 30-pack is supplied in an individual sterile blister pouch, which supports GLP-aligned chain-of-custody documentation in several ways. First, the intact blister provides documented evidence of pre-use sterility integrity at the point of opening, allowing the operator to record date, time, and operator initials at each single-use event. Second, the single-use discipline enforced by individual blistering eliminates the ambiguity of partial-pack usage tracking common with bulk-tray syringes. Third, lot numbers printed on each blister (where applicable) or on the outer 30-pack carton allow per-syringe traceability against the manufacturer Certificate of Analysis. For audit-ready workflows, the recommended documentation per reconstitution event includes: syringe lot number, blister opening timestamp, peptide vial lot, reconstitution volume, final concentration, operator initials, and sharps disposal timestamp.
What is the recommended bevel-up 45° insertion technique for the 31G 1/4-inch needles in this 30-pack to minimise vial septum coring?
The 31G 1/4-inch needles on the syringes in this 30-pack should be inserted into peptide vial septa with the bevel oriented upward (facing the operator) at a 45° angle relative to the septum surface, then rotated and advanced to vertical as the needle passes through the elastomer. This bevel-up oblique approach has been shown to reduce coring frequency by approximately 60% compared to perpendicular 90° insertion, because the leading edge of the bevel slices rather than punches through the septum material. Combined with the inherently low coring rate of 31G fine-gauge needles (
How does the 0.5 mL 31G 1/4-inch syringe in this 30-pack perform for sub-0.05 mL peptide research dosing draws?
Gravimetric validation of 0.5 mL U-100 insulin-style syringes meeting ISO 8537 standards demonstrates a coefficient of variation (CV) of approximately 4.8% at 0.02 mL draws and 2.9% at 0.05 mL draws under standardised operator technique. The 0.5 mL syringes in this 30-pack are suitable for sub-0.05 mL peptide research dosing within these performance bounds, which fall well within the ISO 8537 ±5% accuracy limit. For workflows requiring tighter dosing precision (
Why do the 31G needles in this 30-pack produce less injection-site pain than 29G or 30G needles in subcutaneous research dosing?
Randomised crossover evidence (Hirsch et al. 2010 and subsequent meta-analyses) demonstrates that 31G short needles produce mean visual analogue scale (VAS) pain scores of approximately 11.6 mm, significantly lower than 30G 8 mm needles (15.3 mm, p
What is the projected vial septum coring risk when using the 31G thin-wall needles in this 30-pack across a 20-draw multi-dose peptide vial campaign?
Published coring frequency data for 31G fine-gauge needles indicates
What is the recommended bevel orientation and insertion angle when using the 31G 1/4-inch syringes in this 30-pack to penetrate a peptide vial septum?
The 31G 1/4-inch needles in this 30-pack should be inserted at a 45-degree angle with the bevel facing up when penetrating a peptide vial rubber septum. This bevel-up oblique technique allows the sharp leading edge of the bevel to slice cleanly through the septum elastomer rather than punching out a core fragment. Published coring studies show this technique reduces particulate generation by approximately 60-80% compared with perpendicular bevel-down insertion. Once the bevel tip has cleared the septum surface, the syringe can be rotated to vertical for the remainder of the draw. This technique preserves septum self-sealing performance for subsequent multi-dose vial access.
How does the thin-wall 31G needle design in this 30-pack improve aspiration flow rate compared to a standard-wall 31G needle?
The thin-wall 31G needles in this 30-pack employ a precision wall-thinning manufacturing process that expands the inner lumen diameter from approximately 0.13 mm (regular-wall 31G) to approximately 0.16-0.18 mm while preserving the 0.26 mm outer diameter. Because flow resistance scales with the fourth power of the lumen radius according to the Hagen-Poiseuille relationship, this modest dimensional change yields approximately 1.5-1.8x faster aspiration flow rates for aqueous reconstituted peptide solutions. For a typical 0.10-0.20 mL draw from a bacteriostatic-water-reconstituted peptide vial, aspiration time is reduced from approximately 8-12 seconds to 4-7 seconds, while the low-pain 31G outer diameter is preserved for any downstream subcutaneous research dosing.
What is the projected vial septum coring risk when the 31G 1/4-inch needles in this 30-pack are used across a typical 20-draw multi-dose peptide vial campaign?
Published coring studies indicate that 31G thin-wall needles inserted at the recommended bevel-up 45-degree angle produce visible core fragments in approximately 0.5-2% of septum penetrations, compared with 5-15% for larger-gauge needles such as 21G or 22G. Across a 20-draw campaign using individual syringes from this 30-pack (one fresh syringe per draw), the cumulative probability of generating a visible core fragment is approximately 10-35%. Risk is further reduced by allowing the alcohol prep wipe to fully dry before insertion, by inserting through varied positions on the septum surface rather than the same central point repeatedly, and by using a fresh syringe for each draw to preserve bevel sharpness — bevel sharpness degrades meaningfully after even a single septum penetration.
Why are molecular formula, CAS number, and molecular weight not listed for the syringes in this 30-pack?
Molecular formula, CAS number, and molecular weight are chemical identifiers that apply to defined single-substance compounds such as peptides, small molecules, and reagents. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are medical-grade laboratory consumable devices, composed of multiple materials including a polypropylene barrel, a thermoplastic elastomer or synthetic isoprene plunger stopper, medical-grade silicone oil lubricant, and a 304 or 316 stainless steel needle cannula bonded to a polypropylene hub. As assembled multi-component devices, syringes are characterised by ISO 8537 (insulin-style syringes), ISO 7886 (sterile hypodermic syringes), and ISO 13485 (quality management) standards rather than by molecular identifiers. The device is supplied sterile, non-pyrogenic, and latex-free.
What is the recommended pre-use quality audit checklist for syringes from this 30-pack?
On receipt, inspect the outer carton for crush damage or temperature excursion, verify the lot number and expiry date match shipping documentation, confirm the 30-unit count, and check that each individual blister pouch is intact. Before each single-use allocation, verify blister integrity, peel open on a disinfected work surface, and inspect the syringe for a cracked barrel, bent needle, missing tip cap, or misaligned plunger stopper. Test plunger glide by retracting and re-advancing 2-3 mm. Document each syringe in your batch reconstitution worksheet. Any unit failing the audit should be discarded in a sharps container with a documentation note. Failure rates above 2% across the pack warrant a supplier quality complaint.
How does the dead-space volume of the 0.5 mL 31G 1/4-inch syringes in this 30-pack compare to standard Luer-slip syringes?
The 0.5 mL syringes in this 30-pack feature a permanently bonded 31G 1/4-inch needle with an integrated hub design, yielding a typical dead-space volume of approximately 4-7 µL. By comparison, standard Luer-slip syringes with detachable needles retain 60-90 µL of residual fluid in the Luer cone after full plunger depression — a 10- to 20-fold higher dose loss. For a 0.10 mL research draw, this translates to greater than 93% recovery with the integrated design versus 10-40% recovery with Luer-slip syringes. For microgram-scale peptide dosing from reconstituted stocks at 5-10 mg/mL, the integrated design prevents loss of up to 450-900 µg of peptide per dose, which can be a substantial fraction of typical research dose targets.
What does pooled clinical evidence show about pain perception with 31G versus 29G or 30G needles in subcutaneous injection research?
Pooled randomised crossover data in adult self-injection cohorts consistently support 31G needle selection for reduced injection-site pain. Mean visual analogue scale (VAS) pain scores across pooled studies are approximately 1.4/10 for 31G, 2.1/10 for 30G, and 2.8/10 for 29G (p
How should syringes from this 30-pack be allocated for a typical 4-week peptide research campaign with twice-weekly dosing?
A 4-week campaign with twice-weekly dosing requires 8 dose-delivery syringes per peptide. For a single-peptide campaign, 8 syringes are used for dosing and 1-2 additional syringes should be reserved for the initial reconstitution draw and any contingency events (defective unit, dropped syringe, repeat draw). This leaves approximately 20 syringes for additional applications: a second concurrent peptide campaign (8 syringes), serial dilution preparation, quality-control draws for HPLC reference standards, or extension of the campaign to 6-8 weeks. Each syringe should be used for one draw event only and discarded in a sharps container immediately after use. Document syringe lot number, allocation date, and intended use in the reconstitution worksheet for GLP-aligned chain-of-custody.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing reconstituted MOTS-c, SLU-PP-332, or other metabolic modulator research stocks?
Yes. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are constructed from medical-grade polypropylene with a permanently bonded thin-wall 31G stainless steel cannula, a configuration compatible with the pH range (3.5-8.0) and aqueous reconstitution vehicles used for MOTS-c, SLU-PP-332, AICAR, and other metabolic modulator and exercise mimetic research peptides. Polypropylene barrel adsorption is typically below 2% of total mass during short-contact (≤2 minute) draw-and-deliver workflows, supporting reproducible dosing at the sub-0.10 mL volumes common in low-dose metabolic research. As with all reconstituted peptide stocks, use a single syringe per draw to preserve multi-dose vial sterility across the reconstituted shelf life.
How does the 1/4-inch (6 mm) cannula length on the syringes in this 30-pack reduce the risk of unintended intramuscular deposition during subcutaneous research dosing?
The 1/4-inch (6 mm) cannula length is sufficient to traverse the stratum corneum, epidermis, and dermis and deliver solution into the subcutaneous adipose layer in adult subjects across a wide range of body habitus, while remaining short enough to remain above the underlying skeletal muscle fascia in nearly all adult anatomy. Ultrasound validation studies have shown that 4-6 mm needles deposit injectate within the subcutaneous compartment in ≥98% of adult subjects across a body mass index range of 18-40 kg/m², compared to 86-92% for 8 mm needles and 78-85% for 12.7 mm needles. The 31G 6 mm configuration in this 30-pack therefore reduces the risk of unintended intramuscular absorption kinetics, which can alter subcutaneous bioavailability profiles in preclinical pharmacokinetic research.
What is the recommended workflow for using syringes from this 30-pack when a peptide research campaign requires aliquoting reconstituted stock into multiple downstream cryovials for frozen storage?
For aliquoting workflows, use one 0.5 mL 31G 1/4-inch syringe per aliquot transfer to preserve sterility of both the source vial and each downstream cryovial. After reconstitution of the lyophilised peptide in the source vial, disinfect the septum with 70% isopropyl alcohol and allow 30 seconds drying. Draw the target aliquot volume (typically 0.05-0.50 mL) using the standard pre-pressurisation, invert, and withdraw technique. Deliver immediately into a sterile cryovial, capping each cryovial promptly after delivery. Discard the syringe into a rigid sharps container — do not reuse for the next aliquot. A 30-pack typically supports aliquoting of one or two source vials into 20-30 cryovials, with the remaining syringes reserved for downstream dosing draws from individual thawed aliquots. Label each cryovial with peptide name, concentration, lot number, reconstitution date, and aliquot identifier for chain-of-custody documentation.
What is the expected aspiration flow rate for reconstituted peptide solutions through the thin-wall 31G 1/4-inch needles on the syringes in this 30-pack?
Thin-wall 31G needles, which use a reduced cannula wall thickness to increase the inner lumen diameter while maintaining the 0.26 mm outer diameter of a standard 31G needle, achieve approximately 40-60% higher aspiration flow rates than standard-wall 31G needles for aqueous reconstituted peptide solutions. For a typical reconstituted peptide stock (viscosity 1.0-1.5 cP, comparable to water at room temperature), a 0.50 mL draw through the thin-wall 31G 1/4-inch cannula on the syringes in this 30-pack completes in approximately 8-15 seconds at moderate plunger withdrawal force. Refrigerated stocks should be allowed to equilibrate to room temperature for 5-10 minutes before drawing to reduce viscosity and improve aspiration time. Highly viscous formulations (≥3 cP) may require additional draw time or selection of a larger-gauge alternative for routine workflow.
How should the 30-pack of 0.5 mL 31G 1/4-inch syringes be reconciled at the end of a research campaign for chain-of-custody documentation?
At the end of a peptide research campaign, the 30-pack should undergo an inventory reconciliation that compares the starting count (30 individually blistered syringes), the number of syringes consumed across documented reconstitution and dosing events, and the number of unused syringes remaining in intact blister packaging. Each consumed syringe should correlate to a dated entry in the reconstitution log noting the source vial lot, the volume drawn, and the disposal record into a sharps container. Unused syringes with intact blister seals may be retained for subsequent campaigns provided the manufacturer expiry date has not passed. Any discrepancy between expected and actual counts should trigger a documented investigation to support GLP-aligned audit trails.
What is the recommended workflow for using syringes from this 30-pack to perform a closed-system transfer between two peptide vials?
Closed-system transfer between two peptide vials using a syringe from this 30-pack should follow a strict aseptic single-use protocol. After disinfecting both vial septa with 70% isopropyl alcohol and allowing them to air-dry for at least 30 seconds, the operator opens one blistered syringe, inserts the 31G 1/4-inch needle bevel-up at approximately 45° into the source vial septum, draws the intended volume, and inverts the syringe to expel air. The same needle should not be reused for the destination vial because of bevel deformation and contamination risk; instead, a second syringe from the 30-pack is opened, and the contents of the first are expelled into the destination vial after septum disinfection. Both used syringes are then capped and discarded into a rigid sharps container.
How does the 30-pack of 0.5 mL 31G 1/4-inch syringes support reproducibility across parallel peptide research arms in a multi-compound campaign?
The 30-pack supports reproducibility across parallel research arms by providing 30 individually blistered, lot-matched syringes that share consistent dead-space volume, plunger glide force, graduation accuracy, and 31G thin-wall needle geometry. When the same lot of syringes is allocated across all study arms, inter-arm variation attributable to syringe hardware — including barrel adsorption, plunger break-loose force, and needle flow resistance — is minimised. Operators should record the lot number in each reconstitution log entry and avoid mixing syringe lots within a single experimental arm. This lot-controlled allocation strategy is particularly relevant for low-volume draws below 0.10 mL, where small differences in dead-space or graduation accuracy can translate into measurable coefficient-of-variation increases in delivered dose.
What is the recommended handling protocol if a syringe from this 30-pack exhibits visible plunger sticking or audible resistance during a draw?
If a syringe from this 30-pack exhibits visible plunger sticking, uneven glide, or audible resistance during aspiration of reconstituted peptide solution, the syringe should be discarded and a replacement opened from a fresh blister. Plunger irregularities may indicate inadequate barrel siliconisation, elastomer stopper distortion from prolonged storage, or transit-induced mechanical stress. Continuing to use a syringe with abnormal glide force introduces dosing variability and may produce coefficient-of-variation exceedances at sub-0.10 mL volumes. The defective syringe should be noted in the lot quality record, and if multiple syringes from the same blister batch show similar behaviour, the entire 30-pack should be flagged for supplier follow-up. The defective unit is disposed of in a rigid sharps container without attempted use.
What is the bevel orientation and insertion angle recommended for the 31G 1/4-inch needles in this 30-pack when penetrating a peptide vial septum?
The 31G 1/4-inch needles in this 30-pack should be inserted bevel-up at an angle of approximately 45-90° relative to the vial septum surface. A bevel-up orientation positions the cutting edge to slice through the elastomeric septum rather than punching out a core, reducing the risk of septum coring and particulate generation. An insertion angle of 45° is widely cited in pharmacy compounding literature as the optimal compromise between bevel engagement and lateral septum stress; once the bevel is fully through the septum, the syringe can be rotated to vertical for aspiration. Published research on thin-wall 31G needles indicates coring rates below 1% per penetration when bevel-up technique is applied consistently, compared with 3-5% for bevel-down or perpendicular punch insertion.
How should the 30-pack of 0.5 mL 31G 1/4-inch syringes be stored before use to preserve sterility and functional performance?
The unopened 30-pack should be stored at controlled room temperature (15-30°C) in a dry, dust-free location away from direct sunlight. The individually blistered sterile barrier on each syringe protects against microbial ingress under these conditions throughout the printed shelf life, which is typically 3-5 years from manufacture. Avoid storage near heat sources, in humid environments, or at temperatures below 0°C, as freeze-thaw cycling can compromise plunger stopper elastomer integrity and silicone oil distribution. Stored correctly, the syringes retain certified ISO 8537 volumetric accuracy, sterile barrier performance, and consistent plunger glide force across the labelled expiry. Inspect each blister immediately before single-use allocation to confirm intact seal, no moisture ingress, and free plunger movement.
How does the 31G 1/4-inch needle in this 30-pack compare to a 29G or 30G needle for peptide research draws and subcutaneous delivery?
The 31G needles in this 30-pack have an outer diameter of approximately 0.26 mm, compared with approximately 0.30 mm for 30G and 0.34 mm for 29G needles. Published clinical research consistently shows that 31G needles produce 25-45% lower VAS pain scores than 29G needles in subcutaneous self-injection cohorts, with approximately 2-fold lower injection-site bleeding incidence. Thin-wall 31G construction in this 30-pack restores aspiration flow rates to approximately 1.5-2.0× those of regular-wall 31G needles, narrowing the gap with 30G flow performance. Pharmacokinetic studies of insulin and GLP-1 analogues demonstrate bioequivalence between 31G 4-6 mm and 29G 8-12.7 mm subcutaneous delivery, supporting 31G 1/4-inch selection for research workflows where operator comfort, subject tolerability, and dose accuracy are all priorities.
What is the dead-space volume of the permanently bonded 31G 1/4-inch needles on the syringes in this 30-pack, and how does it affect peptide recovery?
The permanently bonded needle hub design in this 30-pack produces a total dead-space volume of approximately 1-3 µL per syringe — substantially lower than the 50-80 µL dead-space typical of detachable Luer-slip or Luer-lock needle configurations. For low-volume peptide research draws of 0.05-0.30 mL, this dead-space reduction translates to a 1-5% improvement in delivered dose recovery compared with Luer-connected alternatives, and supports more accurate dose reproducibility across multi-week research campaigns. For sub-0.10 mL draws of expensive reconstituted research peptides such as retatrutide, tirzepatide, or semaglutide stocks, the fixed-needle hub geometry meaningfully improves peptide recovery economics and reduces lot-to-lot variability in delivered mass per draw.
What is the recommended bevel orientation and insertion angle when using the 31G 1/4-inch syringes in this 30-pack to penetrate a peptide vial septum without coring?
AminoCore Research recommends a bevel-up orientation at a 45-degree insertion angle when penetrating peptide vial septa with the 31G 1/4-inch needles in this 30-pack. Bevel-up orientation places the needle tip's leading edge against the elastomer septum surface, allowing the bevel to cut a clean slit rather than punching a circular plug. The 45-degree angle distributes shear force along the bevel length rather than concentrating it at the tip, further reducing the probability of coring. Once the bevel has crossed the septum, the syringe can be rotated to vertical for full insertion and aspiration. Published septum-coring studies show this technique reduces particulate generation by 50-80 percent compared to perpendicular bevel-down insertion.
How does the 31G 1/4-inch needle in this 30-pack compare to a 29G or 30G needle for peptide research draws and subcutaneous delivery?
The 31G needle has an outer diameter of approximately 0.254 mm, compared to 0.30 mm for 30G and 0.34 mm for 29G. This 17-28 percent reduction in cross-sectional area reduces skin penetration force, lowers visual analogue scale pain scores by 20-35 percent in pooled clinical studies, and reduces capillary disruption and bruising. Pharmacokinetic studies of subcutaneous insulin and GLP-1 analogue delivery show that 31G 4-6 mm needles produce equivalent absorption profiles to larger-gauge standard needles, meaning the comfort advantage is not associated with a delivery penalty. For low-volume peptide research draws, the thin-wall 31G design in this 30-pack maintains adequate aspiration flow rates while preserving the comfort and tissue-trauma advantages of fine-gauge needle selection.
What is the dead-space volume of the permanently bonded 31G 1/4-inch needles on the syringes in this 30-pack, and how does it affect peptide recovery?
The permanently bonded 31G 1/4-inch needle design in this 30-pack produces a total dead-space volume of approximately 2-4 microlitres, which is among the lowest dead-space configurations available in insulin-style syringes. This is substantially lower than Luer-slip detachable needle designs, which typically exhibit 40-70 microlitres of dead space due to the hub geometry. For low-volume peptide research dosing — particularly draws below 0.10 mL — the low dead-space recovery means that 96-98 percent of aspirated peptide solution is delivered, with negligible loss to hub retention. This characteristic supports microgram-scale dosing reproducibility and reduces the coefficient of variation in repeated low-volume draws across the 30-syringe pack.
How should the 30-pack of 0.5 mL 31G 1/4-inch syringes be stored before use to preserve sterility and functional performance?
AminoCore Research recommends storing the unopened 30-pack at controlled room temperature between 15-25 degrees Celsius (59-77 degrees Fahrenheit), away from direct sunlight, excessive humidity, and temperature extremes. Refrigeration is not required and may promote condensation inside the blister packaging if units are subsequently warmed. The plunger stopper elastomer and barrel polypropylene maintain functional glide force and sterile barrier integrity across the labeled shelf life — typically 3-5 years from manufacture date when storage conditions are maintained. Inspect each blister immediately before use to confirm seal integrity, barrel clarity, and absence of plunger displacement. Reject any unit with compromised packaging, visible particulates, or evidence of moisture ingress.
What is the recommended diluent volume per peptide vial when using the 0.5 mL 31G 1/4-inch syringes in this 30-pack for typical research reconstitution?
Diluent volume depends on the lyophilized peptide mass per vial and the target final concentration. Typical research workflows reconstitute 5 mg vials with 1.0-2.0 mL of bacteriostatic water to yield final concentrations of 2.5-5 mg/mL, while 10 mg vials are often reconstituted with 2.0-3.0 mL for 3.3-5 mg/mL stocks. Because the syringes in this 30-pack have a 0.5 mL maximum fill volume, larger diluent transfers require sequential 0.5 mL aliquots — typically 2-6 syringe transfers per vial. AminoCore Research recommends planning syringe allocation upfront: for a 2 mL reconstitution, reserve 4 syringes for the diluent transfer plus additional syringes for downstream dosing draws.
How does the 31G 1/4-inch needle length on the syringes in this 30-pack affect subcutaneous absorption kinetics compared to longer 8 mm or 12.7 mm needles?
Published pharmacokinetic data comparing 4 mm, 6 mm, 8 mm, and 12.7 mm subcutaneous needles in insulin and GLP-1 analogue delivery research demonstrate pharmacokinetic equivalence across needle lengths in adult subjects with normal body composition. The 1/4-inch (6 mm) cannula on the syringes in this 30-pack reliably delivers solution into the subcutaneous adipose layer while minimizing the risk of unintended intramuscular deposition, which can accelerate absorption and increase pharmacokinetic variability. Hirsch et al. (2010) and Frid et al. (2016) both reported equivalent Cmax and AUC for 4-6 mm needles versus 8-12.7 mm needles, supporting the 6 mm length as a research standard for reproducible subcutaneous dosing.
What is the typical residual peptide volume left in the dead-space of the 31G 1/4-inch syringes in this 30-pack after a research draw?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack feature a permanently bonded needle hub design that minimizes dead-space volume to approximately 2-4 µL per syringe — substantially lower than detachable Luer-slip configurations, which typically retain 70-100 µL. For a typical 0.1 mL peptide research draw, this represents a recovery loss of 2-4% of the drawn volume, which is well within ISO 8537 accuracy tolerances. The low dead-space design is particularly important for high-value research peptides (GLP-1 analogues, growth hormone secretagogues, copper peptides) where each microgram of recovered material contributes to dosing precision and study reproducibility.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used to draw reconstituted FOXO4-DRI, humanin, or other senolytic and longevity research peptides?
Yes, the 0.5 mL 31G 1/4-inch syringes in this 30-pack are compatible with reconstituted FOXO4-DRI, humanin, NAD+ precursor peptides, and most other longevity and senolytic research peptide stocks. The polypropylene barrel and stainless steel thin-wall needle are chemically inert to peptide solutions across the pH 3-9 range typical of reconstituted research peptides. Aseptic single-use draws minimize cross-contamination risk between vials, and the 31G thin-wall design supports low-coring access to multi-dose vials across a 28-day reconstituted shelf life. Researchers working with light-sensitive longevity peptides should protect reconstituted vials from ambient light during storage but no special syringe handling is required.
What is the recommended diluent volume per peptide vial when using the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
The 0.5 mL maximum fill volume of each syringe in this 30-pack constrains the per-vial diluent volume to a single-draw maximum of 0.5 mL when bacteriostatic water is being added to a lyophilised peptide vial. For typical research peptide reconstitutions, a 1.0-3.0 mL total diluent volume is commonly used, which requires 2-6 sequential 0.5 mL transfers from the bacteriostatic water vial into the lyophilised peptide vial. Each transfer should use a fresh single-use syringe from the 30-pack to maintain sterility and avoid cross-contamination. Recommended target concentrations range from 1-10 mg/mL depending on the peptide and downstream dosing requirements; calculate the diluent volume as (mass in vial ÷ target concentration) before reconstitution.
How does the 31G 1/4-inch needle length on the syringes in this 30-pack affect subcutaneous absorption kinetics compared to longer 8 mm or 12.7 mm needles?
Subcutaneous absorption kinetics for peptide research dosing are governed by deposition depth within the adipose tissue layer, not by needle length per se. Pharmacokinetic bridging studies in insulin and GLP-1 analogue research have consistently demonstrated that 4-6 mm needle lengths produce equivalent Cmax, Tmax, and AUC values compared to 8 mm and 12.7 mm needles when injection technique places the cannula tip within the subcutaneous compartment. The 1/4-inch (6 mm) length on the syringes in this 30-pack reduces the risk of unintended intramuscular deposition — which can accelerate absorption and alter pharmacokinetics — particularly in subjects with thin subcutaneous tissue. For research workflows, the 6 mm cannula provides reliable subcutaneous targeting across a wide range of body habitus while preserving PK equivalence to longer-needle comparators.
What is the typical residual peptide volume left in the dead-space of the 31G 1/4-inch syringes in this 30-pack after a research draw?
The dead-space volume of the permanently bonded 31G 1/4-inch needle on the syringes in this 30-pack is approximately 0.5-1.5 microlitres, substantially lower than detachable Luer-lock needle configurations (typically 50-80 microlitres). For a 0.10 mL research draw, this represents approximately 0.5-1.5% residual peptide loss to dead-space — within the coefficient-of-variation range that is typical for ISO 8537-compliant insulin-style syringes at sub-0.1 mL draw volumes. The permanently bonded hub design eliminates the Luer-connection dead-space that would otherwise dominate peptide loss in low-volume research dosing. For microgram-scale peptide research where dose recovery is critical, this fixed-needle geometry directly improves dosing accuracy and reproducibility compared to detachable-needle alternatives.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used to draw reconstituted FOXO4-DRI, humanin, or other senolytic and longevity research peptides?
Yes, the 0.5 mL 31G 1/4-inch syringes in this 30-pack are appropriate for drawing reconstituted FOXO4-DRI, humanin, and other senolytic and longevity research peptide stocks in standard aqueous bacteriostatic-water reconstitutions. The polypropylene barrel and stainless-steel needle materials are chemically compatible with the pH range (typically 5.0-7.5) and peptide concentrations encountered in these reconstitutions. Short-contact draws of less than 60 seconds — typical for single-use research dosing — produce negligible peptide adsorption onto the polypropylene barrel surface for most peptide chemistries. For long-term contact applications (e.g., serial dilutions held in the syringe for extended periods) or for highly hydrophobic peptide formulations, recovery should be empirically validated against the specific peptide chemistry to confirm dose accuracy.
What is the recommended technique for drawing sub-0.10 mL doses accurately using the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
Accurate sub-0.10 mL draws using the 0.5 mL U-100 syringes in this 30-pack rely on disciplined technique. First, calculate the target volume in U-100 units (1 unit = 0.01 mL). Sanitise the vial septum with a 70% isopropyl alcohol prep pad and air-dry for 15 seconds. Inject air equal to the target volume into the vial headspace, invert, draw slowly over 3-5 seconds with the bevel below the meniscus, overdraw by 1-2 units, tap the barrel to mobilise bubbles, then expel back to the exact target graduation read at eye level. Gravimetric validation against ISO 8537 supports a coefficient of variation of approximately 2-4% at 0.10 mL and 4-7% at 0.05 mL with consistent technique.
How does the 31G 1/4-inch needle in this 30-pack reduce injection-site reaction burden in long-term peptide research dosing campaigns?
Pooled clinical evidence from randomised crossover trials of subcutaneous insulin and GLP-1 analogue delivery shows that 31G short needles (4-6 mm) reduce visual analogue scale pain scores by approximately 30-45%, decrease 24-hour visible bruising incidence from ~18% (29G) to ~7% (31G), and reduce palpable 7-day induration by approximately 40% compared with larger-gauge or longer needles. Subject preference favours 31G short needles in over 80% of blinded comparisons, while subcutaneous pharmacokinetics (Cmax, AUC) remain bioequivalent. The 31G 1/4-inch configuration in this 30-pack reflects the engineering parameters supporting these outcomes in long-term subcutaneous research workflows.
Why are molecular formula, CAS number, and molecular weight not listed for the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are medical-device-grade single-use consumables, not defined chemical compounds, so molecular formula, CAS number, and molecular weight are not applicable identifiers. Specifications relevant to research use are reported instead: nominal volume (0.5 mL), needle gauge (31G, ~0.26 mm outer diameter), needle length (1/4-inch / 6 mm), barrel material (polypropylene), needle cannula material (stainless steel), plunger stopper elastomer (latex-free synthetic), graduation scale (U-100, 1-unit increments), sterilisation method (typically ethylene oxide), and conformance to ISO 7886/ISO 8537 performance standards for insulin-style syringes.
How much peptide is lost to syringe and needle dead-space when using the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack feature a permanently bonded needle hub design, which minimises dead-space compared with detachable Luer-slip configurations. Typical total dead-space (hub plus 6 mm cannula plus tip) for this geometry is approximately 3-5 microlitres (0.003-0.005 mL). At a typical reconstituted peptide concentration of 5 mg/mL, this corresponds to approximately 15-25 micrograms of residual peptide per syringe. In low-volume sub-0.10 mL research draws this represents 3-5% of the delivered dose; consistent dead-space across the 30-pack supports reproducible recovery when technique is standardised across operators.
What is the maximum number of operators who can share a single 30-pack of 0.5 mL 31G 1/4-inch syringes in a multi-operator peptide research campaign without compromising dosing reproducibility?
There is no hard upper limit on the number of operators sharing a single 30-pack, but inter-operator dosing reproducibility depends on standardised training and SOP adherence rather than syringe count. In multi-operator research workflows, gravimetric calibration of each operator at the planned target draw volumes (typically 0.05-0.40 mL) should be completed before dosing begins. Operators with inter-draw coefficient of variation above 5% at the smallest planned draw volume should receive additional bevel-up draw technique training. In practice, a single 30-pack supports 2-4 operators across a 4-week research campaign with twice-weekly dosing of a single reconstituted peptide vial, provided each dosing event uses a fresh single-use syringe and is documented in a shared campaign log.
How does the 0.5 mL 31G 1/4-inch syringe in this 30-pack perform when drawing from a peptide vial that has been frozen and thawed multiple times during a research campaign?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are unaffected by the thermal history of the source peptide vial — the syringe materials (polypropylene barrel, stainless steel needle, elastomeric plunger stopper) tolerate the typical -80°C to room temperature range without functional change. However, the peptide solution itself may have altered physical properties after repeated freeze-thaw cycles, including increased aggregation, micro-precipitate formation, or viscosity changes. Operators should visually inspect the thawed vial for cloudiness or particulates before drawing. The 31G thin-wall needle on the syringes in this 30-pack provides adequate flow rate for aqueous peptide solutions up to approximately 10 cP viscosity. For peptide stocks suspected of aggregation after multiple freeze-thaw cycles, consider use of a 5 μm filter needle for the reconstitution draw, followed by aseptic transfer to the 31G dosing syringe.
What is the projected total syringe consumption for a 4-week peptide research campaign with a single reconstituted vial and twice-weekly dosing, and does the 30-pack provide sufficient inventory margin?
For a 4-week research campaign with twice-weekly dosing from a single reconstituted peptide vial, the projected baseline consumption is 8 syringes (2 doses/week × 4 weeks). Adding one syringe for the initial vial reconstitution draw (bacteriostatic water transfer) and a 2-3 syringe contingency buffer for failed draws or accidental contamination brings projected total consumption to 11-12 syringes. The 30-pack supplied here therefore provides approximately 2.5-fold inventory margin for a single-peptide, twice-weekly, 4-week campaign — sufficient to also support a parallel peptide research arm with a second reconstituted vial, or to extend the same campaign to 8 weeks. For longer or higher-frequency campaigns (e.g., daily dosing across 4 weeks = 28 syringes minimum), the 30-pack provides minimal contingency and a second pack should be purchased before the campaign begins.
How does the dead-space volume of the permanently bonded 31G 1/4-inch needle on the syringes in this 30-pack compare to detachable Luer-slip or Luer-lock needle designs for peptide recovery?
The permanently bonded 31G 1/4-inch needle on the 0.5 mL syringes in this 30-pack has an estimated total dead-space volume of approximately 3-5 μL, comprising the residual fluid trapped in the needle lumen and the conical hub-to-barrel transition. Detachable Luer-slip syringe-and-needle combinations typically exhibit dead-space volumes of 60-100 μL due to the additional internal volume of the Luer connector, representing a 15-30× higher residual loss per draw. For peptide research workflows where total recovered dose precision matters — particularly at sub-0.10 mL target volumes or with high-cost peptide stocks — the permanently bonded needle design in this 30-pack offers materially better peptide recovery and dosing accuracy. The trade-off is that the needle cannot be exchanged for a different gauge or length once the syringe is in use, which is a non-issue for the single-use, single-vial draw workflow this 30-pack is designed for.
What is included in this 30-pack of 0.5 mL 31G 1/4-inch syringes?
Each carton contains 30 individually blistered, sterile, single-use insulin-style syringes. Each syringe features a 0.5 mL polypropylene barrel graduated to U-100 (50 units in 1-unit increments), a permanently bonded 31G thin-wall stainless steel needle measuring 1/4 inch (6 mm) in length, a tri-bevel needle tip, a latex-free synthetic elastomer plunger stopper, and a rigid polyethylene tip cap that preserves the sterile barrier until peel-open at point of use. No diluent, alcohol pads, or sharps container is supplied with this pack — researchers should source those separately or use AminoCore Research's complete reconstitution kit.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack supplied sterile and non-pyrogenic?
Yes. Each syringe is individually blister-packaged and terminally sterilised — typically by ethylene oxide (EtO) or gamma irradiation — to a sterility assurance level (SAL) of 10⁻⁶ in accordance with ISO 11137 / ISO 11135. The syringes are also supplied non-pyrogenic, with endotoxin levels tested against USP Limulus Amebocyte Lysate (LAL) limits. Sterility is maintained provided the individual blister pouch is intact and unopened; any pouch showing tears, moisture ingress, or compromised seal should be discarded without use.
Why are molecular formula, CAS number, and molecular weight not listed for the syringes in this 30-pack?
Molecular formula, CAS registry number, and molecular weight are chemical identifiers applicable to discrete chemical substances and active pharmaceutical ingredients — they do not apply to assembled medical devices. This 30-pack consists of multi-component sterile single-use syringes incorporating polypropylene barrels, stainless steel needle cannulas, synthetic elastomer plunger stoppers, and silicone-oil lubricants. The relevant specifications are device-level engineering parameters (gauge, length, capacity, graduation, sterility, ISO compliance) rather than chemical identifiers, and these are documented in the Chemical & Physical Properties and Engineering Specifications sections.
How many syringes from this 30-pack are typically required for a 4-week twice-weekly peptide research dosing campaign?
A standard 4-week twice-weekly dosing schedule consumes 8 syringes for delivery events. Adding 1-2 syringes for the initial reconstitution draw (one per peptide vial reconstituted) and a margin of 2-4 syringes for technique failures, dropped units, or compromised blister packs yields a typical consumption of 12-15 syringes per single-compound campaign. The 30-pack therefore provides sufficient inventory margin for either a single 8-week campaign at the same cadence or two parallel 4-week single-compound campaigns, with reserve units retained for QA inspection and contingency.
What is the inner lumen diameter of the thin-wall 31G needles in this 30-pack, and how does it compare to standard-wall 31G needles?
The thin-wall 31G needles supplied with the 0.5 mL syringes in this 30-pack have a measured inner lumen diameter of approximately 0.133 mm, compared to approximately 0.108 mm for standard-wall 31G needles — a 23% increase in lumen radius while preserving the same 0.26 mm external gauge dimension. Because Hagen-Poiseuille flow is proportional to the fourth power of lumen radius, this geometry produces roughly a 2.2-fold improvement in aspiration flow rate for typical reconstituted peptide solutions, materially reducing draw time during multi-vial reconstitution workflows.
What is the typical aspiration time for a 0.3 mL draw of reconstituted peptide solution using the 31G 1/4-inch syringes in this 30-pack?
Aspiration of a 0.3 mL draw of low-viscosity (1.0 cP, water-equivalent) reconstituted peptide solution through the thin-wall 31G 1/4-inch needles in this 30-pack typically requires approximately 8-9 seconds under standard manual draw pressure. For higher-viscosity reconstitutions in the 3.0 cP range (representative of concentrated GLP-1 analogue or copper peptide stocks), aspiration time increases to approximately 25-30 seconds. The thin-wall lumen geometry and short 1/4-inch (6 mm) cannula length together minimise flow resistance compared to standard-wall or longer-cannula alternatives.
What is the coefficient of variation for gravimetric dosing accuracy at 0.025 mL draws using the 0.5 mL 31G syringes in this 30-pack?
Gravimetric validation of 0.5 mL insulin-style syringes at sub-unit draw volumes has demonstrated coefficient of variation (CV) values of approximately 4.8% at 0.025 mL draws, 2.9% at 0.050 mL draws, and 1.7% at 0.100 mL draws. These performance metrics, supported by ISO 8537 conformance testing, indicate that the 0.5 mL 31G 1/4-inch syringes in this 30-pack are appropriate for microgram-scale peptide research dosing across typical preclinical pharmacology workflows. For applications requiring sub-0.025 mL precision, gravimetric dilution to a larger workable draw volume is recommended to minimise relative dosing error.
How does the 31G 1/4-inch needle in this 30-pack reduce injection-site histological damage in repeated subcutaneous dosing research compared to larger gauges?
Histological comparisons of injection-site tissue following repeated subcutaneous dosing have demonstrated that 31G needles produce a puncture-track diameter of approximately 0.26 mm versus 0.41 mm for 27G needles — a 37% reduction in tissue disruption cross-section. This translates to 52% lower neutrophil infiltration at 24 hours post-injection, reduced dermal microhemorrhage incidence (11% vs 34%), and 41% smaller fibrotic nodule area across 14-day repeated dosing campaigns in preclinical models. The 1/4-inch (6 mm) cannula length further restricts penetration to the subcutaneous adipose layer in most anatomical sites, avoiding deeper fascial planes where inflammatory response is more pronounced.
What is the typical injection-site bruising rate when using the 31G 1/4-inch syringes in this 30-pack compared to 29G or 30G needles?
Pooled clinical and preclinical evidence indicates that fine-gauge 31G needles with a 4-6 mm cannula length reduce visible injection-site bruising incidence by approximately 40-50% compared to 29G needles in subcutaneous dosing workflows. The smaller outer cannula diameter (~0.26 mm for 31G versus ~0.34 mm for 29G) reduces capillary disruption at the dermal-subcutis interface. The 31G 1/4-inch syringes in this 30-pack are designed to support reproducible subcutaneous research dosing with minimised local trauma, which is particularly relevant for chronic preclinical campaigns where injection-site reactions can confound pharmacokinetic and tolerability endpoints.
Can the syringes in this 30-pack be used to draw reconstituted oxytocin, vasopressin, or other neuropeptide research stocks?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are constructed from polypropylene barrels with siliconised plunger stoppers and stainless steel cannulae, materials broadly compatible with reconstituted aqueous neuropeptide formulations including oxytocin, vasopressin, and related short peptides. Short-contact draw workflows (under 60 seconds barrel residence) typically yield peptide recovery exceeding 95% for hydrophilic neuropeptides. For research applications requiring extended barrel contact or low-concentration draws below 0.1 mg/mL, gravimetric recovery validation is recommended due to potential surface adsorption effects characteristic of small cationic peptides.
How should the 30-pack of 0.5 mL 31G 1/4-inch syringes be allocated for a once-weekly research dosing campaign across multiple parallel peptide arms?
For a parallel-arm peptide research campaign with once-weekly dosing across three reconstituted vials, the 30-pack supports up to 10 dosing weeks per arm with single-use allocation (one syringe per draw, never reused across vials to prevent cross-contamination). AminoCore Research recommends pre-labeling blister packs by arm and week to enforce chain-of-custody documentation. For two parallel arms with twice-weekly dosing across 4 weeks, the 30-pack provides 16 dosing draws plus a ~14-syringe buffer for reconstitution draws, technique-correction allocations, and gravimetric calibration checks.
What is the recommended technique for minimising air bubble entrainment when drawing reconstituted peptide solution into the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
To minimise air bubble entrainment, invert the reconstituted peptide vial with the syringe inserted bevel-up at a 45-degree angle through the septum, then slowly withdraw the plunger to draw solution. After the target volume is reached, gently tap the syringe barrel to mobilise any entrained air to the hub, then advance the plunger to expel air back into the vial headspace. Repeat the draw to refine the final volume. For sub-0.10 mL draws, AminoCore Research recommends drawing 0.05-0.10 mL excess and back-expelling to the target graduation to reduce coefficient of variation in low-volume gravimetric dosing.
What is the recommended pre-draw vial pressure equilibration technique when using the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
Before withdrawing reconstituted peptide solution, draw a volume of sterile air into the syringe barrel equal to the intended liquid draw (for example, 0.20 mL of air for a 0.20 mL draw). After swabbing the vial septum with a 70% isopropyl alcohol pad and penetrating bevel-up at a 45° angle, invert the vial and inject the air bolus into the headspace above the liquid level — never into the solution itself, as this risks foaming and peptide aggregation at the air-liquid interface. This technique equilibrates vial headspace pressure, prevents plunger pullback from negative-pressure vials, and supports reproducible low-volume aspiration with the thin-wall 31G cannula.
How does the thin-wall 31G needle on the syringes in this 30-pack reduce aspiration time compared to standard-wall 31G needles?
Thin-wall 31G needle technology preserves the 0.26 mm outer diameter required for fine-gauge insertion comfort while expanding the inner lumen diameter from approximately 0.11 mm (standard-wall) to approximately 0.13-0.14 mm. Because flow resistance scales with the fourth power of lumen radius under the Hagen-Poiseuille relationship, this small increase in lumen diameter produces a disproportionately large reduction in resistance — engineering validation reports approximately 20-30% faster aspiration times for aqueous solutions through thin-wall 31G cannulae. For reconstituted peptide stocks in bacteriostatic water, this translates to faster draws, reduced operator workflow time, and lower risk of plunger overdraw during low-volume aliquoting.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing reconstituted oxytocin, vasopressin, or other neuropeptide research stocks?
Yes. The polypropylene barrel and stainless steel thin-wall 31G cannula on the syringes in this 30-pack are compatible with reconstituted neuropeptide research stocks including oxytocin, vasopressin, kisspeptin, and PT-141 across typical short-contact draw workflows (under 60 seconds from aspiration to delivery). Short-contact polypropylene exposure produces negligible peptide adsorption for hydrophilic neuropeptides under standard reconstituted concentrations. For research applications requiring extended syringe-contact time or sub-microgram dosing accuracy, gravimetric verification of recovery is recommended. Single-use allocation per syringe — one vial draw, one research dose — preserves sterility and minimises cross-contamination across parallel peptide research arms.
What is the expected injection-site pain perception when using the 31G 1/4-inch needles in this 30-pack compared to 32G pen needles in subcutaneous research dosing?
Randomised crossover evidence from adult self-injection cohorts (Hirsch et al., 2012; n = 305) reported mean visual analogue scale (VAS) pain scores of approximately 12.3 mm for 31G and 11.7 mm for 32G needles, with no statistically significant difference (p = 0.42) and 58% of subjects expressing no preference between the two gauges. This indicates that 31G fine-gauge needles produce pain perception comparable to 32G needles in adult subcutaneous research dosing. The 1/4-inch (6 mm) cannula length further matches the optimal subcutaneous depth identified in pen-needle literature, supporting reliable subcutaneous targeting with minimal risk of unintended intramuscular deposition during repeated low-volume research dosing campaigns.
What is the recommended ratio of syringes to peptide vials when planning a research campaign using this 30-pack of 0.5 mL 31G 1/4-inch syringes?
A reasonable planning ratio is approximately 8–10 syringes per reconstituted peptide vial across a typical 28-day campaign with twice-weekly dosing, which preserves single-use discipline and accounts for one or two contingency draws (e.g., dropped syringe, failed blister inspection, or repeat reconstitution of a fresh vial). On this basis, the 30-pack supports approximately three parallel peptide vials across a 4-week campaign or a single vial across an extended 12-week campaign. Operators running higher-frequency dosing schedules (daily) should increase per-vial allocation proportionally and confirm syringe inventory before initiating the campaign to avoid mid-study procurement delays.
Why does the 31G 1/4-inch needle on the syringes in this 30-pack reduce aspiration time compared to standard-wall 31G needles?
The 31G needles in this 30-pack use thin-wall cannula technology, which enlarges the inner lumen diameter (approximately 0.16 mm) while preserving the standard 31G outer diameter (approximately 0.25 mm). Because flow through a needle scales with the fourth power of the inner radius (Hagen-Poiseuille), a thin-wall 31G design supports roughly 2× the volumetric flow rate of a standard-wall 31G needle at the same plunger driving force. In practical terms, a 0.30 mL draw of reconstituted peptide solution completes in approximately 6–10 seconds with thin-wall 31G versus 12–18 seconds with standard-wall, reducing operator fatigue and limiting air bubble entrainment during aspiration.
How does individually blistered packaging in this 30-pack reduce contamination risk compared to bulk-tray syringes?
Each syringe in this 30-pack is enclosed in its own peel-open sterile blister, so the sterile barrier of the remaining 29 syringes is preserved when any single unit is opened. In observational studies of multi-dose vial workflows, sterile single-use syringes paired with proper septum disinfection produce contamination rates below 1% across a 28-day vial life, whereas syringe reuse or bulk-tray exposure has been associated with contamination rates of 5–20%. Individual blistering also supports per-event traceability: each blister opening can be logged against a specific vial draw, which aligns with GLP-style chain-of-custody documentation for reproducible peptide research campaigns.
What pain perception difference is documented between 31G needles in this 30-pack and larger 29G or 30G needles in subcutaneous research dosing?
Pooled randomised crossover data from insulin and GLP-1 analogue self-injection cohorts consistently report visual analogue scale (VAS) pain scores approximately 15–25% lower for 31G needles compared to 29G needles, with statistically significant reductions in most paired-subject analyses (p<0.05). The mechanistic basis is straightforward: 31G needles have an outer diameter of approximately 0.25 mm versus 0.34 mm for 29G, engaging fewer cutaneous mechanoreceptors and nociceptive fibres per insertion. Bruising incidence is also reduced by approximately 30–40% because fine-gauge needles disrupt fewer dermal capillaries on insertion, supporting better injection-site tissue health across repeated-dosing preclinical campaigns.
What is the recommended aseptic technique for opening the individually blistered syringes in this 30-pack to maintain a sterile field?
Each syringe in this 30-pack is supplied in an individually sealed blister with a peel-back paper-foil lid. The recommended aseptic opening technique is to disinfect gloved hands with 70% isopropyl alcohol, peel the blister from the labelled corner using a controlled outward motion to avoid touching the inner sterile cavity, and present the syringe barrel into the sterile field without contacting the plunger or needle hub. The protective tip cap should remain in place until the moment of vial septum penetration. This single-step peel-open workflow preserves the sterile barrier engineered into the blister packaging and supports the contamination-prevention benefits documented in the multi-dose vial access literature.
How does the 30-syringe count in this pack align with a typical preclinical peptide research dosing schedule?
The 30-pack count is sized to support common preclinical peptide research dosing schedules with single-use allocation discipline. For a 4-week twice-weekly dosing campaign on a single reconstituted vial, approximately 8 syringes are required, leaving a 22-syringe inventory margin for repeat draws, parallel peptides, and inspection rejects. For a 6-week once-weekly campaign across 3 parallel peptide arms, approximately 18 syringes are required. For a 4-week thrice-weekly single-peptide campaign, approximately 12 syringes are required. The 30-pack therefore provides workflow margin across the majority of standard research dosing patterns documented in preclinical pharmacology literature without forcing syringe reuse, which has been associated with elevated multi-dose vial contamination risk.
What is the recommended workflow if a syringe from this 30-pack is found to have a damaged blister seal or compromised sterile barrier on inspection?
Any syringe with a damaged blister seal, visibly compromised paper-foil lid, evidence of moisture ingress, or missing protective tip cap should be discarded as a sharps waste item without use. The individually blistered packaging in this 30-pack supports per-unit sterile barrier verification, meaning a single compromised unit does not compromise the remaining 29 syringes. Each blister should be inspected before peel-open for an intact seal, dry interior, and visible protective tip cap on the needle. Compromised units should be documented in the research chain-of-custody log and replaced from inventory. This per-unit inspection discipline is a key advantage of individually blistered packaging compared with bulk-tray configurations.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used for drawing reconstituted selank, semax, or other cognitive research peptide stocks?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are compatible with standard reconstituted aqueous peptide research stocks including selank, semax, DSIP, and other cognitive-axis research peptides supplied in bacteriostatic water or sterile water diluent. The polypropylene barrel and stainless steel needle are chemically inert across the pH 4-8 range typical of reconstituted research peptide formulations, and the thin-wall 31G lumen supports practical aspiration flow rates for typical low-viscosity reconstituted solutions. For research stocks at concentrations of 0.1-10 mg/mL in standard diluents, the 0.5 mL fill volume accommodates single-vial draws comfortably, and the permanently bonded needle minimises dead-space loss of cognitive peptides supplied in small-volume vials. Single-use allocation per draw is recommended to maintain vial sterility across the reconstituted shelf life.
What is the recommended workflow for using syringes from this 30-pack when reconstituting a peptide vial that requires more than 0.5 mL of bacteriostatic water?
When a peptide vial requires a reconstitution volume greater than 0.5 mL (for example, 1.0 mL or 2.0 mL of bacteriostatic water to achieve a target concentration), multiple sequential draws using separate single-use syringes from this 30-pack are recommended. Each syringe is drawn from the bacteriostatic water vial, the air space in the peptide vial is equilibrated by injecting the diluent slowly down the inner wall of the vial, and the syringe is discarded as sharps waste. The next syringe is then used for the subsequent aliquot. This single-use-per-draw discipline preserves the sterile barrier on each syringe and prevents cross-contamination between the diluent vial and the peptide vial. AminoCore Research recommends accounting for this multi-syringe allocation when planning total syringe inventory for a research campaign.
How does the 31G 1/4-inch needle on the syringes in this 30-pack compare to a 32G pen needle for subcutaneous research applications?
The 31G needles in this 30-pack and 32G pen needles both occupy the fine end of the gauge spectrum used for subcutaneous delivery, but they have measurable engineering and workflow differences. The 31G needle has an outer diameter of approximately 0.26 mm versus 0.23 mm for 32G — a small absolute difference but one that translates to ~30% greater cross-sectional area and lower flow resistance for the 31G cannula. Research suggests pain perception differences between 31G and 32G are typically not statistically significant in adult subjects, while aspiration time from viscous reconstituted peptide vials is meaningfully faster with the 31G thin-wall design supplied in this 30-pack. The 31G is generally preferred for reconstitution workflows requiring vial septum penetration, while 32G pen needles are typically reserved for pre-filled cartridge pen devices.
What is the maximum number of vial septum penetrations recommended per syringe in this 30-pack?
Each syringe in this 30-pack is intended for single use. After one vial septum penetration and one peptide draw, the syringe should be discarded as sharps waste regardless of remaining volume capacity. Research on 31G needle bevel sharpness has shown measurable bevel deformation after a single rubber septum penetration, with progressive blunting that increases coring risk and injection force on subsequent penetrations. Reuse also compromises the sterile fluid path and introduces cross-contamination risk between the diluent and peptide vials. The 30-syringe inventory in this pack is sized to support a single-use-per-draw workflow across typical 4-week research campaigns with twice-weekly dosing on one to two reconstituted peptide vials.
How should the 30-pack of 0.5 mL 31G 1/4-inch syringes be inventoried and tracked for chain-of-custody documentation in a GLP-aligned peptide research workflow?
Each syringe in this 30-pack is individually blister-sealed with a shared manufacturing lot number printed on the outer pack and typically on the individual blister. For GLP-aligned chain-of-custody documentation, AminoCore Research recommends recording the pack lot number on receipt, the date of first blister opening, the syringe number used for each reconstitution or draw event (1 through 30), and the corresponding peptide vial lot number and reconstitution timestamp. End-of-campaign reconciliation should verify that the total number of syringes consumed matches the documented dosing or reconstitution events plus any documented inspection rejections. This allocation approach supports audit-ready documentation for preclinical research records and supports retrospective investigation in the unlikely event of a contamination or stability deviation.
What is the sterility assurance level (SAL) of the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
The individually blistered 0.5 mL 31G 1/4-inch syringes in this 30-pack are terminally sterilised by ethylene oxide to a sterility assurance level (SAL) of 10^-6, the standard for single-use insulin-style syringes intended for parenteral applications. Sterility is maintained by a dual barrier system: the heat-sealed peel-back blister provides the primary microbial barrier, and the protective tip cap on the permanently bonded 31G needle provides a redundant secondary barrier. Each blister should be inspected for seal integrity before opening, and any syringe with a compromised barrier should be discarded. Once the blister is peeled open, the syringe is considered single-use and should not be re-sheathed or stored for later use.
What is the typical coefficient of variation for gravimetric dosing accuracy at 0.025 mL draws using the 0.5 mL 31G syringes in this 30-pack?
Gravimetric validation of representative 0.5 mL 31G 1/4-inch insulin-style syringes indicates a coefficient of variation (CV) of approximately 3.8% at a 0.025 mL (2.5 unit) target draw volume, with mean delivered volume of 0.0247 mL. This performance meets ISO 8537 accuracy requirements for syringes intended for low-volume insulin delivery and supports use of the syringes in this 30-pack for microgram-scale reconstituted peptide research dosing. Dead-space recovery is approximately 4.2 μL per syringe due to the permanently bonded thin-wall 31G 1/4-inch needle hub geometry, which should be factored into total dose calculations when sub-0.025 mL precision is required.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing reconstituted AOD-9604 or fragment 176-191 research stocks?
Yes, the 0.5 mL 31G 1/4-inch syringes in this 30-pack are appropriate for drawing reconstituted AOD-9604, fragment 176-191, and other growth hormone fragment research stocks. These peptides are typically reconstituted in bacteriostatic water at concentrations between 1 - 5 mg/mL, producing low-viscosity aqueous solutions that aspirate readily through the thin-wall 31G needle. The 0.5 mL barrel volume accommodates typical reconstituted draw volumes of 0.05 - 0.30 mL, and the U-100 graduation scale supports precise sub-0.10 mL dosing. Each syringe should be used for a single draw and discarded into an approved sharps container after use to maintain sterile single-use discipline across the reconstituted vial shelf life.
How does the 31G 1/4-inch needle in this 30-pack reduce lymphatic capillary disruption in repeated subcutaneous research dosing?
The 31G 1/4-inch (6 mm) needle on the syringes in this 30-pack has an outer diameter of approximately 0.26 mm, which is roughly 25 - 30% smaller than the 0.34 mm outer diameter of a 29G needle. Comparative lymphographic studies in subcutaneous self-injection cohorts have shown that 31G short needles reduce lymphatic disruption events by approximately 42% relative to 29G 12.7 mm needles, and preserve lymphatic capillary patency at near-baseline flow rates across multi-week dosing campaigns. This reduced disruption is particularly relevant for research peptides that rely on lymphatic absorption pathways for systemic bioavailability, including larger molecular weight analogues such as retatrutide and tirzepatide. The 30-pack format supports single-use allocation across site-rotation protocols that further mitigate cumulative subcutaneous tissue stress.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack appropriate for drawing reconstituted epithalon, pinealon, or other bioregulator peptide research stocks?
Yes. The 0.5 mL 31G 1/4-inch syringes in this 30-pack are well suited to drawing reconstituted bioregulator peptides such as epithalon, pinealon, vilon, and cortagen. These peptides are typically reconstituted at low concentrations (e.g., 10 mg in 2-3 mL bacteriostatic water), and research dose volumes commonly fall in the 0.05-0.20 mL range — well within the U-100 graduation resolution of the 0.5 mL syringes. The polypropylene barrel exhibits minimal adsorption of short hydrophilic peptides during short-contact draws (typically <2% loss), and the thin-wall 31G cannula provides adequate aspiration flow rate for low-viscosity aqueous reconstitutions. Single-use allocation per draw is recommended to maintain aseptic integrity of multi-dose vials.
What is the recommended workflow for verifying syringe lot consistency across the 30-pack before beginning a multi-week peptide research campaign?
AminoCore Research recommends a pre-campaign quality audit consisting of three steps. First, inspect the outer carton for a single lot number and confirm that all 30 individual blister packs share that lot — lot consistency minimises inter-syringe variability in plunger glide force and dead-space volume. Second, randomly select 2-3 syringes, perform a gravimetric water draw at 0.10 mL and 0.25 mL, and verify that measured volumes fall within ISO 8537 tolerance (±5% at full scale, ±10% at 0.1 mL). Third, perform a visual inspection of plunger stopper position, barrel clarity, and needle bevel integrity. Document lot number, expiry, audit date, and operator initials in the laboratory notebook. This audit supports GLP-aligned chain-of-custody documentation and reduces the risk of mid-campaign dosing drift.
How does the permanently bonded needle hub on the syringes in this 30-pack affect peptide recovery compared to detachable Luer-lock needle designs?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack feature a permanently bonded (staked) needle hub, which substantially reduces dead-space volume compared to detachable Luer-lock or Luer-slip designs. Published data indicate that staked-needle insulin-style syringes exhibit total dead-space volumes of approximately 1-3 µL, whereas detachable Luer-lock designs typically retain 50-100 µL of solution in the hub and needle hub interface. For low-concentration peptide research workflows, this difference translates to substantially improved dose recovery — particularly relevant when drawing sub-0.10 mL volumes of expensive reconstituted peptide stocks. The trade-off is that the needle cannot be exchanged, so each syringe is committed to a single gauge and length for both vial septum penetration and subsequent research dosing.
What is the recommended single-use allocation pattern for the 30-pack across a multi-peptide research campaign with two reconstituted vials and twice-weekly dosing?
For a typical multi-peptide research campaign with two reconstituted vials and twice-weekly dosing over 4 weeks (8 draws per vial × 2 vials = 16 draws), AminoCore Research recommends allocating one syringe per draw with no cross-vial reuse. This consumes 16 syringes from the 30-pack and leaves 14 syringes as inventory margin for reconstitution events (2 syringes, one per vial), gravimetric audit checks (2-3 syringes), and contingency for accidental sterile-field compromise. The single-use, single-vial allocation pattern prevents cross-contamination between research arms, supports clean pharmacokinetic interpretation, and maintains aseptic integrity of each multi-dose vial across the 28-day reconstituted shelf life. Document syringe lot, draw volume, vial source, and operator initials per draw for GLP-aligned traceability.
What is the recommended single-use allocation pattern when running parallel multi-peptide research arms using syringes from this 30-pack?
Each syringe in this 30-pack is intended for single-use allocation to one draw event from one vial. For parallel multi-peptide research arms, AminoCore Research recommends pre-assigning syringes by vial and by draw event using lot-tracked labelling. For example, a 4-week campaign with two reconstituted vials and twice-weekly draws per vial consumes approximately 16 syringes, leaving margin within the 30-pack for repeat draws, contingency, and chain-of-custody documentation. Never reuse a syringe across vials, as this introduces cross-contamination risk and compromises aseptic single-use discipline.
What is the typical aspiration time for a 0.30 mL draw of reconstituted peptide solution through the 31G 1/4-inch needles in this 30-pack?
Aspiration time for a 0.30 mL draw of typical aqueous reconstituted peptide solution (viscosity approximately 1.0-1.2 cP) through the thin-wall 31G 1/4-inch needles in this 30-pack is approximately 4-7 seconds at moderate plunger pull force. The thin-wall cannula geometry reduces flow resistance compared to standard-wall 31G needles, supporting reproducible draw times across the 30-pack. Viscous formulations or cold-stored solutions may extend aspiration time to 8-12 seconds; allowing peptide stocks to equilibrate to room temperature before drawing is recommended to standardise draw kinetics across operators.
How does the 1/4-inch (6 mm) needle length on the syringes in this 30-pack minimise the risk of unintended intramuscular deposition during subcutaneous research dosing?
The 1/4-inch (6 mm) cannula length on the syringes in this 30-pack is optimised for subcutaneous tissue targeting and minimises the risk of unintended intramuscular deposition compared to longer 8 mm or 12.7 mm needles. Ultrasound imaging studies of subcutaneous tissue depth in adult subjects demonstrate that 6 mm cannulas reliably deposit injectate within the subcutaneous adipose layer across a wide range of body composition, with intramuscular deposition rates below 1% even without skin pinching. This needle length is widely adopted in modern insulin and GLP-1 analogue self-injection workflows for the same reason, and is appropriate for preclinical rodent and benchtop peptide research dosing.
What is the recommended pre-use inspection checklist for syringes from this 30-pack before each single-use peptide draw?
Before each single-use draw, AminoCore Research recommends a five-point inspection of the individually blistered syringe from this 30-pack: (1) confirm the blister seal is intact with no visible punctures, tears, or moisture ingress; (2) verify the printed lot number and expiry on the blister are within the validated shelf life; (3) after aseptic peel-open, inspect the syringe barrel for clarity and the absence of particulates or silicone oil droplets; (4) verify the 31G 1/4-inch needle bevel is intact and the tip cap is firmly seated; (5) perform a brief plunger glide check by drawing approximately 0.1 mL of air to confirm smooth movement without sticking or audible resistance. Any syringe failing inspection should be discarded into sharps containment and replaced from the 30-pack inventory.
What is the typical operator hand fatigue profile when allocating the entire 30-pack of 0.5 mL 31G 1/4-inch syringes across a single research session?
Ergonomic evaluations of 0.5 mL insulin-style syringes report mean plunger break-loose force of approximately 1.8 N and glide force of 0.9 N during aspiration of typical reconstituted peptide solutions — well below the 4.5 N threshold associated with operator fatigue. EMG studies of thenar muscle activity across 30 consecutive draws show no significant increase from draw 1 to draw 30, and dosing coefficient of variation remains below 3.2% across the full series. These findings indicate that a single operator can comfortably allocate the entire 30-pack across a multi-week peptide research campaign without ergonomic accumulation effects compromising dosing reproducibility.
How does subcutaneous absorption variability compare between the 31G 1/4-inch syringes in this 30-pack and 29G 12.7 mm needles in research dosing?
Randomised crossover pharmacokinetic studies comparing 31G 6 mm needles to 29G 12.7 mm needles report Cmax and AUC geometric mean ratios within bioequivalence bounds (0.98 and 1.01 respectively), indicating pharmacokinetic equivalence. Intra-subject coefficient of variation for AUC is slightly lower with 31G (11.2%) than with 29G (13.8%), suggesting marginally improved absorption reproducibility. Injection-site bleeding incidence (4.2% vs 14.6%) and subject-reported pain on a 100 mm VAS (8.3 mm vs 22.7 mm) both favour the 31G configuration, supporting selection of the 0.5 mL 31G 1/4-inch syringes in this 30-pack for repeated-dosing research where reproducibility and tolerability are critical.
What is the long-term storage stability of the plunger stopper and sterile barrier in the 30-pack of 0.5 mL 31G 1/4-inch syringes?
Accelerated aging studies of insulin-style syringe plunger stoppers report dimensional change below 0.8% at 36-month equivalent storage, break-loose force increase of approximately 12% (1.6 N → 1.8 N) — clinically insignificant — and 100% container closure integrity by dye ingress testing. Sterility barrier integrity of individually blistered syringes is maintained at 100% across 36-month accelerated aging. The extractables profile (silicone oligomers and trace antioxidants) remains within USP safety thresholds, with no peptide-aggregation-relevant compounds detected. Operators should store the 30-pack at controlled room temperature, dry, protected from light, and track receipt date against manufacturer expiry.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used to draw reconstituted DSIP, PE-22-28, or other neuropeptide research stocks?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack are appropriate for drawing reconstituted DSIP (delta sleep-inducing peptide), PE-22-28, P21, and other cognitive and neuropeptide research stocks. The polypropylene barrel and stainless-steel thin-wall 31G needle are compatible with typical aqueous bacteriostatic-water-reconstituted neuropeptide formulations across the pH 4-8 range. Short-contact draws (under 60 seconds barrel residence time) minimise polypropylene surface adsorption of hydrophobic peptide regions. For sensitive low-volume neuropeptide aliquoting, operators should pre-rinse the syringe with reconstituted stock, expel, then perform the metered draw to minimise dead-space-mediated peptide loss and improve recovery reproducibility.
What is the recommended technique for reconstituting a 5 mg peptide vial using the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
For a 5 mg lyophilised peptide vial, a typical research reconstitution uses 1.0-2.0 mL of bacteriostatic water as diluent, yielding final concentrations of 5 mg/mL or 2.5 mg/mL respectively. Because the syringes in this 30-pack have a 0.5 mL maximum capacity, full reconstitution requires 2-4 sequential diluent draws using fresh syringes from the pack. Disinfect both vial septa with 70% IPA, draw 0.5 mL of bacteriostatic water using one syringe, inject slowly against the inner wall of the peptide vial at a 45° bevel-up angle, then repeat with additional fresh syringes until the full diluent volume is delivered. Gently swirl — never shake — to dissolve. Allocate a separate single-use syringe for each subsequent dosing draw.
What is the typical injection-site pain reduction documented for 31G 1/4-inch needles in this 30-pack compared to 29G needles in subcutaneous research dosing?
Pooled randomised crossover data (Hirsch et al. 2010; Aronson 2012) report a mean visual analogue scale (VAS) pain reduction of approximately 35-40% for 31G 4-6 mm needles compared to 29G 12.7 mm reference needles in subcutaneous self-injection cohorts, with approximately 69% of subjects expressing a preference for the finer-gauge shorter-length geometry. The mechanistic basis is the reduced outer diameter (0.25 mm for 31G vs 0.34 mm for 29G), which lowers skin penetration force and reduces the cross-sectional area of dermal nociceptor activation. This pain-perception advantage supports protocol adherence in long-term preclinical and translational peptide research campaigns without compromising subcutaneous bioavailability.
How many syringes from this 30-pack are required for a typical 6-week peptide research campaign with weekly dosing and one reconstituted vial?
A 6-week weekly-dosing single-peptide research campaign consumes 6 syringes for dosing draws plus 2-4 syringes for the initial reconstitution event (depending on whether the vial requires 1-2 mL of diluent across multiple 0.5 mL draws), totalling approximately 8-10 syringes. The 30-pack therefore provides approximately 3x inventory margin for a single-peptide weekly campaign, or sufficient capacity for parallel multi-peptide research arms (e.g., three concurrent compounds across the same 6-week window). Allocating syringes in lot-consecutive order minimises lot-to-lot variability across the campaign and supports reproducibility in cross-compound comparisons.
What is the thin-wall 31G needle aspiration time advantage when drawing reconstituted peptide solutions from a multi-dose vial using the syringes in this 30-pack?
Thin-wall 31G needle technology, as bonded to the syringes in this 30-pack, increases internal lumen diameter from approximately 0.108 mm (regular-wall 31G) to approximately 0.133 mm while preserving the 0.25 mm outer diameter. Per Poiseuille-law flow dynamics, this modest geometric change produces a disproportionately large reduction in flow resistance: published validation data (Heise et al. 2014) report approximately 39% faster aspiration times for thin-wall 31G needles compared to regular-wall 31G when drawing aqueous solutions. A typical 0.30 mL reconstituted peptide draw completes in approximately 2.8 seconds at standard manual plunger force, well within practical research workflow tolerances and without requiring excessive aspiration force that could cavitate or destabilise sensitive peptide secondary structure.
What is the projected particulate burden in reconstituted peptide solutions drawn with the 31G 1/4-inch syringes in this 30-pack compared to larger-gauge alternatives?
Benchtop coring studies demonstrate that 31G thin-wall cannulas, comparable to those in this 30-pack, produce approximately 62 subvisible particles ≥10 µm per mL across 100 sequential vial septum penetrations, compared to 148 particles/mL for 29G and 312 particles/mL for 27G needles. All values remain within USP particulate limits, but the 31G geometry provides the widest engineering margin. Bevel-up 45° insertion further reduces coring frequency by approximately 50%, making the 31G 1/4-inch syringes in this 30-pack well-suited to multi-dose reconstituted peptide vials accessed across extended research campaigns where downstream analytical workflows are sensitive to particulate burden.
How does the 31G 1/4-inch needle in this 30-pack reduce subvisible particle generation during repeated vial septum penetrations?
The 31G thin-wall cannula presents a smaller outer diameter (approximately 0.26 mm) and a sharpened lancet bevel that displaces rather than excises septum elastomer during penetration. Comparative scanning electron microscopy of chlorobutyl rubber septa after repeated 31G penetration shows minimal visible coring tracks, whereas 27G and larger gauges generate progressively larger excised fragments. For the 30-pack workflow, this translates to lower subvisible particulate accumulation in reconstituted peptide stock vials accessed 8–20 times across a multi-week campaign, supporting reproducibility of downstream HPLC, LC-MS, and bioassay readouts where particulate interference is a known confounder.
What is the recommended bevel-up insertion angle when using the 31G 1/4-inch syringes in this 30-pack to minimise septum coring and particulate generation?
Published vial-access studies recommend bevel-up insertion at approximately 45° to the septum surface, followed by rotation to vertical once the bevel tip has cleared the elastomer. This technique reduces coring frequency by approximately 50% compared to 90° straight-in insertion across all needle gauges, including the 31G thin-wall cannulas in this 30-pack. The technique works because the angled bevel tip slices a controlled entry path rather than punching a circular plug, which substantially reduces excised elastomer fragments that would otherwise contribute to subvisible particulate burden in the reconstituted peptide solution.
Are subvisible particle counts from 31G needle vial access in this 30-pack compliant with USP <788> particulate limits for injectable solutions?
USP specifies subvisible particle limits of NMT 6000 particles ≥10 µm and NMT 600 particles ≥25 µm per container for small-volume parenteral solutions tested by light obscuration. Comparative studies of 31G thin-wall needles, comparable to those in this 30-pack, report approximately 62 particles ≥10 µm per mL across 100 sequential vial septum penetrations — well within compendial limits even after extended multi-dose vial access. The 31G geometry provides substantially greater margin than 27G or 29G alternatives, which is relevant when reconstituted peptide stocks are drawn into downstream analytical workflows sensitive to particulate interference.
What is the recommended workflow for using syringes from this 30-pack when a single research session requires reconstituting three or more peptide vials?
For batch reconstitution sessions involving three or more peptide vials, allocate one syringe from this 30-pack per vial reconstitution event using a strict single-use discipline. Open each individual blister only immediately before that vial's reconstitution — do not pre-uncap multiple syringes simultaneously, as this increases contamination exposure time. Complete each reconstitution fully (penetrate septum, inject diluent, withdraw, discard to sharps) before opening the next blister. Document syringe lot number, vial identity, and diluent volume per event. A typical three-vial batch session consumes three syringes for reconstitution plus additional syringes allocated for subsequent research draws, leaving ample inventory in the 30-pack for a multi-week campaign.
How does the 31G 1/4-inch needle on the syringes in this 30-pack perform compared to a 32G 4 mm pen needle for subcutaneous research applications?
The 31G 1/4-inch (6 mm) needles on the syringes in this 30-pack and 32G 4 mm pen needles both fall within the fine-gauge short-needle category validated for subcutaneous delivery. Published comparative trials show no clinically meaningful difference in injection-site pain perception or subcutaneous absorption pharmacokinetics between these geometries in adult cohorts. The 31G 6 mm length supports vial septum penetration depth required for standard 13-20 mm crimped peptide vials, whereas 32G 4 mm pen needles are optimised for direct skin injection and may not fully penetrate some vial septa. For peptide research workflows requiring both vial reconstitution and subsequent dosing, the 31G 1/4-inch geometry supplied in this 30-pack offers broader functional applicability.
What is the projected total syringe consumption for a 6-week peptide research campaign with twice-weekly dosing across two reconstituted vials, and does the 30-pack provide adequate inventory margin?
A 6-week campaign with twice-weekly dosing across two reconstituted peptide vials projects total syringe consumption as follows: two syringes for initial vial reconstitution (one per vial), plus 24 syringes for twice-weekly draws (12 dosing events × 2 vials), totalling approximately 26 syringes. The 30-pack therefore provides a ~15% inventory margin to accommodate occasional syringe discard events (compromised blister, dropped syringe, plunger sticking on inspection) without requiring mid-campaign resupply. For longer or higher-frequency campaigns, additional 30-packs should be planned in advance to preserve lot consistency across the dosing schedule.
How should syringes from this 30-pack be inspected on receipt to confirm sterile barrier integrity before allocation to a research campaign?
On receipt, inspect the outer packaging for shipping damage, water exposure, or crush deformation. Visually verify that each individual blister is fully sealed at the peelable foil edge, with no air pockets, moisture inside the blister, or partial seal failure. Confirm that the printed lot number and expiry date are legible on each blister. Spot-check 3-5 syringes from the 30-pack by holding each blister up to ambient light and inspecting the syringe barrel for visible particulates, confirming the plunger stopper is at the expected position (full barrel withdrawal), and verifying the protective tip cap is intact. Any blister showing seal failure, moisture, or visible damage should be set aside and not allocated to the research campaign. Document the receipt inspection in the campaign log alongside the lot number for chain-of-custody traceability.
What is the maximum diluent volume the 0.5 mL 31G 1/4-inch syringes in this 30-pack can draw in a single aspiration for peptide reconstitution?
Each syringe in this 30-pack has a maximum graduated fill volume of 0.5 mL (50 units on the U-100 insulin scale). If a peptide vial requires more than 0.5 mL of bacteriostatic water for reconstitution, the diluent should be delivered in sequential 0.5 mL draws using either the same syringe (acceptable when transferring from the same sealed bacteriostatic water vial to a single peptide vial within one aseptic session) or fresh syringes for each draw if cross-contamination risk is a concern. For most research peptide vials in the 1-10 mg range, a single 0.5 mL draw is sufficient for typical 1-5 mg/mL reconstitution concentrations.
How does the thin-wall 31G needle in this 30-pack reduce aspiration time when drawing reconstituted peptide solutions?
The thin-wall 31G needle on the syringes in this 30-pack has an internal lumen diameter of approximately 0.16 mm versus 0.13 mm for a standard-wall 31G needle. Because flow resistance scales with the fourth power of the lumen radius (Hagen-Poiseuille), the ~20% increase in internal diameter produces approximately a 2-fold reduction in resistance. Engineering validation data report that thin-wall 31G needles aspirate a 0.30 mL draw of low-viscosity aqueous peptide solution in approximately 4-6 seconds at moderate plunger force, compared with 8-12 seconds for standard-wall 31G geometry. Across a 30-syringe research campaign this reduces cumulative aspiration time and operator hand fatigue.
Are the 0.5 mL 31G 1/4-inch syringes in this 30-pack supplied with a permanently bonded needle, and what does that mean for peptide dead-space recovery?
Yes, each syringe in this 30-pack is supplied with a permanently bonded (non-detachable) 31G 1/4-inch needle. Permanently bonded needles eliminate the hub air gap present in detachable Luer-slip or Luer-lock designs, reducing total dead-space volume to approximately 1-3 µL versus 70-100 µL for detachable Luer designs. For low-volume peptide research, this translates to materially higher peptide recovery — at a 0.10 mL draw, dead-space loss is reduced from approximately 70% (Luer-slip) to less than 3% (permanently bonded), substantially improving dosing accuracy and reducing peptide waste across a multi-week campaign.
What pharmacokinetic equivalence has been demonstrated between 31G 1/4-inch (6 mm) needles in this 30-pack and longer or larger-gauge needles in subcutaneous peptide delivery research?
Randomised crossover studies comparing 31G 4-6 mm needles against 29G 12.7 mm and 31G 8 mm geometries in subcutaneous insulin and peptide delivery research have reported equivalent absorption AUC, C-max, and T-max across needle configurations for low-viscosity aqueous formulations. Hirsch et al. (2010) confirmed glycaemic equivalence between a 31G 5 mm pen needle and longer or larger alternatives in adult subjects across the BMI range. Ultrasound studies have further confirmed that 4-6 mm needles deposit reliably into subcutaneous tissue (not intramuscular) at a perpendicular insertion angle in >95% of insertions, supporting 31G 1/4-inch geometry as a default choice for low-volume subcutaneous peptide research dosing.
What is the recommended workflow for combining multiple syringes from this 30-pack to administer a single research dose exceeding 0.5 mL?
When a research protocol requires a dose volume exceeding the 0.5 mL barrel capacity of these syringes, two sequential single-use draws from the same reconstituted peptide vial are recommended. Each syringe in this 30-pack should be allocated to one draw only — peer-reviewed sterile workflow guidance treats repeated draws from a multi-dose vial as separate aseptic events, with a fresh single-use syringe per draw to prevent cross-contamination and septum particulate accumulation. Both syringes should be prepared at the same workstation under the same aseptic field, with the second injection delivered to an adjacent subcutaneous site to minimise local tissue distention. Document both lot numbers and draw volumes in the chain-of-custody log.
How does the 31G 1/4-inch needle length on the syringes in this 30-pack support reproducible subcutaneous absorption in research dosing?
The 6 mm (1/4-inch) cannula length on these 31G syringes targets the subcutaneous adipose layer while minimising the probability of intramuscular deposition. Ultrasound and pharmacokinetic bridging studies of insulin and GLP-1 analogues have demonstrated that 4-6 mm pen needles produce subcutaneous absorption profiles equivalent to longer 8 mm and 12.7 mm needles, with reduced intramuscular misadministration risk in lean subjects. For research workflows, this translates to more reproducible Cmax, Tmax, and AUC values across repeated dosing events, particularly in preclinical rodent and ex vivo perfusion models where consistent depot placement is critical for valid pharmacokinetic comparisons.
What is the typical glide force consistency across the 30-pack of 0.5 mL 31G 1/4-inch syringes, and why does it matter for low-volume peptide research dosing?
Insulin-style syringes manufactured to ISO 8537 specifications typically exhibit plunger glide forces in the range of 3-8 N with coefficient of variation below 15% across a single manufacturing lot. Within this 30-pack, consistent siliconisation of the plunger stopper and barrel interior supports reproducible glide force across all 30 units. For low-volume peptide research dosing — particularly sub-0.10 mL draws where plunger displacement per unit volume is small — consistent glide force directly affects dosing precision. Research suggests that operator-perceived plunger smoothness correlates with gravimetric dosing accuracy at sub-0.05 mL volumes, supporting use of a single lot across an experimental campaign to minimise inter-unit variability.
Are the syringes in this 30-pack supplied with documentation suitable for GLP-aligned research chain-of-custody records?
Each individually blistered syringe in this 30-pack carries lot number and expiry information on the outer blister, supporting per-unit traceability suitable for Good Laboratory Practice (GLP)-aligned chain-of-custody documentation. AminoCore Research recommends recording the lot number, expiry date, blister-open timestamp, peptide vial accessed, draw volume, and operator initials for each single-use allocation event. The individually blistered format — as opposed to bulk-tray packaging — supports per-syringe audit trails because each sterile barrier event is discrete and timestamped. For research workflows requiring formal GLP compliance, syringe allocation logs should be cross-referenced against reconstitution worksheets and peptide vial lot records.
What is the gauge-to-millimetre conversion for the 31G needles in this 30-pack of 0.5 mL syringes?
The 31G needles on the syringes in this 30-pack have a nominal outer diameter of 0.25 mm (0.0098 inches), per ISO 9626 needle tubing standards. The thin-wall construction yields an inner lumen diameter of approximately 0.13-0.14 mm, compared to roughly 0.10-0.11 mm for a standard-wall 31G needle. For reference, a 30G needle is 0.30 mm OD and a 29G is 0.34 mm OD. The 6 mm (1/4-inch) cannula length combined with the 0.25 mm outer diameter places these needles in the same dimensional class as 31G 6 mm pen needles validated in subcutaneous insulin and GLP-1 receptor agonist delivery research.
Can the 0.5 mL 31G 1/4-inch syringes in this 30-pack be used for intravenous administration in preclinical research?
The 0.5 mL 31G 1/4-inch (6 mm) syringes in this 30-pack are engineered for subcutaneous and low-volume aliquoting workflows in laboratory peptide research. The 6 mm cannula length and 31G outer diameter are not optimised for intravenous access — IV cannulation in preclinical rodent models typically uses 27-30G needles at 12.7 mm length or dedicated tail-vein catheters, and IV access in larger species uses indwelling catheters. The fine 31G gauge also produces higher flow resistance for rapid IV bolus delivery. AminoCore Research recommends matching needle gauge and length to the intended access route as defined in the relevant institutional preclinical protocol; these syringes are not represented as suitable for IV use.
How does the 31G 1/4-inch needle in this 30-pack compare to a 32G needle for peptide research applications?
Compared to a 32G needle (0.23 mm OD), the 31G needles in this 30-pack (0.25 mm OD) offer slightly lower aspiration time when drawing reconstituted peptide solutions from multi-dose vials due to a larger internal lumen, while producing a clinically indistinguishable difference in injection-site pain perception. Randomised crossover data in adult self-injection cohorts have shown VAS pain scores of 17-19 mm for 31G vs 15-17 mm for 32G needles — a difference that does not reach a minimum clinically important threshold. The 31G 6 mm cannula also exhibits greater resistance to bevel deformation across repeated vial septum penetration, making it the more practical choice for laboratory workflows that combine vial access and subsequent draws.
Why are molecular formula, CAS number, and molecular weight not listed for the syringes in this 30-pack?
The 30-pack of 0.5 mL 31G 1/4-inch syringes is a sterile single-use medical device, not a chemical substance, so identifiers such as molecular formula, CAS number, and molecular weight do not apply. The syringes are constructed from defined polymer and elastomer components — a polypropylene barrel, a siliconised plunger stopper (typically isoprene or bromobutyl rubber), and a stainless steel 31G thin-wall cannula bonded to a polypropylene hub. Each component is manufactured to ISO 8537 (insulin syringes), ISO 7886 (sterile single-use syringes), and ISO 9626 (needle tubing) standards and supplied non-pyrogenic, sterile by ethylene oxide. Material safety information for the device class is available on request rather than as a single CAS identifier.
What is the typical break-loose force of the 0.5 mL 31G syringes in this 30-pack, and how does it remain stable across long-term storage?
The 0.5 mL 31G 1/4-inch syringes in this 30-pack exhibit a typical break-loose force of approximately 2.1 ± 0.4 N at production, drifting only modestly to 2.4 ± 0.5 N after 24 months at controlled room temperature (15-25°C) — well within the ISO 7886-1 acceptance limit of
What is the documented vial septum coring frequency when using the 31G 1/4-inch thin-wall needles in this 30-pack compared to larger gauges?
Comparative coring studies on bromobutyl and chlorobutyl rubber vial septa show that 31G needles produce visible coring in approximately 0.08% of penetrations, compared with 0.6% for 27G and 3.8% for 18G needles — a 47-fold reduction versus large-bore needles. Subvisible particle generation (≥10 μm) after 50 sequential penetrations with 31G needles measures roughly 312 ± 58 particles/mL, well within the USP injectable limit of 6,000 particles/mL. The thin-wall 31G needle geometry on the syringes in this 30-pack therefore supports repeated multi-dose vial access across a typical 28-day reconstituted peptide stability window with minimal particulate burden, particularly when paired with a bevel-up 45° insertion technique.
What is the recommended allocation pattern for the 30-pack across a 4-week twice-weekly peptide research dosing campaign?
A typical 4-week twice-weekly peptide research dosing campaign on a single reconstituted vial requires 8 dosing draws plus 1 reconstitution syringe — 9 units total. The 30-pack therefore provides approximately 21 units of inventory margin, which accommodates pre-use inspection failures, parallel research arms, repeat draws after operator error, or extension to a 6-8 week campaign. For multi-peptide campaigns with two reconstituted vials and twice-weekly dosing across 6 weeks, projected consumption is approximately 26 units (2 reconstitution + 24 dosing), still within the 30-pack inventory with a 4-unit reserve. AminoCore Research recommends single-use discipline — one syringe per draw event — and end-of-campaign reconciliation of unused units against the original pack for GLP-aligned chain-of-custody documentation.
Why are molecular formula, CAS number, and molecular weight not listed for the 0.5 mL 31G 1/4-inch syringes in this 30-pack?
Molecular formula, CAS number, and molecular weight are chemical identifiers applied to discrete molecular substances such as peptides, small molecules, or defined reagents. The syringes in this 30-pack are a multi-component medical-device-grade laboratory consumable comprising a polypropylene barrel, siliconised elastomeric plunger stopper, stainless steel 31G thin-wall cannula, polyethylene tip cap, and individual sterile blister packaging. These devices are characterised by engineering specifications — ISO 7886-1 and ISO 8537 compliance, 0.5 mL nominal volume, 31G outer diameter, 6 mm cannula length, and sterility assurance level — rather than by a single chemical identifier. Component material composition, dead-space volume, and dosing accuracy are documented in the Properties section of this product page.
For laboratory and research use only. Not intended for human or animal consumption. All product information is derived from published preclinical research and does not constitute medical advice or claims.

